Neurological assessment
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have enough material from authoritative textbooks to provide a thorough, comprehensive answer. Let me compile it.
Neurological Assessment
A complete neurological assessment examines every region of the nervous system in a systematic way. In practice, a full examination is often compressed into a screening exam supplemented by a focused exam based on the presenting complaint.
1. Approach and Principles
The neurological examination begins during the history, before formal testing even starts. Observe the patient from the moment they walk in:
- Facial expression: reduced (hypomimia - parkinsonism/depression), astonished (progressive supranuclear palsy)
- Ptosis: suggests myasthenia gravis or brainstem lesion
- Speech quality: dysarthria, aphasia, spasmodic dysphonia
- Involuntary movements at rest: tremor, dystonia, chorea
The exam serves two goals: confirm or refute the diagnostic hypothesis from the history, and localize the lesion within the nervous system.
"Both the presence and absence of abnormalities may be of diagnostic importance." - Bradley and Daroff's Neurology in Clinical Practice
2. Mental Status
Assessed largely during history-taking, but formal testing includes:
| Domain | Assessment |
|---|---|
| Level of consciousness | Alert, drowsy, stuporous, comatose |
| Orientation | Person, place, time, situation |
| Attention | Digit span, serial 7s |
| Language | Fluency, comprehension, naming, repetition |
| Memory | Immediate, short-term, long-term |
| Visuospatial | Clock drawing, copy figures |
| Executive function | Abstraction, judgment, planning |
For altered consciousness, use validated scales:
- Glasgow Coma Scale (GCS) - most widely used; scores Eye (1-4), Verbal (1-5), Motor (1-6)
- FOUR Score - better for intubated patients; scores Eye, Motor, Brainstem reflexes, Respiration (each 0-4)
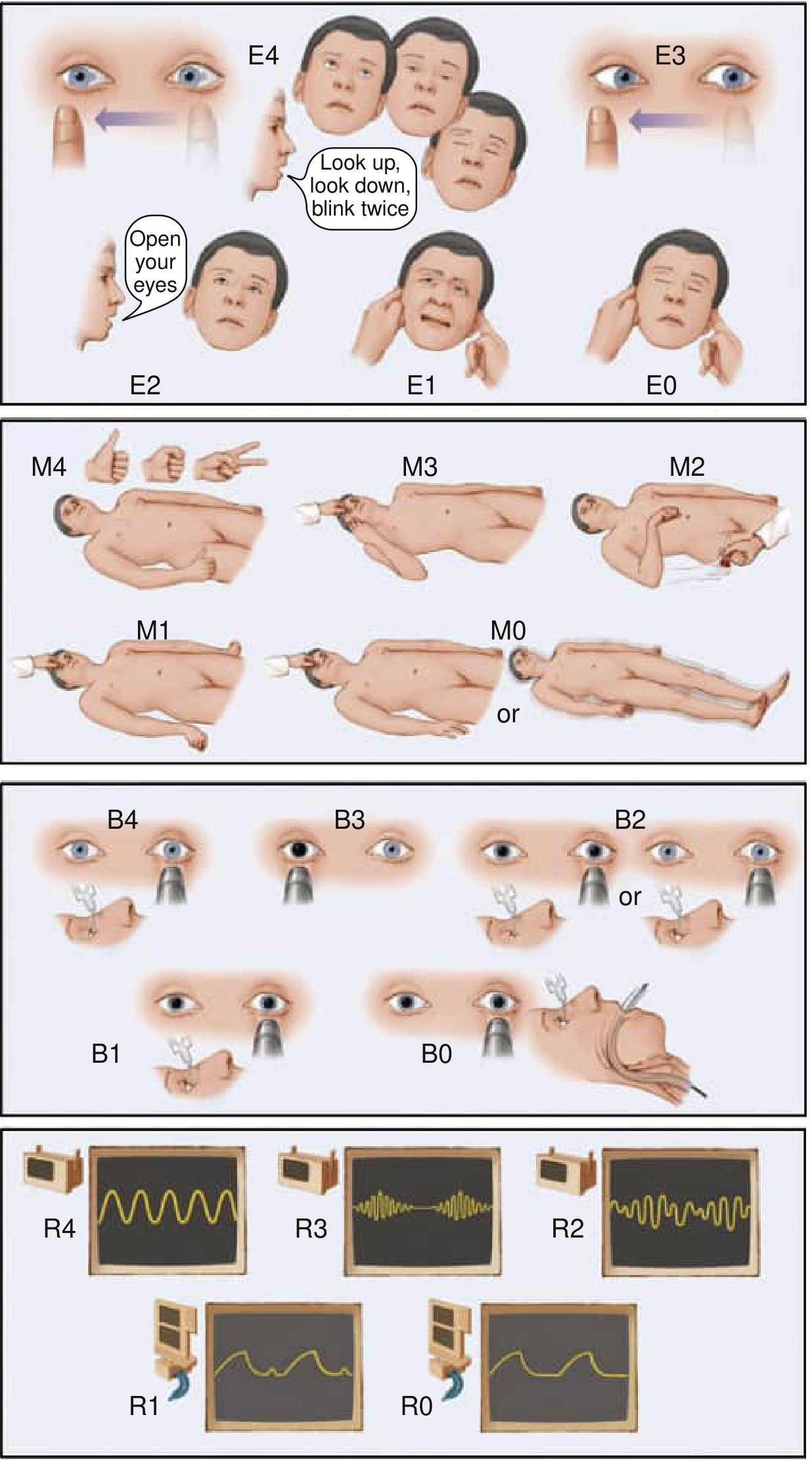
FOUR Score components:
- E (Eye): E4 = tracking + blinking to command; E3 = open, not tracking; E2 = opens to voice; E1 = opens to pain; E0 = no opening
- M (Motor): M4 = thumbs up/fist/peace sign; M3 = localizes; M2 = flexion; M1 = extension; M0 = no response
- B (Brainstem): B4 = pupillary + corneal present; B3 = one pupil fixed; B2 = either reflex absent; B1 = both absent; B0 = absent + cough reflex gone
- R (Respiration): R4 = regular; R3 = Cheyne-Stokes; R2 = irregular; R1 = above ventilator rate; R0 = at vent rate or apnea
3. Cranial Nerve (CN) Examination
Test in numerical order; group CNs III, IV, VI together.
Screening minimum: fundi, visual fields, pupil size/reactivity, extraocular movements, facial movements.
| CN | Name | Key Tests |
|---|---|---|
| I | Olfactory | Identify coffee/toothpaste with eyes closed (test only if head trauma, Parkinson's, or frontal lobe disease suspected) |
| II | Optic | Visual acuity (Snellen chart); visual fields by confrontation (4 quadrants); fundoscopy (disc, vessels, retina); swinging flashlight test for relative afferent pupillary defect (RAPD) |
| III, IV, VI | Oculomotor, Trochlear, Abducens | Pupil size, shape, direct + consensual light reflex, accommodation; extraocular movements (H-pattern); nystagmus at 45 deg - hold for a few seconds |
| V | Trigeminal | Pinprick + light touch in V1/V2/V3 territories; corneal reflex (cotton wisp - tests V afferent, VII efferent); jaw clench (masseter) |
| VII | Facial | At rest + spontaneous expression; forehead wrinkling, eye closure, smile, cheek puff. Lower 2/3 weakness only = UMN; entire side = LMN |
| VIII | Vestibulocochlear | Whispered voice or finger-rub each ear; Rinne (air vs bone) and Weber (lateralization) with 512 Hz tuning fork |
| IX, X | Glossopharyngeal, Vagus | Palatal movement ("Ah"); gag reflex; voice quality (hoarseness) |
| XI | Accessory | Sternocleidomastoid (head turn against resistance); trapezius (shoulder shrug) |
| XII | Hypoglossal | Tongue protrusion (deviates toward weak side); fasciculations; dysarthria |
Pupillary Findings - Localizing Value:
- Reactive, symmetric throughout toxic-metabolic coma = structural cause unlikely
- Asymmetric pupils: distinguish which side is abnormal; compressive CN III lesion dilates the pupil (parasympathetics on outside compress first)
- Horner syndrome (ptosis, miosis, anhidrosis): sympathetic pathway disruption
- Pinpoint pupils + ICU setting: pontine hemorrhage/infarct (stimulates parasympathetics)
- Eye deviation: "look toward a stroke, look away from a seizure" (hemispheric); opposite rule for pontine lesions
4. Motor Examination
Inspection
- Bulk (atrophy, hypertrophy)
- Fasciculations (lower motor neuron sign)
- Involuntary movements (tremor, chorea, dystonia, myoclonus)
Tone
- Flaccidity = LMN or acute UMN ("spinal shock")
- Spasticity (velocity-dependent, clasp-knife) = UMN (corticospinal tract)
- Rigidity (lead-pipe, cogwheel) = basal ganglia (parkinsonism)
Strength - MRC Scale
| Grade | Description |
|---|---|
| 0 | No contraction |
| 1 | Flicker/trace contraction |
| 2 | Active movement with gravity eliminated |
| 3 | Active movement against gravity |
| 4 | Active movement against resistance (reduced) |
| 5 | Normal power |
Screening maneuver: Arms extended in supination in front of body, eyes open (assess drift, tremor, dystonia) then eyes closed (assess proprioception). A weak arm shows pronator drift (downward + pronation).
Reflexes - Grading Scale
| Grade | Response |
|---|---|
| 0 | Absent |
| 1+ | Diminished |
| 2+ | Normal |
| 3+ | Brisk (may indicate UMN) |
| 4+ | Clonus (definite UMN) |
Key pathological reflexes:
- Babinski sign (extensor plantar response): great toe dorsiflexes + fan of other toes = UMN lesion
- Hoffman's sign: UMN lesion in upper limbs
- Absent abdominal reflexes: UMN lesion ipsilaterally
Standard reflexes to test: Biceps (C5-6), brachioradialis (C5-6), triceps (C7), knee/patellar (L3-4), ankle/Achilles (S1-2), plantar response
5. Sensory Examination
Five primary modalities, derived from two anatomic pathways:
| Modality | Pathway | Testing |
|---|---|---|
| Pain | Spinothalamic (lateral) | New pin or pinwheel |
| Temperature | Spinothalamic (lateral) | Cold/warm tuning fork |
| Light touch | Both | Cotton wisp, finger |
| Vibration | Dorsal column (medial) | 128 Hz tuning fork on distal phalanx |
| Joint position sense (proprioception) | Dorsal column (medial) | Grasp digit laterally; small 1-2 mm excursions |
Romberg test: Stand feet together, eyes open then closed. Falling with eyes closed (positive Romberg) = dorsal column/proprioceptive loss (not cerebellar).
Cortical sensation (requires intact primary sensation):
- Two-point discrimination
- Stereognosis (identify object by touch alone)
- Graphesthesia (identify numbers written on skin)
- Double simultaneous stimulation (extinction = parietal lobe lesion contralaterally)
6. Coordination Examination
Tests cerebellar and basal ganglia function; must interpret in context of motor and sensory findings.
| Test | Technique | Abnormality |
|---|---|---|
| Finger-nose-finger | Touch own nose, then examiner's moving finger alternately | Intention tremor, dysmetria = cerebellar |
| Rapid alternating movements (dysdiadochokinesia) | Fist, extend index finger, tap thumb rapidly | Imprecise/irregular = cerebellar; slow = pyramidal |
| Heel-knee-shin | Slide heel from knee down contralateral shin | Dysmetria, ataxia |
| Foot tapping | Tap foot rapidly on floor | Slow = pyramidal; arrhythmic = cerebellar |
7. Gait Examination
"Watching the patient walk is the most important part of the neurologic examination." - Harrison's Principles of Internal Medicine 22E
Observe: normal walk, heel-walking, toe-walking, tandem (heel-to-toe), Romberg.
| Gait Pattern | Lesion / Cause |
|---|---|
| Hemiplegic (circumduction, arm adducted) | Contralateral UMN (stroke) |
| Spastic-scissors (stiff, crossing) | Bilateral UMN (spinal cord) |
| Steppage (high steps, foot drop) | LMN / peroneal nerve |
| Waddling (pelvis drops) | Proximal muscle weakness (myopathy) |
| Cerebellar ataxic (wide-base, staggering) | Cerebellar disease |
| Sensory ataxic (wide-base, stamping, worse dark) | Dorsal column / peripheral neuropathy |
| Parkinsonian (shuffling, stooped, reduced arm swing, festination) | Basal ganglia |
| Apraxic (magnetic, short steps, feet stick) | Frontal lobe / NPH |
A patient who can walk tandem gait does not have significant cerebellar or proprioceptive deficit. A patient who can walk on toes, heels, and do a pushup has normal limb strength.
8. Screening Neurological Examination (Summary Table)
Adapted from Bradley and Daroff's Neurology in Clinical Practice:
| Component | Key Maneuver |
|---|---|
| Mental status | Assessed during history |
| CN I | Only if indicated (head trauma, Parkinson's) |
| CN II | Acuity, fields, fundoscopy, RAPD |
| CN III/IV/VI | Eye movements, pupils, nystagmus |
| CN V | Facial sensation, corneal reflex |
| CN VII | Eye closure, smile symmetry |
| CN VIII | Whisper test each ear |
| CN IX-XII | Gag, palate, tongue, shoulder shrug |
| Motor | Drift test; tone; bulk |
| Reflexes | Biceps, triceps, knee, ankle, plantar |
| Sensation | Pin, vibration, proprioception distally |
| Coordination | Finger-nose-finger, rapid alternating |
| Gait | Normal, tandem, toe/heel walking |
9. Localization Framework
The neurological examination is designed to localize the lesion:
| Location | Key Signs |
|---|---|
| Cerebral cortex | Contralateral hemiparesis (face = arm > leg), aphasia, neglect, cortical sensory loss, seizures |
| Internal capsule | Dense contralateral hemiparesis + hemisensory loss (face = arm = leg equally) |
| Brainstem | Ipsilateral CN deficit + contralateral hemiparesis (crossed signs) |
| Cerebellum | Ipsilateral limb ataxia, nystagmus, dysarthria, wide-base gait |
| Spinal cord | Level-based motor + sensory loss; Brown-Sequard (ipsilateral motor/proprioception loss + contralateral pain/temp loss) |
| Anterior horn cell | LMN signs only: weakness, wasting, fasciculations, hyporeflexia |
| Peripheral nerve | Distal > proximal, mixed motor + sensory, loss of reflexes |
| Neuromuscular junction | Fatigable weakness, ptosis, diplopia |
| Muscle | Proximal > distal weakness, no sensory loss, preserved reflexes until late |
Sources: Bradley and Daroff's Neurology in Clinical Practice; Harrison's Principles of Internal Medicine 22E (2025); Goldman-Cecil Medicine International Edition
This is a shared conversation. Sign in to Orris to start your own chat.