Cipap and bipap
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Excellent - I now have comprehensive data from five major textbooks. Let me compile the full answer.
CPAP vs BiPAP - Non-Invasive Positive Pressure Ventilation
Both CPAP and BiPAP are forms of Non-Invasive Positive Pressure Ventilation (NIPPV/NPPV) - meaning they deliver respiratory support via a mask rather than an endotracheal tube.
Definitions
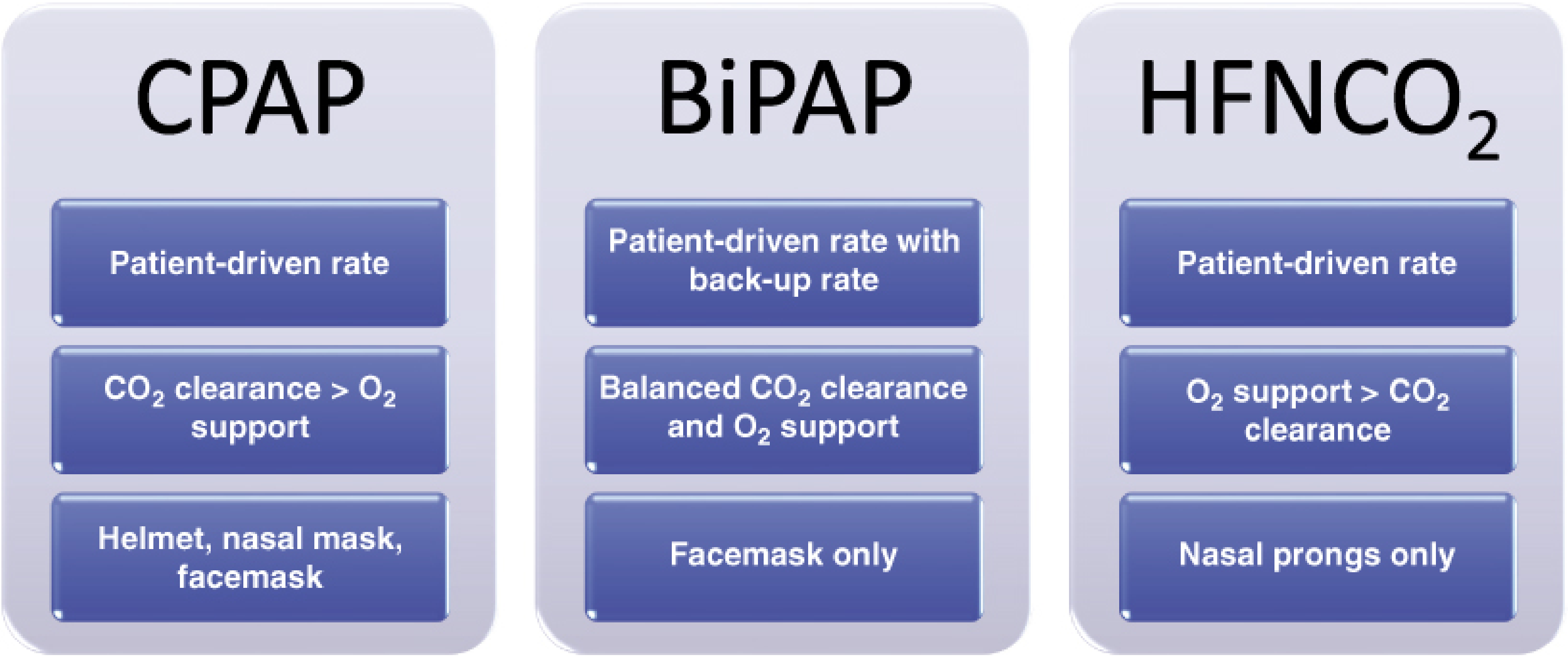
CPAP - Continuous Positive Airway Pressure
- Delivers a single, constant pressure throughout the entire respiratory cycle (both inspiration and expiration)
- The pressure level is equivalent to PEEP (Positive End-Expiratory Pressure)
- Patient-driven rate - completely relies on the patient's own respiratory effort and drive
- No extra pressure boost during inhalation
- Delivered via: helmet, nasal mask, or full facemask
BiPAP - Bilevel Positive Airway Pressure
- Delivers two different pressure levels:
- IPAP (Inspiratory Positive Airway Pressure) - higher pressure during inhalation
- EPAP (Expiratory Positive Airway Pressure) - lower pressure during exhalation (equivalent to PEEP)
- The IPAP-EPAP difference = pressure support (analogous to PS in invasive ventilation)
- Patient-driven rate with a backup rate - newer devices can be set to cycle between pressures at a minimum rate even if the patient fails to initiate a breath
- Delivered via: facemask only
Key Physiological Effects
| Effect | Mechanism |
|---|---|
| Alveolar recruitment | Increased pressure keeps alveoli open at end-expiration (PEEP effect) |
| Improved V/Q matching | Opens atelectatic areas, improves gas exchange surface area |
| Reduced work of breathing | IPAP (BiPAP) and PEEP (both) reduce inspiratory effort by 60% |
| Decreased preload | Increased intrathoracic pressure reduces venous return |
| Decreased afterload | Reduced transmural pressure aids LV emptying - especially beneficial in pulmonary edema |
| PEEP negation in auto-PEEP | Externally applied PEEP reduces inspiratory threshold load in COPD/asthma |
BiPAP provides both CO2 clearance AND oxygenation support (balanced). CPAP favors CO2 clearance over oxygenation.
Indications
CPAP Indications
- Obstructive Sleep Apnea (OSA) - primary chronic use
- Acute cardiogenic pulmonary edema - well-evidenced reduction in intubation rate
- Mild-moderate hypoxemic respiratory failure
- Post-operative atelectasis
- Bridge therapy in selected hypoxic patients
BiPAP Indications
- Acute exacerbation of COPD - strongest evidence; reduces intubation, length of stay, and in-hospital mortality (should be started early, not after medical therapy failure)
- Acute cardiogenic pulmonary edema
- Neuromuscular disease with respiratory failure (e.g., ALS, myasthenia gravis)
- Obesity Hypoventilation Syndrome (OHS) - preferred when patient cannot tolerate high CPAP levels
- Hypercapnic respiratory failure of any cause
- Patients who fail CPAP
- Bridge to intubation in impending respiratory failure
- DNR/DNI patients - as ceiling-of-care respiratory support
(Roberts and Hedges' Clinical Procedures in Emergency Medicine, Box 8.2; Tintinalli's Emergency Medicine)
Starting Settings
| Parameter | CPAP | BiPAP |
|---|---|---|
| Starting pressure | 5-15 cm H2O | IPAP 8-12 cm H2O / EPAP 4-5 cm H2O |
| Titration goal | Relieve obstruction, improve SpO2 | Reduce RR, reduce dyspnea, improve SpO2, lower PaCO2 |
| Backup rate | Not available | Set on BiPAP S/T (Spontaneous/Timed) mode |
(Tintinalli's Emergency Medicine)
Contraindications (Both)
- Altered mental status / inability to protect airway - risk of aspiration if vomiting occurs
- Apnea (CPAP specifically, as it has no backup rate)
- Neuromuscular blockade - both modes require an open glottis and intact respiratory drive
- Copious secretions (patient must be able to cough and clear)
- Facial fractures or trauma preventing mask seal
- Recent esophageal, gastric, or duodenal anastomoses (positive pressure can insufflate the GI tract and stress anastomoses)
- Hemodynamic instability
- Inability to cooperate (delirium)
- Bacterial pneumonia is a relative contraindication for BiPAP - the high mask pressures make it very difficult to expectorate sputum and reduce bacterial bioburden
Advantages Over Invasive Mechanical Ventilation
- Avoids ETT-related complications (VAP, airway/lung injury)
- Preserves upper airway defense mechanisms
- Patient can speak, eat, clear secretions when mask removed
- Less sedation required
- Shorter hospital stay
- Reduced mortality in appropriate populations (especially COPD exacerbation)
(Roberts and Hedges; Sabiston Textbook of Surgery)
Important Practical Notes
- Tightness of mask seal is critical for effectiveness - leaks reduce delivered pressure
- Do NOT use physical restraints on patients wearing NIV masks - they must be able to remove the mask if they vomit
- Standard ventilators set to NIPPV mode have additive IPAP + EPAP (total delivered = sum). Standalone BiPAP units have independent IPAP/EPAP (set IPAP = delivered IPAP)
- CPAP is appropriate in the right patient for COVID-19 (including helmet CPAP)
- Early initiation in COPD exacerbation is key - late initiation after failed medical therapy eliminates the mortality benefit
Summary Comparison
| Feature | CPAP | BiPAP |
|---|---|---|
| Pressure levels | 1 (continuous) | 2 (IPAP + EPAP) |
| Respiratory rate | Patient-driven | Patient-driven + backup rate option |
| Primary effect | Oxygenation / recruitment | Both O2 + CO2 clearance |
| CO2 clearance | Limited | Good |
| Best for | OSA, cardiogenic pulmonary edema | COPD exacerbation, hypercapnic failure, neuromuscular disease |
| Interface | Nasal mask, facemask, helmet | Facemask only |
| Sedation/NMB | Contraindicated | Contraindicated |
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine; Fischer's Mastery of Surgery 8th ed; Sabiston Textbook of Surgery; Tintinalli's Emergency Medicine; Miller's Anesthesia 10th ed
This is a shared conversation. Sign in to Orris to start your own chat.