Transport of blood
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I have all the essential content needed. Now I can compile a thorough, well-structured answer on the transport of blood (O2 and CO2 transport), including the key diagrams.
Transport of Blood (O₂ and CO₂)
The "transport of blood" in physiology refers primarily to how blood carries oxygen (O₂) from the lungs to tissues and carbon dioxide (CO₂) from tissues back to the lungs. Both gases are transported by two mechanisms: dissolved in plasma and chemically combined.
I. Transport of Oxygen (O₂)
1. Two Forms of O₂ in Blood
O₂ is carried in blood in two forms:
| Form | Proportion | Mechanism |
|---|---|---|
| Dissolved in plasma | ~2% | Henry's law; proportional to PO₂ |
| Bound to hemoglobin | ~98% | Chemical combination |
Why dissolved O₂ alone is insufficient:
- Solubility of O₂ in blood = 0.003 mL O₂/100 mL blood per mm Hg
- At a normal arterial PO₂ of 100 mm Hg: dissolved O₂ = only 0.3 mL O₂/100 mL blood
- At a resting cardiac output of 5 L/min, this delivers only 15 mL O₂/min
- But the body needs ~250 mL O₂/min at rest - a 17-fold shortfall
- Therefore, hemoglobin binding is essential for adequate O₂ delivery
(Costanzo Physiology 7th Ed; Medical Physiology)
2. Hemoglobin Structure and O₂ Binding
- Normal adult hemoglobin (Hb A) is a tetramer (~68 kDa) with 2α + 2β subunits
- Each subunit contains a heme (iron-porphyrin) group + a globin polypeptide
- Each heme group binds one O₂ molecule → 4 O₂ per Hb molecule
- Iron must be in the ferrous (Fe²⁺) state to bind O₂
- 1 g of hemoglobin A can bind 1.34 mL O₂
- Normal Hb concentration = 15 g/100 mL → O₂-binding capacity = 20.1 mL O₂/100 mL blood
Hemoglobin variants:
| Variant | Feature | Clinical Significance |
|---|---|---|
| HbA (α₂β₂) | Normal adult | - |
| HbF (α₂γ₂) | Fetal; higher O₂ affinity | Facilitates O₂ transfer from mother to fetus |
| HbS (αA₂βS₂) | Deoxygenated form sickles | Sickle cell disease; lower O₂ affinity |
| Methemoglobin | Fe³⁺ (ferric) | Cannot bind O₂; caused by nitrites/sulfonamides |
(Costanzo Physiology 7th Ed)
3. O₂ Content of Blood
The O₂ content (actual O₂ per 100 mL blood) is calculated as:
O₂ content = (O₂-binding capacity × % Saturation) + Dissolved O₂
- Normal arterial blood (98% saturated): O₂ content ≈ 20.0 mL O₂/100 mL
- O₂ delivery = Cardiac output × O₂ content
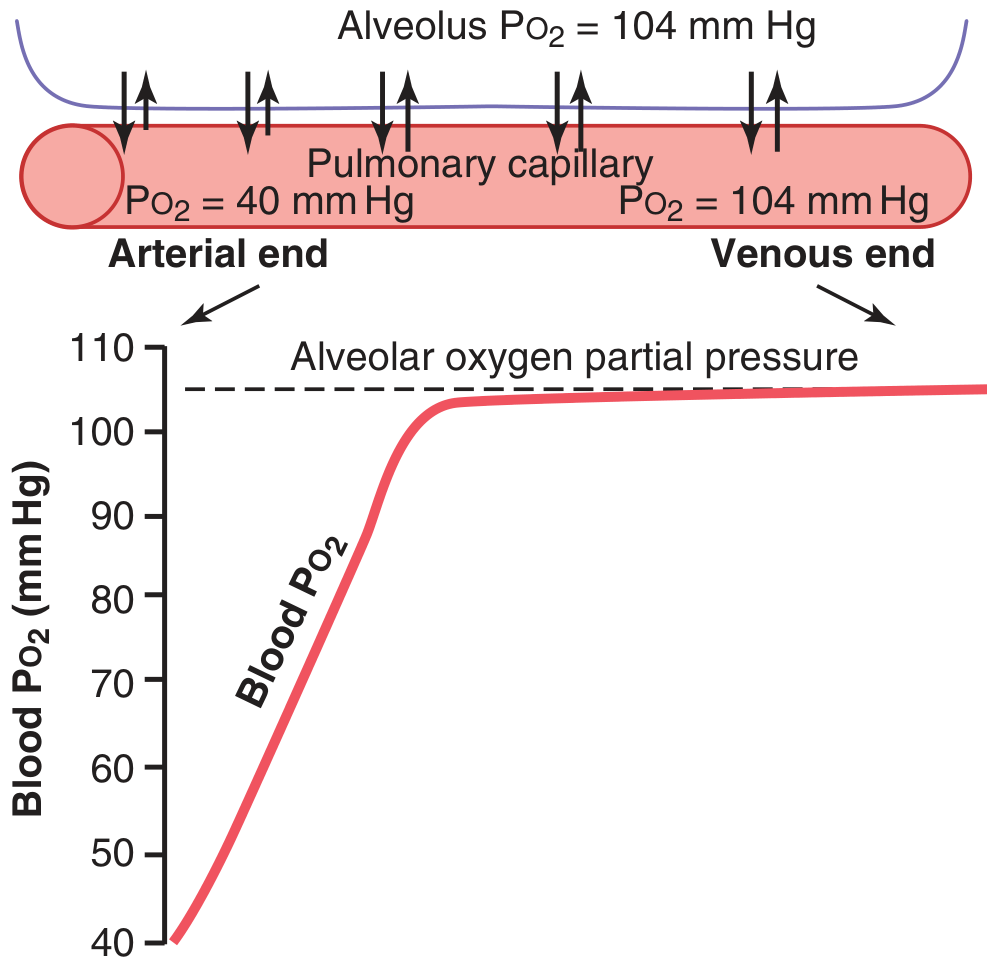
4. Diffusion of O₂: Alveoli → Blood → Tissues
At the lungs (alveolar capillaries):
- Alveolar PO₂ = 104 mm Hg
- Venous blood entering pulmonary capillary PO₂ = 40 mm Hg
- Pressure gradient = 64 mm Hg → drives O₂ into blood rapidly
- Blood reaches near-equilibrium (~104 mm Hg) after only 1/3 of capillary length
Venous admixture ("shunt"):
- ~2% of blood passes through bronchial circulation (unexposed to alveolar air), PO₂ ≈ 40 mm Hg
- This mixes with oxygenated blood → aortic PO₂ drops slightly to ~95 mm Hg
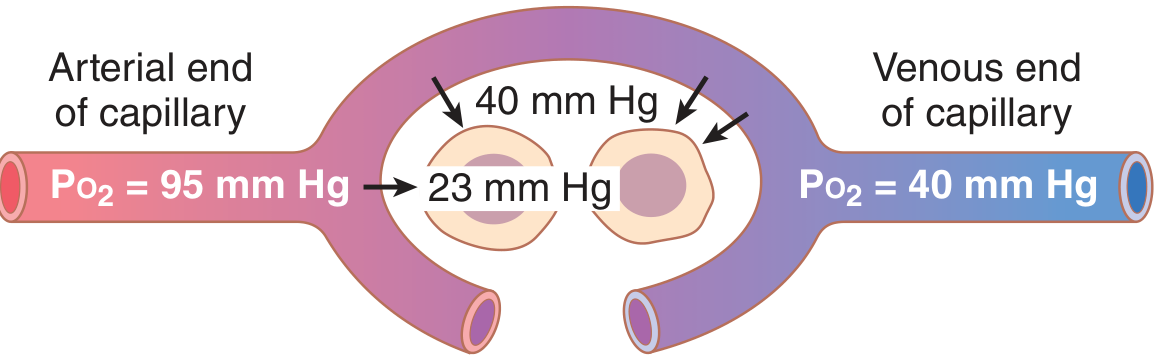
At the tissues (peripheral capillaries):
- Arterial blood arrives at PO₂ = 95 mm Hg
- Interstitial fluid PO₂ = 40 mm Hg
- Intracellular PO₂ = ~23 mm Hg (or even lower near mitochondria)
- O₂ diffuses down this gradient into cells
(Guyton & Hall Textbook of Medical Physiology)
5. Factors Affecting O₂-Hemoglobin Dissociation (Bohr Effect)
The oxyhemoglobin dissociation curve describes the sigmoidal relationship between PO₂ and Hb saturation:
Right shift (decreased O₂ affinity, more O₂ released to tissues):
- ↑ PCO₂
- ↑ [H⁺] (acidosis / ↓ pH) - Bohr effect
- ↑ Temperature
- ↑ 2,3-DPG (diphosphoglycerate)
Left shift (increased O₂ affinity, O₂ held tighter):
- ↓ PCO₂
- ↓ [H⁺] (alkalosis / ↑ pH)
- ↓ Temperature
- Fetal hemoglobin (HbF)
- CO poisoning (carboxyhemoglobin)
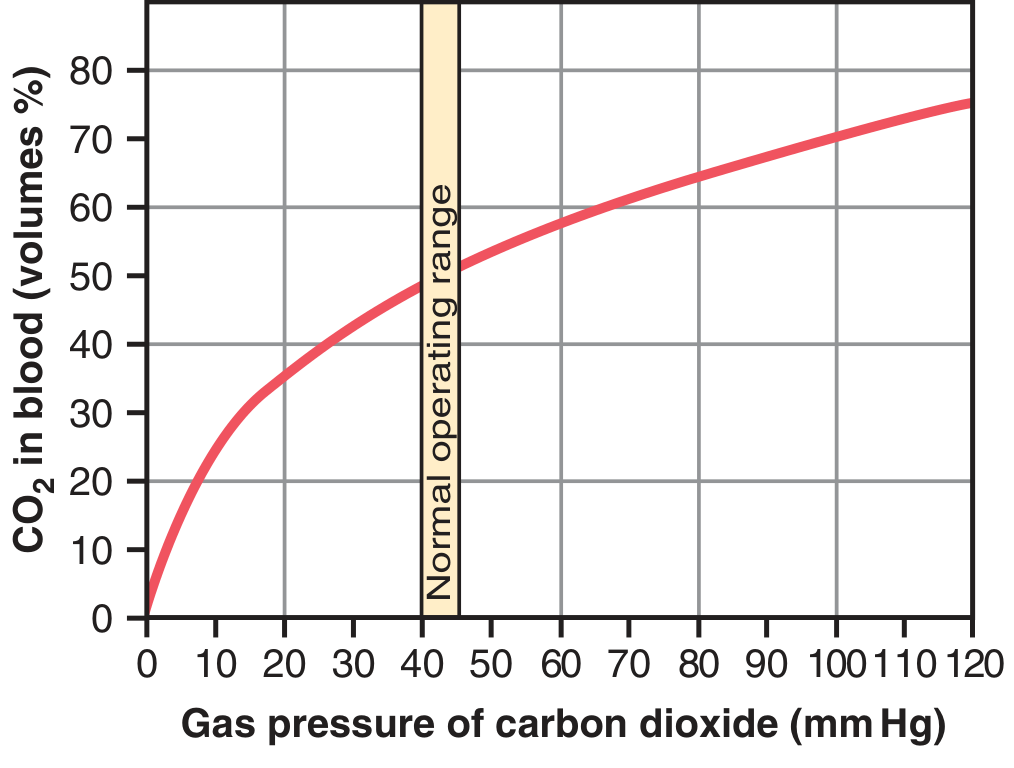
II. Transport of Carbon Dioxide (CO₂)
CO₂ is produced by cellular metabolism and must be carried from tissues to lungs. Average transport: 4 mL CO₂ per 100 mL blood. CO₂ is transported in three forms:
1. Dissolved CO₂ (~7%)
- PCO₂ venous = 45 mm Hg; arterial = 40 mm Hg
- Dissolved CO₂ at 45 mm Hg = 2.7 mL/100 mL; at 40 mm Hg = 2.4 mL/100 mL
- Difference = 0.3 mL/100 mL transported this way
2. As Bicarbonate Ion (HCO₃⁻) - the MAJOR form (~70%)
This is the most important mechanism, driven by carbonic anhydrase inside RBCs:
CO₂ + H₂O →[carbonic anhydrase]→ H₂CO₃ → H⁺ + HCO₃⁻
- Carbonic anhydrase accelerates this reaction 5,000-fold
- H⁺ ions are buffered by hemoglobin inside RBCs
- HCO₃⁻ diffuses out of RBCs into plasma in exchange for Cl⁻ (chloride shift / Hamburger phenomenon)
- The venous RBC thus has higher chloride content than arterial RBC
Importance: Blocking carbonic anhydrase (e.g., acetazolamide) raises tissue PCO₂ to ~80 mm Hg (vs. normal 45 mm Hg)
3. Carbaminohemoglobin (~20-30%)
- CO₂ binds directly to amine (-NH₂) groups on hemoglobin → carbaminohemoglobin (CO₂Hb)
- Reaction is reversible; CO₂ released easily in alveoli where PCO₂ is lower
- A small amount also binds to plasma proteins (less significant - only 1/4 the protein mass of Hb)
| Form | % of CO₂ Transported |
|---|---|
| Dissolved CO₂ | ~7% |
| Bicarbonate (HCO₃⁻) | ~70% |
| Carbaminohemoglobin | ~20-23% |
(Guyton & Hall Textbook of Medical Physiology)
The Haldane Effect
Oxygenation of Hb in the lungs displaces CO₂ - this is the reverse of the Bohr effect:
- When O₂ binds to Hb in alveolar capillaries, Hb releases CO₂ more readily
- This increases CO₂ unloading from blood to alveolar air
- The Haldane effect is actually quantitatively more important than the Bohr effect in enhancing gas exchange
III. Summary: The Full Transport Cycle
LUNGS
Alveolar PO₂ = 104 mm Hg → O₂ loads onto Hb
Alveolar PCO₂ = 40 mm Hg → CO₂ unloads from blood
↓
ARTERIAL BLOOD
PO₂ = 95 mm Hg
PCO₂ = 40 mm Hg
O₂ content ≈ 20 mL/100 mL
↓
TISSUES
Interstitial PO₂ = 40 mm Hg → O₂ unloads from Hb
Intracellular PCO₂ rises → CO₂ loads into blood
↓
VENOUS BLOOD
PO₂ = 40 mm Hg
PCO₂ = 45 mm Hg
CO₂ content rises ~4 mL/100 mL
↓
Back to LUNGS
Key numbers to remember:
| Parameter | Arterial | Venous |
|---|---|---|
| PO₂ | 95 mm Hg | 40 mm Hg |
| PCO₂ | 40 mm Hg | 45 mm Hg |
| O₂ content | ~20 mL/100 mL | ~15 mL/100 mL |
| Hb O₂ saturation | ~98% | ~75% |
Sources:
- Guyton and Hall Textbook of Medical Physiology (Chapter 41)
- Costanzo Physiology, 7th Edition
- Medical Physiology (Boron & Boulpaep)
This is a shared conversation. Sign in to Orris to start your own chat.