Iron deficiency anemia
Reading File
Finding Sources
Searching PubMed
"iron deficiency anemia"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, authoritative information from multiple medical textbooks. Here is the full, detailed response on Iron Deficiency Anemia:
Iron Deficiency Anemia (IDA)
Iron deficiency is the most common nutritional disorder in the world and the most frequent cause of anemia globally. It affects ~10% of people in high-resource countries and 25-50% in low-resource settings. - Robbins, Cotran & Kumar Pathologic Basis of Disease
Iron Metabolism - Foundation
Understanding IDA requires knowing how iron is handled in the body:
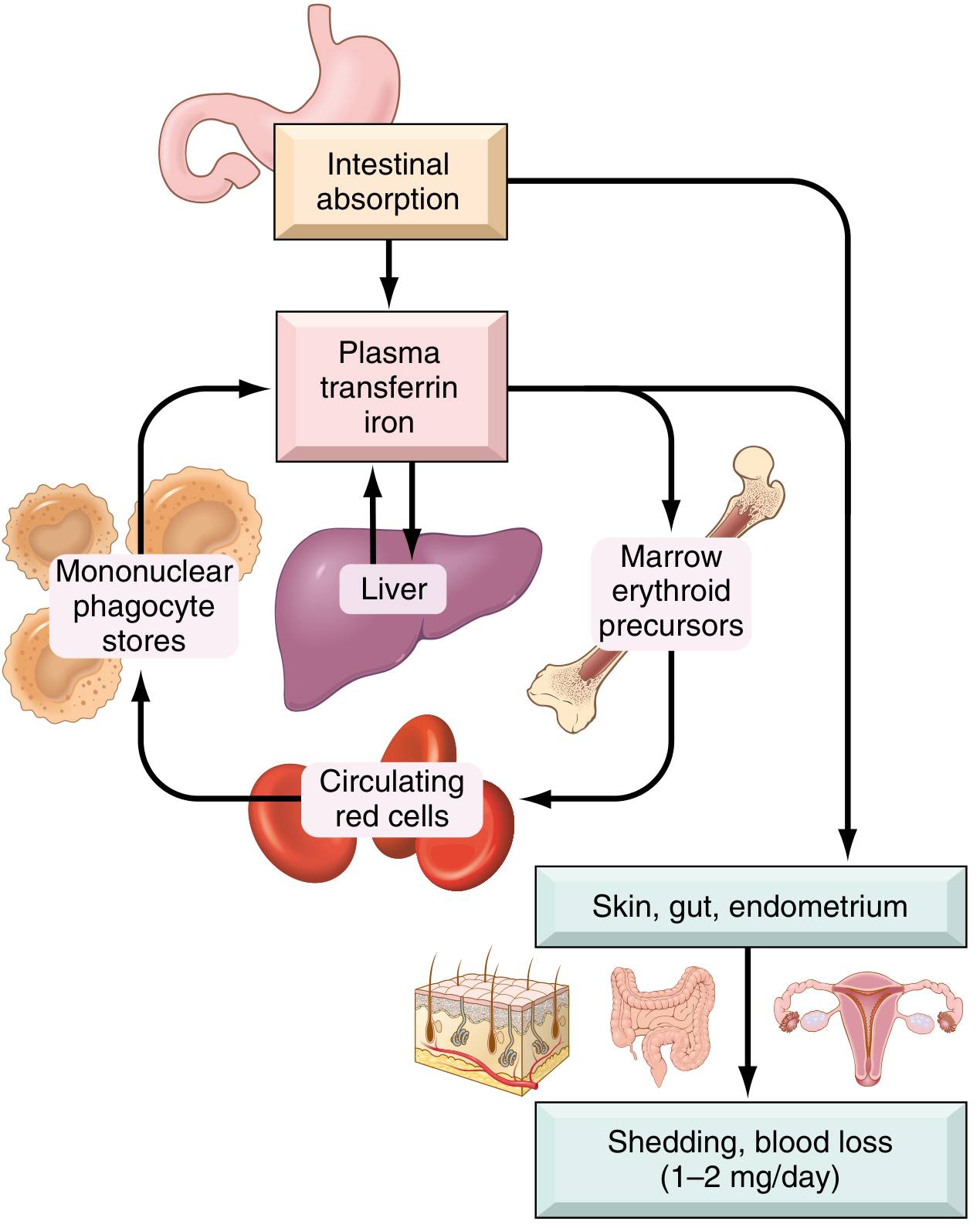
Total body iron distribution (healthy young adults):
| Pool | Males | Females |
|---|---|---|
| Hemoglobin | 2100 mg | 1750 mg |
| Myoglobin | 300 mg | 250 mg |
| Enzymes | 50 mg | 50 mg |
| Storage (ferritin + hemosiderin) | 1000 mg | 400 mg |
| Total | ~3450 mg | ~2450 mg |
- Iron is lost at only 1-2 mg/day via shed epithelial cells. There is no regulated excretory pathway.
- Daily dietary intake in the US: 10-20 mg; only ~20% of heme iron and 1-2% of nonheme iron is absorbed.
- Transferrin is the plasma carrier; normally ~one-third saturated, giving serum iron of ~120 µg/dL (males) and ~100 µg/dL (females). Total iron-binding capacity (TIBC) is normally 300-350 µg/dL.
The key regulator is hepcidin, a liver-derived peptide that inhibits ferroportin (the basolateral iron exporter in enterocytes and macrophages). When iron stores are replete or inflammation is present, hepcidin rises → ferroportin is degraded → iron is trapped in enterocytes and macrophages. When stores are low, hepcidin falls → increased duodenal absorption and iron release from macrophage stores. - Robbins, Cotran & Kumar; Robbins & Kumar Basic Pathology
Etiology and Causes
Iron deficiency arises from four main mechanisms:
1. Dietary Lack
- Rare in high-resource countries where ~2/3 of dietary iron is heme (animal products).
- High-risk groups: infants (breast milk provides only 0.3 mg/L), the impoverished, older adults with restricted diets, and vegans (no heme iron).
- Bioavailability is enhanced by: ascorbic acid, citric acid, amino acids, sugars.
- Bioavailability is reduced by: tannins (tea), carbonates, oxalates, phosphates.
2. Impaired Absorption
- Sprue (celiac disease), fat malabsorption, chronic diarrhea.
- Post-gastrectomy: reduced gastric acidity + rapid transit through duodenum.
3. Increased Requirement
- Infants, children, adolescents (rapid growth).
- Premenopausal women, especially during pregnancy.
- Chronic kidney disease patients on hemodialysis + erythropoietin therapy.
4. Chronic Blood Loss (most common cause in developed countries)
- GI tract (men and postmenopausal women): ulcers, cancers, hookworm infection. In adult males and postmenopausal females, GI blood loss must be presumed until proven otherwise - overlooking this risks missing a GI cancer.
- Uterus: menstrual blood loss (~30 mg iron per cycle); heavy menorrhagia causes significantly more.
- Urinary tract, other sites.
Stages of Progression
Iron deficiency progresses through sequential stages:
- Pre-latent - Storage depletion. Bone marrow iron stores fall; serum ferritin decreases. Hemoglobin and serum iron remain normal.
- Latent - Transport iron depletion. Serum iron falls, TIBC rises, transferrin saturation drops. No anemia yet, but erythroid hyperplasia appears in bone marrow.
- Frank IDA - Iron-deficient erythropoiesis. Anemia appears; microcytic, hypochromic red cells on smear. All iron indices are abnormal. - Robbins, Cotran & Kumar Pathologic Basis of Disease
Morphology
Bone marrow:
- Mild to moderate increase in erythroid progenitors (compensatory erythroid hyperplasia).
- Absence of stainable iron in macrophages - the most diagnostically significant finding; confirmed with Prussian blue stain.
Peripheral blood smear:

- Microcytosis (MCV < 80 fL)
- Hypochromia (MCHC < 30%): zone of central pallor enlarged beyond 1/3 of cell diameter; hemoglobin visible only at the rim.
- Poikilocytosis: characteristic "pencil cells" (small, elongated red cells).
Laboratory Diagnosis
| Test | IDA | Anemia of Chronic Inflammation |
|---|---|---|
| Serum iron | Low (< 30 µg/dL) | Low |
| TIBC | High | Low to normal |
| Transferrin saturation | < 15% (often < 10%) | Low |
| Serum ferritin | Low (< 12 µg/L) | Normal to high |
| Bone marrow iron | Absent | Increased in macrophages |
| Hepcidin | Low | High |
Key distinguishing point: ferritin is low in IDA but high or normal in anemia of chronic inflammation. A low ferritin is essentially diagnostic of IDA; an elevated ferritin does not exclude IDA in the setting of coexisting inflammation (ferritin is an acute-phase reactant).
The transferrin saturation below 15% combined with low serum iron and elevated TIBC is the classic lab triad. - Katzung's Basic and Clinical Pharmacology; Robbins, Cotran & Kumar
Clinical Features
General anemia symptoms: fatigue, pallor, weakness, dyspnea on exertion, palpitations, light-headedness.
Signs specific to severe or long-standing IDA (from iron depletion in non-erythroid tissues):
- Koilonychia - spoon-shaped nails
- Alopecia
- Atrophic glossitis - smooth, painful tongue
- Gastric mucosal atrophy
- Pica - craving for non-food substances (clay) or items like ice (pagophagia) or starch; linked to iron depletion in the CNS
- Intestinal malabsorption
- Plummer-Vinson syndrome (rare triad): microcytic hypochromic anemia + atrophic glossitis + esophageal webs
The dominant symptoms often relate to the underlying cause (GI disease, gynecologic condition, malnutrition, malabsorption). - Robbins, Cotran & Kumar Pathologic Basis of Disease
Workup and Investigation
For adult men and postmenopausal women with confirmed IDA:
- Colonoscopy first, then upper endoscopy + push enteroscopy if colonoscopy negative.
- Duodenal biopsy to screen for celiac disease.
- Test and treat H. pylori if present (reduces iron absorption; can cause microerosions).
- If all three endoscopic procedures are negative: capsule endoscopy.
- Only after negative GI workup: pursue non-GI causes.
For premenopausal women: GI evaluation warranted only after menorrhagia and other obvious gynecologic causes are excluded. - Goldman-Cecil Medicine
Treatment
Oral Iron (first-line for most patients)
Oral iron corrects anemia as rapidly as parenteral iron when GI absorption is intact. Ferrous (Fe²⁺) salts are preferred over ferric forms for better absorption.
| Preparation | Tablet size | Elemental iron/tablet | Usual dose |
|---|---|---|---|
| Ferrous sulfate (hydrated) | 325 mg | 65 mg | 2-4 tabs/day |
| Ferrous sulfate (desiccated) | 200 mg | 65 mg | 2-4 tabs/day |
| Ferrous gluconate | 325 mg | 36 mg | 3-4 tabs/day |
| Ferrous fumarate | 325 mg | 106 mg | 2-3 tabs/day |
- Target: 200-400 mg of elemental iron/day (about 25% is absorbed = 50-100 mg incorporated into Hgb daily).
- Continue treatment for 3-6 months after correcting the underlying cause to replenish stores.
- Response monitoring: reticulocytosis appears in 5-7 days; hemoglobin and red cell indices normalize over weeks.
- GI side effects (nausea, cramps, constipation, diarrhea) are dose-related; can be mitigated by taking with meals or switching to a different ferrous salt. Black stools are expected.
Parenteral Iron (for specific indications)
Reserved for patients who:
- Cannot tolerate or absorb oral iron (malabsorption, post-gastrectomy, IBD involving proximal small bowel)
- Have very high ongoing iron requirements (hemodialysis + erythropoietin)
- Need rapid repletion
Available IV forms:
- Iron dextran (50 mg elemental iron/mL) - can be given as a total-dose infusion; risk of anaphylaxis requires a test dose first.
- Sodium ferric gluconate complex - lower risk of anaphylaxis vs. iron dextran; multiple infusions needed.
- Iron sucrose - low risk; commonly used in CKD patients.
- Ferric carboxymaltose (newer) - high-dose single infusion; favorable safety profile.
Mechanism of safety: ferric iron is stabilized in a carbohydrate shell, allowing slow controlled release and avoiding the toxicity of free ionic iron. - Katzung's Basic and Clinical Pharmacology
Differentiation from Anemia of Chronic Inflammation
This is a common and clinically important distinction:
- Anemia of chronic inflammation (ACI) results from IL-6-driven hepcidin upregulation, which sequesters iron in macrophages and restricts delivery to erythroid precursors.
- Unlike IDA, ACI shows elevated ferritin, elevated storage iron in marrow macrophages, and reduced TIBC.
- Red cells in ACI may be normocytic/normochromic or mildly microcytic/hypochromic.
- Treatment of ACI targets the underlying disease; erythropoietin helps some patients (especially those with cancer). - Robbins, Cotran & Kumar Pathologic Basis of Disease
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease | Robbins & Kumar Basic Pathology | Goldman-Cecil Medicine | Katzung's Basic and Clinical Pharmacology, 16e | Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.