Varicose veins examination
Reading File
Finding Sources
Searching the Web
varicose veins clinical examination techniques tests
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have all the material needed for a comprehensive answer. Let me compile the full response.
Varicose Veins - Clinical Examination
Varicose veins are tortuous, dilated superficial veins most commonly affecting the lower limb. A systematic clinical examination is structured around history, inspection, palpation, and a set of specific clinical tests to determine the site and level of valvular incompetence.
History
Key questions to ask:
- Onset and duration - when did the veins first appear?
- Symptoms - aching, heaviness, throbbing, or itching in the legs (worse at end of day / after standing)
- Complications - swelling, skin changes, ulceration, superficial thrombophlebitis
- Precipitating factors - prolonged standing, occupation
- Obstetric history (women) - number of pregnancies, any "white leg" (phlegmasia alba dolens) during pregnancy, oral contraceptive use (increases DVT risk)
- Abdominal symptoms - constipation, pelvic mass (secondary varicose veins)
- Past history - any previous injection treatment or surgery for varicose veins; previous illness or surgery that may have caused deep vein thrombosis (DVT)
- Family history - varicose veins have a strong hereditary component
- S Das A Manual on Clinical Surgery, p. 105
Inspection
The patient should stand (ideally on a raised platform) in good light, with both lower limbs fully exposed.
1. The Varicose Veins Themselves
- Note which system is involved:
- Long (great) saphenous vein (LSV): tortuous dilated trunk on the medial side of the leg, from in front of the medial malleolus upward along the medial side of the thigh to the saphenous opening (groin)
- Short (small) saphenous vein (SSV): from behind the lateral malleolus, up the posterior aspect of the leg to the popliteal fossa
- Note distribution, extent, and severity
2. Swelling
- Localized - varicose segment, saphena varix (at groin - can mimic femoral hernia), or superficial thrombophlebitis
- Generalized - suggests deep vein thrombosis (DVT)
3. Skin Changes
Look for:
- Colour: local redness (thrombophlebitis), brown pigmentation (haemosiderin deposition) around the medial malleolus, white patches - atrophie blanche
- Eczema / lipodermatosclerosis - induration and inflammation of lower leg skin
- Phlebectasia corona - fan-shaped intradermal veins near ankle/foot
- Ulceration - shallow, irregular-bordered venous ulcer near medial malleolus (most common site)
- Scars from previous surgery or injection
- S Das A Manual on Clinical Surgery, p. 105-106; Harrison's 22E, p. 2223
Palpation
1. Temperature
- Compare both limbs - varicose veins may feel warm; DVT limb is also warm
2. Consistency of the Veins
- Soft and compressible when patient lies down
- Firm and tense on standing
3. Saphena Varix
- A soft swelling at the saphenofemoral junction (groin) that disappears on lying down
- Transmits a fluid thrill on tapping the varicose veins lower in the thigh
- A cough impulse can be felt here (if SFJ is incompetent)
4. Tenderness
- Present along the vein in superficial thrombophlebitis
- Tenderness of calf muscles suggests DVT (Homan's sign - now considered unreliable)
5. Oedema
- Pitting oedema around the ankle - note severity
6. Fascial Gaps (Fegan's Method)
- With patient standing, mark points of maximum bulge
- Lie patient down, elevate limb, then palpate along the line of varicosities for gaps or pits in the deep fascia - these indicate sites of incompetent perforators
- S Das A Manual on Clinical Surgery, p. 106-108
Percussion (Auscultation)
Tap / Schwartz Test (Percussion Test)
- Place one hand over the saphena varix at the groin (or over the upper part of the long saphenous vein)
- Tap the varicose vein lower down the thigh with the other hand
- A fluid thrill transmitted upward confirms continuity of the venous trunk (patent, uninterrupted column of blood)
- Also: tapping the lower long saphenous vein - an impulse felt at the saphenous opening indicates SFJ incompetence
- S Das A Manual on Clinical Surgery, p. 108; Pye's Surgical Handicraft 22nd Ed., p. 376
Special Clinical Tests
These tests determine:
- The level of valvular incompetence (superficial vs. communicating)
- Patency of the deep venous system
1. Brodie-Trendelenburg Test
The most important test for varicose veins.
Technique:
- Patient lies supine; leg is elevated to drain the varicose veins (milking proximally speeds this up)
- Compress the saphenofemoral junction with the thumb or apply a tourniquet just below the SFJ
- Ask the patient to stand quickly
- Observe:
- Keep compression on for 1 minute (without releasing): Gradual slow filling of veins from below = incompetent perforating/communicating veins (positive test - part 1)
- Then release the compression: Rapid filling from above downward = incompetent saphenofemoral valve (positive test - part 2)
Interpretation:
| Result | Interpretation |
|---|---|
| Veins fill rapidly on release of tourniquet | SFJ incompetence (primary varicose veins) |
| Veins fill slowly while tourniquet maintained | Incompetent perforating/communicating veins |
| Filling occurs both ways | Combined SFJ + communicating incompetence |
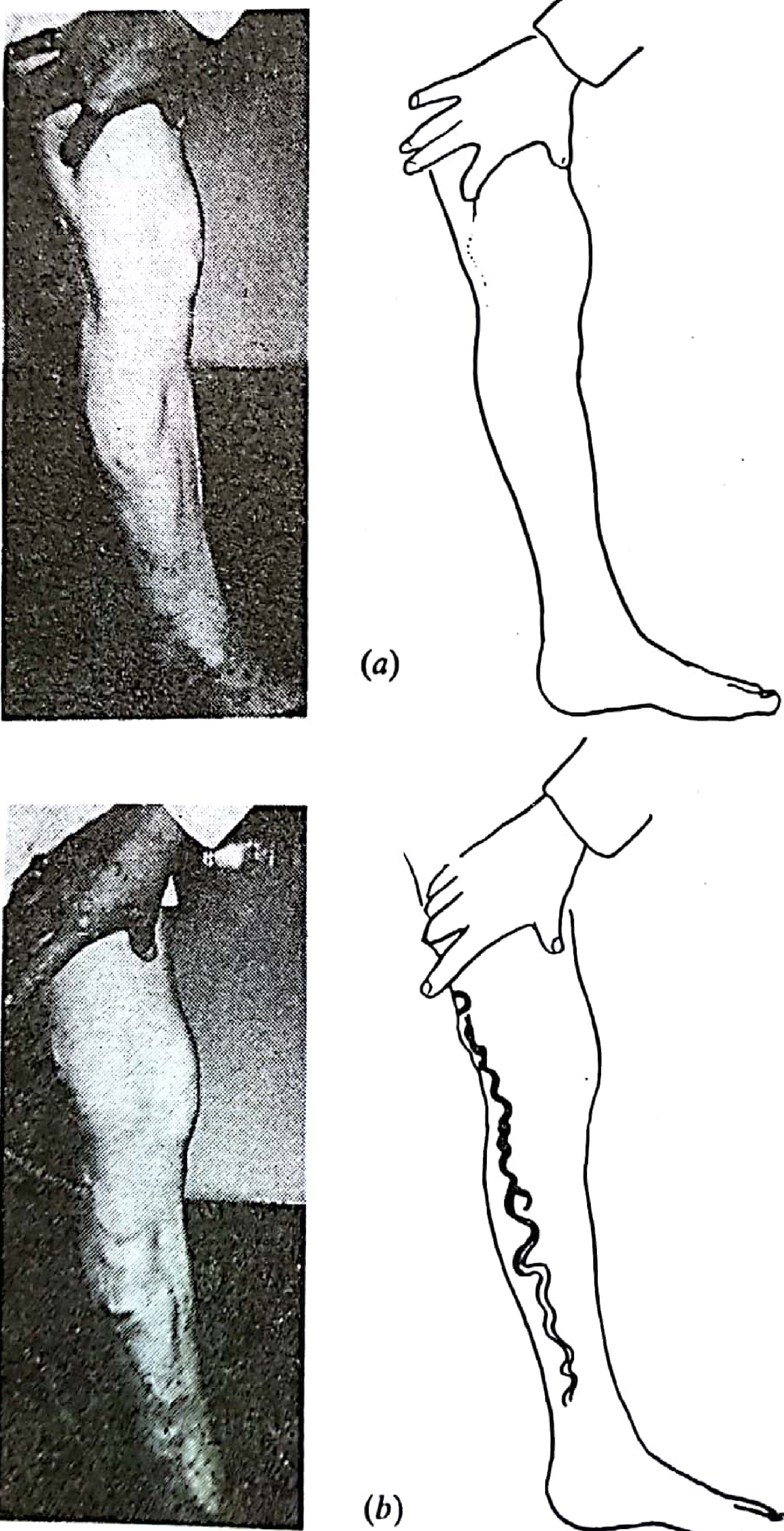
Figure: Trendelenburg's test. (a) Digital compression of main saphenous vein - no refilling; (b) release of compression allows incompetent downward filling - Pye's Surgical Handicraft 22nd Ed.
- S Das A Manual on Clinical Surgery, p. 107; Pye's Surgical Handicraft 22nd Ed., p. 376; Harrison's 22E, p. 2224
2. Tourniquet Test (Multiple Tourniquet Test)
Purpose: Identifies the exact level of incompetent perforating/communicating veins.
Technique:
- Empty the superficial veins by elevating the leg
- Apply a tourniquet at the upper thigh (just below SFJ)
- Ask the patient to stand
- If veins below tourniquet remain empty → SFJ is the only site of incompetence
- If veins below tourniquet fill → incompetent perforators exist below the tourniquet
- Move tourniquet progressively down the leg in steps to locate the exact level
Key perforator sites in LSV system:
- Saphenofemoral junction (most important)
- Mid-thigh perforator
- Lower thigh perforator
- Medial lower leg perforators (Cockett's perforators)
- S Das A Manual on Clinical Surgery, p. 107
3. Perthes Test
Purpose: Assesses patency of the deep venous system.
Technique:
- Apply a tourniquet at the mid-thigh with the patient standing (veins are full)
- Ask the patient to walk briskly for 5 minutes
- Observe varicose veins below the tourniquet:
| Result | Interpretation |
|---|---|
| Veins collapse (shrink) | Deep veins and communicating veins are patent and functional - safe to operate |
| Veins remain same or distend further | Deep venous obstruction present - surgery is contraindicated |
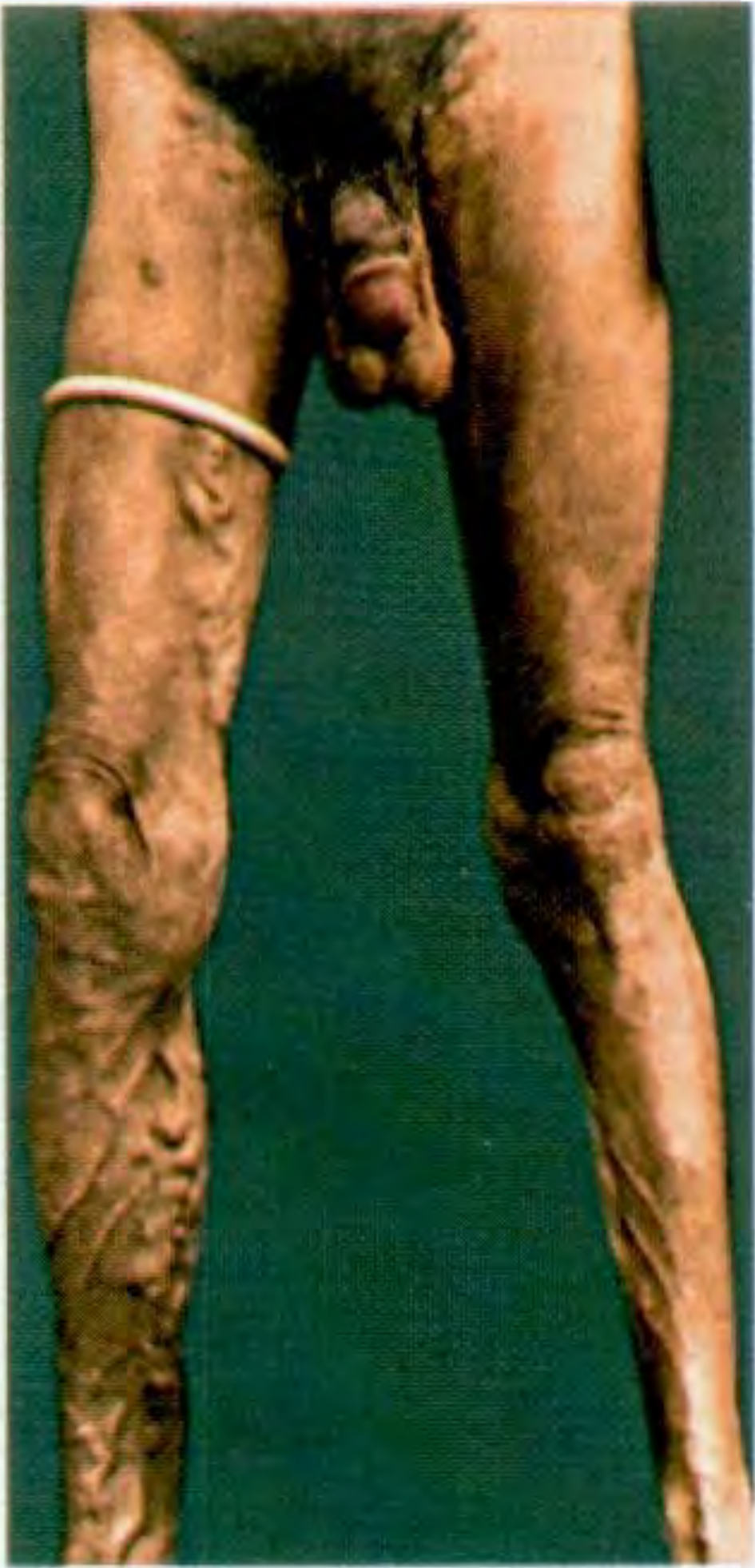
Figure: Performing Perthes' test - S Das Manual on Clinical Surgery
This is the most important pre-operative test - operating on varicose veins when the deep system is occluded is dangerous and will worsen symptoms.
- S Das A Manual on Clinical Surgery, p. 108; Harrison's 22E, p. 2224
4. Morrissey's Cough Impulse Test
Purpose: Detects SFJ incompetence.
Technique:
- Elevate limb to empty varicose veins
- Place limb back on the couch
- Ask the patient to cough forcibly
- Place fingers at the saphenous opening (groin)
Positive result: An expansile impulse is felt at the saphenous opening - indicates incompetent saphenofemoral valve. A bruit may be heard on auscultation at the same point.
- S Das A Manual on Clinical Surgery, p. 108
5. Schwartz Test (Tap Test / Percussion Test)
Purpose: Confirms continuity of the venous trunk.
Technique:
- One hand placed over the SFJ/saphena varix
- Other hand taps the varicose vein at a lower level
- A transmitted fluid impulse felt superiorly = patent, uninterrupted column of blood in the vein
- S Das A Manual on Clinical Surgery, p. 108
6. Pratt's Test
Purpose: Locates the sites of incompetent perforating veins.
Technique:
- Apply Esmarch elastic bandage from toes to groin (emptying veins)
- Apply tourniquet at groin
- Remove the elastic bandage from below
- Reapply it from the groin downward
- Observe: at each incompetent perforator, a "blow-out" or visible varix appears between the two bandages
- S Das A Manual on Clinical Surgery, p. 108
7. Fegan's Method (Locating Perforators)
Technique:
- Mark bulge sites on the leg while patient stands
- Lie the patient down and elevate the limb to empty veins
- Palpate along the varicosity line - identify gaps or pits in the deep fascia (these are the perforator entry points)
- Mark them for surgery
- S Das A Manual on Clinical Surgery, p. 108
Summary of Tests
| Test | What it detects | How performed |
|---|---|---|
| Brodie-Trendelenburg | SFJ incompetence & communicating vein incompetence | Elevate leg, tourniquet at groin, patient stands; release and observe filling |
| Multiple Tourniquet | Level of incompetent perforators | Tourniquet moved down leg in steps |
| Perthes | Deep vein patency | Mid-thigh tourniquet, patient walks 5 min |
| Morrissey's Cough Impulse | SFJ incompetence | Cough with finger at saphenous opening |
| Schwartz/Tap | Continuity of venous trunk | Tap lower vein, feel impulse at groin |
| Pratt's | Sites of perforators | Double bandage technique |
| Fegan's | Fascial defects at perforators | Palpation for gaps in deep fascia |
CEAP Classification
The CEAP (Clinical, Etiologic, Anatomic, Pathophysiologic) system is used to classify chronic venous disease severity:
| Class | Features |
|---|---|
| C0 | No visible or palpable signs |
| C1 | Telangiectasias / reticular veins |
| C2 | Varicose veins |
| C3 | Oedema |
| C4a | Pigmentation or eczema |
| C4b | Lipodermatosclerosis or atrophie blanche |
| C5 | Healed venous ulcer |
| C6 | Active venous ulcer |
- Harrison's 22E, p. 2224
Investigations
- Hand-held Doppler: Simple, quick - detects reflux at SFJ and sapheno-popliteal junction. Note: clinical tests alone are inaccurate; Doppler is now the minimum standard.
- Duplex ultrasound: Gold standard - maps the anatomy of both superficial and deep systems, identifies exact sites of reflux and perforator incompetence. Mandatory before any intervention.
- Venography: Rarely needed now; reserved for complex/recurrent cases
- Pye's Surgical Handicraft 22nd Ed., p. 376; Bailey & Love 28th Ed.
Key Complications to Look For
- Superficial thrombophlebitis (tender, red, indurated vein)
- Venous eczema and lipodermatosclerosis
- Venous ulceration (medial malleolus - most common)
- Haemorrhage from varicosity
- Saphena varix (may mimic femoral hernia)
- Pye's Surgical Handicraft 22nd Ed., p. 376
Note: Modern practice has largely moved away from bedside clinical tests (which have limited accuracy) in favor of hand-held Doppler and duplex ultrasound for planning treatment. The clinical tests remain important for examinations and for understanding the anatomy of incompetence. As noted by a PMC validation study, clinical tests for varicose veins are inaccurate, and hand-held Doppler assessment is more reliable.
This is a shared conversation. Sign in to Orris to start your own chat.