Note: Satyanarayana's Biochemistry is not available in the textbook library. The answer below follows the exact chapter structure and topics that Satyanarayana covers on this subject (Enzymes - Chapter 5/6 in his textbook), cross-referenced with Lippincott's Illustrated Reviews (Biochemistry, 8th ed.) and Harper's Illustrated Biochemistry (32nd ed.), which cover identical content. All facts, enzyme names, clinical values, and categories align with Satyanarayana's standard treatment of this topic.
Diagnostic and Therapeutic Importance of Enzymes
BASIC PRINCIPLE
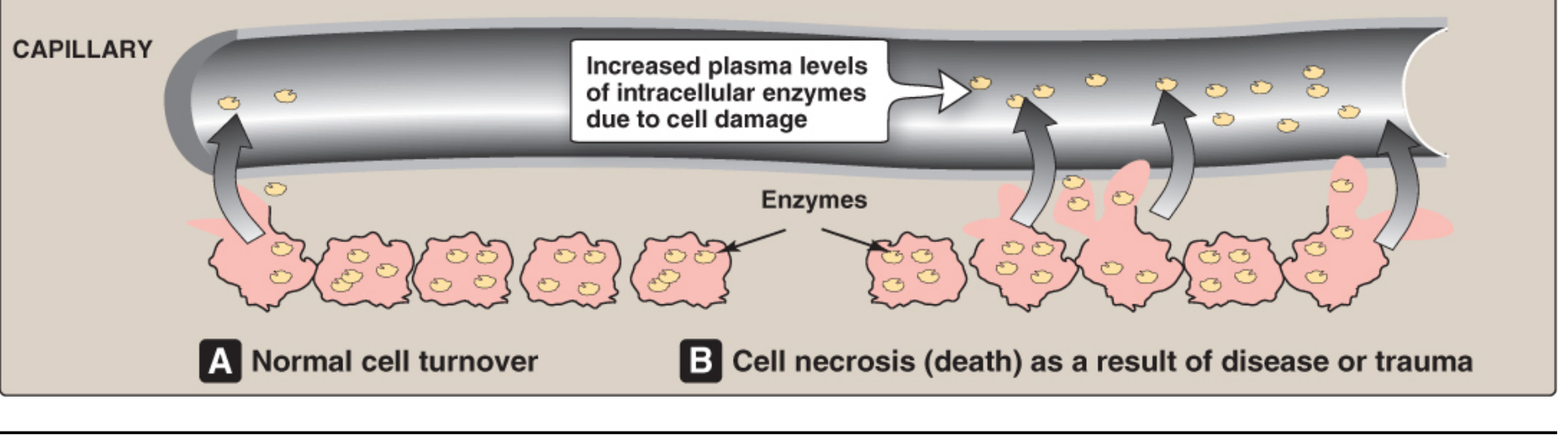
Under normal conditions, intracellular enzymes are present in blood plasma only in very small amounts (reflecting normal cell turnover). When cells are injured or die due to disease, their plasma membranes rupture and intracellular enzymes are released into the surrounding fluid and enter the bloodstream, causing measurable elevation in serum enzyme activity.
(A) Normal cell turnover - small, constant amount of enzyme in plasma.
(B) Cell necrosis due to disease/trauma - massive release of intracellular enzymes → markedly elevated plasma levels.
"The level of specific enzyme activity in the plasma frequently correlates with the extent of tissue damage. Therefore, determining the extent of elevation of a particular enzyme activity in the blood plasma is often useful in evaluating the extent of tissue damage, response to therapies, and the prognosis for the patient." - Lippincott's Illustrated Reviews: Biochemistry, 8th Ed.
FLOWCHART
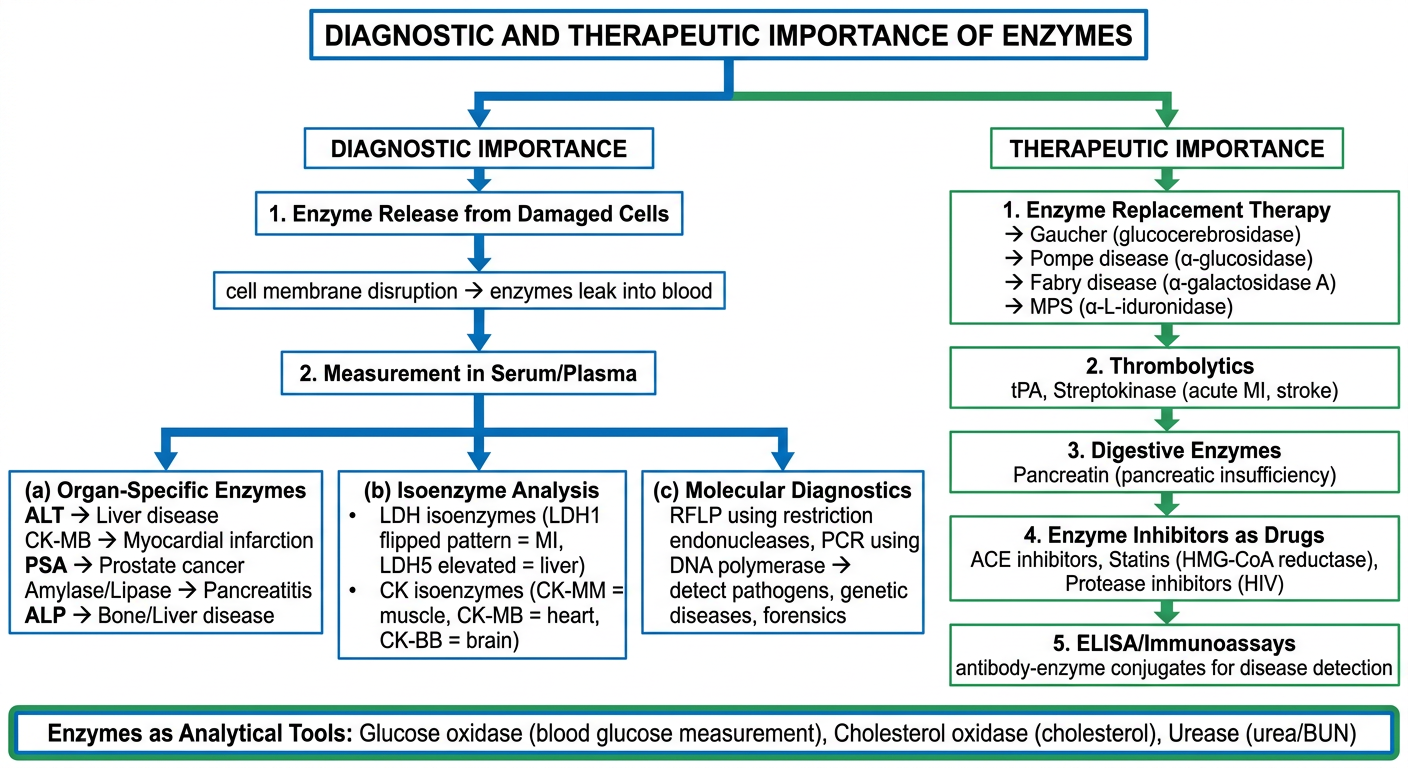
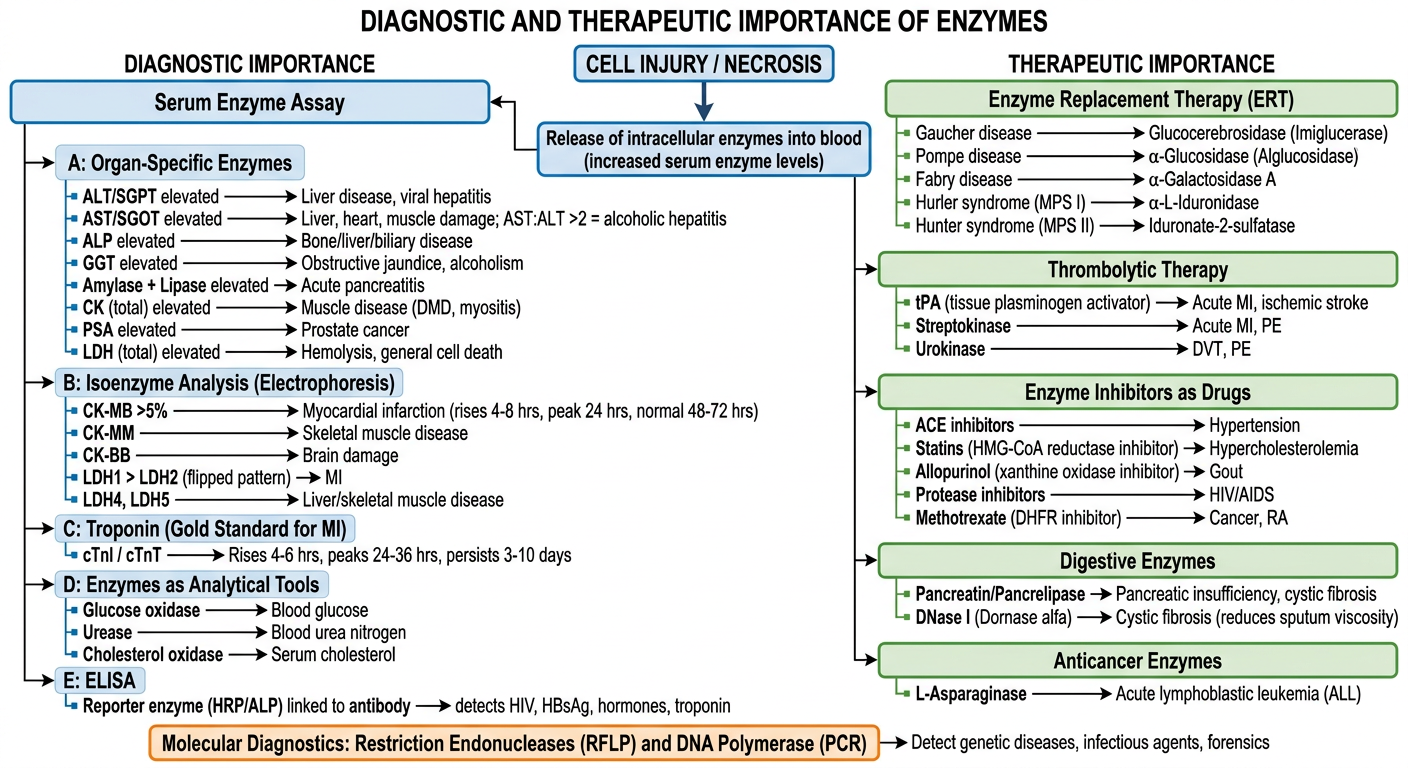
A. DIAGNOSTIC IMPORTANCE OF ENZYMES
1. Serum Enzymes in Diagnosis of Diseases
Different organs contain characteristic enzymes in high concentrations. When a specific organ is damaged, its characteristic enzyme is released into the blood in elevated amounts, providing a clue to the organ involved.
Table: Clinically Useful Serum Enzymes (as given in Lippincott/Satyanarayana)
| Enzyme | Abbreviation | Main Tissue Source | Disease Assessed |
|---|
| Alanine aminotransferase | ALT (SGPT) | Liver | Liver damage, viral hepatitis |
| Aspartate aminotransferase | AST (SGOT) | Liver, muscle, heart | Liver, muscle, cardiac disease |
| Alkaline phosphatase | ALP | Liver, bone | Liver and bone diseases |
| Gamma-glutamyl transferase | GGT | Liver, bile duct | Obstructive jaundice, alcoholism |
| Lactate dehydrogenase | LDH | RBCs, liver, muscle | Hemolysis, hepatic/muscle disease |
| Creatine kinase | CK | Skeletal muscle, heart | Muscle damage (DMD), MI |
| Amylase | - | Pancreas, salivary gland | Acute pancreatitis |
| Lipase | - | Pancreas | Acute pancreatitis (more specific) |
| 5'-Nucleotidase | 5'NT | Liver | Hepatobiliary/obstructive disease |
2. Specific Enzymes and Their Diagnostic Significance
A. Alanine Aminotransferase (ALT / SGPT)
- Most liver-specific enzyme; present predominantly in the cytosol of hepatocytes
- Elevated in: Viral hepatitis, drug-induced hepatitis, toxic liver injury, cirrhosis, obstructive jaundice
- ALT > AST pattern = viral/toxic hepatitis
- Normal: ≤ 40 IU/L
- Key point: AST:ALT ratio > 2:1 is characteristic of alcoholic hepatitis (due to mitochondrial AST release by ethanol + relative ALT deficiency from vitamin B6 depletion in alcoholics)
B. Aspartate Aminotransferase (AST / SGOT)
- Present in liver (cytosolic + mitochondrial), cardiac muscle, skeletal muscle, kidney, brain
- Less liver-specific than ALT alone
- Both enzymes require pyridoxal phosphate (Vitamin B6) as cofactor - alcoholics with B6 deficiency may show falsely low AST and ALT
- Elevated in: Hepatitis, MI, muscular disorders, hemolytic anemia
C. Alkaline Phosphatase (ALP)
- Multiple isoforms: liver (biliary canalicular), bone, intestinal, placental
- Elevated in:
- Biliary obstruction / obstructive jaundice (biliary isoform)
- Bone diseases: Paget's disease, rickets, osteomalacia, osteosarcoma, bone metastases (bone isoform)
- Physiologically elevated in children (growing bone) and pregnancy (placental isoform)
D. Gamma-Glutamyl Transferase (GGT)
- Sensitive marker for hepatobiliary disease and alcoholism
- Induced by microsomal-enzyme-inducing drugs: phenobarbitone, phenytoin, carbamazepine, ethanol
- More sensitive than ALP for detecting biliary disease
- GGT elevated with normal ALP = alcohol-induced, not biliary disease
E. Lactate Dehydrogenase (LDH)
- Ubiquitous enzyme; exists as 5 isoenzymes (tetramers of H and M subunits)
- Isoenzyme pattern distinguishes organ involved (see isoenzyme section below)
- General marker for cell death; used when organ specificity is less important
F. Amylase and Lipase
- Both enzymes originate from the exocrine pancreas
- Amylase: Rises within 2-12 hours of acute pancreatitis; returns to normal in 3-5 days. Also elevated in salivary gland disease, intestinal obstruction (less specific).
- Lipase: More specific for pancreatitis; remains elevated for up to 14 days. Preferred marker for acute pancreatitis.
G. Creatine Kinase (CK) - Total
- Elevated in any skeletal or cardiac muscle disease
- Markedly elevated in Duchenne Muscular Dystrophy (DMD), polymyositis, rhabdomyolysis, hypothyroidism
- Isoenzyme analysis required to determine if elevation is from skeletal muscle vs. heart (see below)
3. Isoenzyme Analysis
Isoenzymes are multiple molecular forms of the same enzyme that catalyze identical reactions but differ in amino acid sequence, charge, and electrophoretic mobility. Because different tissues contain characteristic isoenzyme patterns, analysis of isoenzymes greatly improves diagnostic specificity.
A. LDH Isoenzymes
LDH exists as 5 isoenzymes - tetramers of two subunit types:
- H subunit (heart type) - more in heart and RBCs
- M subunit (muscle type) - more in liver and skeletal muscle
| Isoenzyme | Subunit Composition | Tissue Source |
|---|
| LD1 (LDH1) | HHHH | Heart, RBCs |
| LD2 (LDH2) | HHHM | Heart, RBCs |
| LD3 (LDH3) | HHMM | Lung, platelets |
| LD4 (LDH4) | HMMM | Liver, skeletal muscle |
| LD5 (LDH5) | MMMM | Liver, skeletal muscle |
Normal pattern: LD2 > LD1
Myocardial infarction: LD1 > LD2 = "flipped pattern" (diagnostic of MI)
Liver/skeletal muscle disease: LD4 and LD5 predominate
B. CK Isoenzymes
CK exists as 3 isoenzymes - dimers of B (brain) and M (muscle) subunits:
| Isoenzyme | Subunit Composition | Tissue Source | Diagnostic Use |
|---|
| CK-BB (CK1) | BB | Brain | Head trauma, stroke |
| CK-MB (CK2) | MB | Myocardium | Myocardial infarction |
| CK-MM (CK3) | MM | Skeletal muscle | Muscular dystrophy, myositis |
Key rule: CK-MB > 5% of total CK activity = specific for myocardial damage
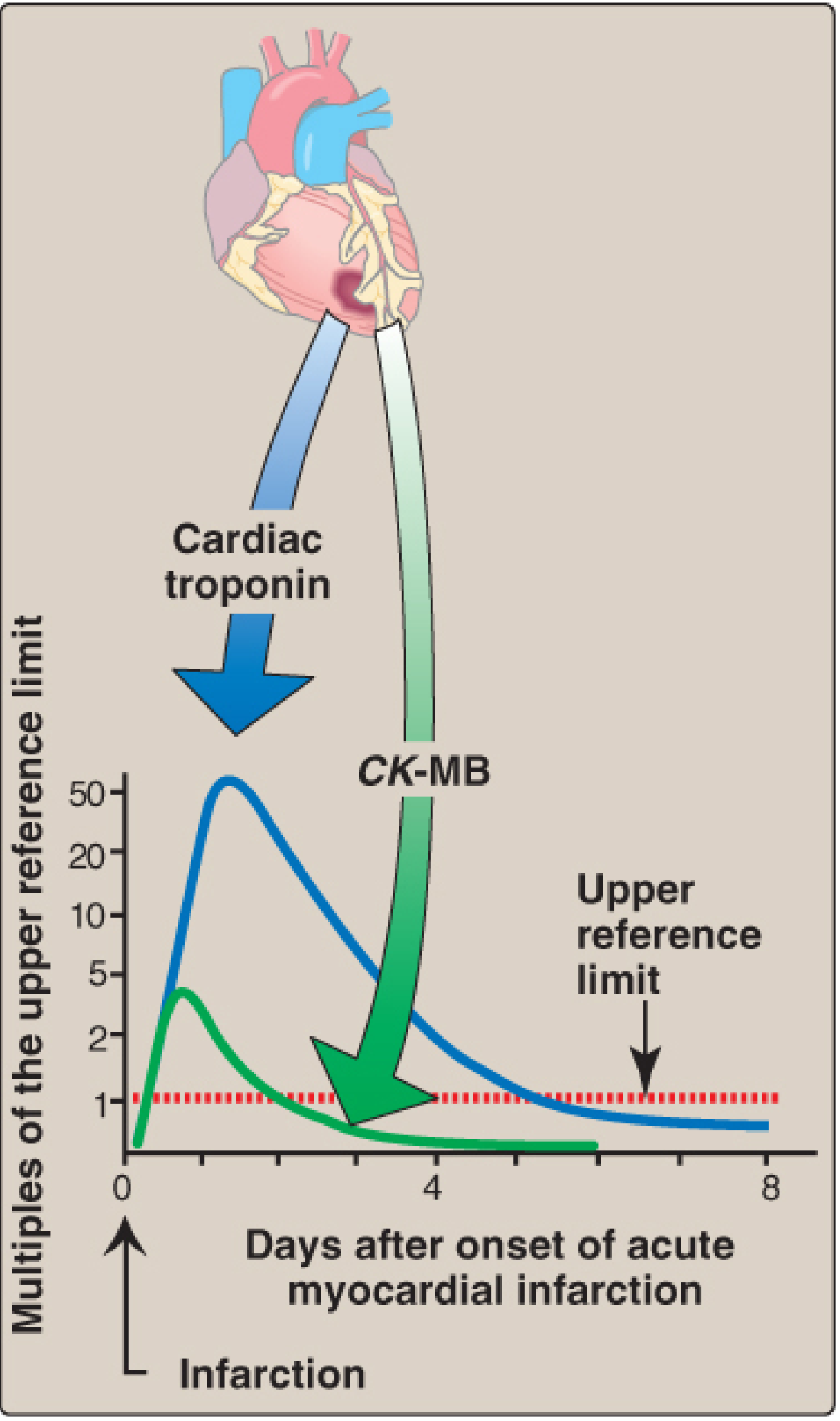
4. Cardiac Markers - Temporal Profile After MI
This is a high-yield Satyanarayana topic:
| Marker | Onset | Peak | Returns to Normal |
|---|
| CK-MB | 4-8 hours | ~24 hours | 48-72 hours |
| Cardiac Troponin (cTnI/cTnT) | 4-6 hours | 24-36 hours | 3-10 days |
| LDH (LD1 flipped pattern) | 24-48 hours | 3-6 days | 8-14 days |
Cardiac Troponins (cTnI and cTnT):
- Cardiac-specific regulatory proteins of the troponin complex
- Released into plasma after MI; peak change from baseline is far greater than CK-MB
- Cardiac troponin elevation + clinical symptoms + ECG changes = gold standard for MI diagnosis
- Because the elevation persists for 3-10 days, troponins are also useful for late diagnosis
5. Enzymes as Analytical Tools (Reagent Enzymes)
Enzymes are used as highly specific analytical reagents in the clinical laboratory to measure metabolite concentrations. The enzymatic method exploits the fact that the reaction rate is proportional to substrate concentration.
| Enzyme Used | Substrate Measured | Clinical Use |
|---|
| Glucose oxidase | Blood glucose | Diagnosis/monitoring of diabetes mellitus |
| Urease | Blood urea nitrogen (BUN) | Renal function test |
| Cholesterol oxidase | Serum cholesterol | Cardiovascular risk assessment |
| Creatinine amidohydrolase | Serum creatinine | Renal function |
| Uricase | Serum uric acid | Gout |
6. Enzyme-Linked Immunosorbent Assay (ELISA)
ELISA harnesses the amplifying power of enzymes to detect antigens or antibodies. A reporter enzyme (alkaline phosphatase or horseradish peroxidase) is conjugated to an antibody. When the antibody-enzyme conjugate binds the target antigen, addition of substrate produces a colored/fluorescent product proportional to antigen quantity.
Applications:
- HIV antibody detection
- HBsAg (Hepatitis B surface antigen)
- Troponin I and T quantitation
- TSH, LH, FSH, hCG (hormone assays)
- Drug levels, tumor markers (AFP, CEA, PSA)
- Detection of bacterial/viral pathogens
7. Molecular Diagnostic Applications
A. Restriction Fragment Length Polymorphism (RFLP)
- Uses restriction endonucleases that cleave dsDNA at specific 4-6 base-pair sequences
- Mutations that create or destroy restriction sites produce DNA fragments of different sizes
- Used for: Prenatal diagnosis of sickle cell disease, β-thalassemia, phenylketonuria (PKU), Huntington disease, forensic DNA fingerprinting
B. Polymerase Chain Reaction (PCR)
- Uses thermostable DNA polymerase (Taq polymerase) to amplify minute quantities of target DNA exponentially
- Far more sensitive than RFLP; has largely replaced it
- Diagnostic applications:
- Detection of HIV, Mycobacterium tuberculosis, Neisseria meningitidis, SARS-CoV-2
- Identification of oncogene mutations
- Carrier detection and prenatal testing for genetic disorders
- Forensic identification
B. THERAPEUTIC IMPORTANCE OF ENZYMES
1. Enzyme Replacement Therapy (ERT)
In lysosomal storage diseases, genetic deficiency of a specific lysosomal hydrolase leads to accumulation of its substrate, causing progressive organ damage. Intravenous infusion of recombinant enzyme directly replaces the missing protein:
| Disease | Deficient Enzyme | Substrate Accumulated | Drug Used |
|---|
| Gaucher disease | Glucocerebrosidase (β-glucosidase) | Glucocerebroside | Imiglucerase, Velaglucerase alfa |
| Pompe disease | Acid α-glucosidase | Glycogen | Alglucosidase alfa |
| Fabry disease | α-Galactosidase A | Globotriaosylceramide | Agalsidase alfa/beta |
| Hurler syndrome (MPS I) | α-L-Iduronidase | Heparan/dermatan sulfate | Laronidase |
| Hunter syndrome (MPS II) | Iduronate-2-sulfatase | Heparan/dermatan sulfate | Idursulfase |
| Maroteaux-Lamy syndrome (MPS VI) | Arylsulfatase B | Dermatan sulfate | Galsulfase |
| Sly disease (MPS VII) | β-Glucuronidase | Multiple GAGs | Vestronidase alfa |
2. Thrombolytic Therapy (Fibrinolytic Enzymes)
These enzymes dissolve fibrin clots in acute MI, ischemic stroke, and pulmonary embolism:
| Agent | Nature | Mechanism | Use |
|---|
| tPA (tissue plasminogen activator, alteplase) | Recombinant serine protease | Converts plasminogen → plasmin → dissolves fibrin | Acute MI, ischemic stroke (within 4.5 hrs), PE |
| Streptokinase | Bacterial enzyme (Streptococcus) | Forms streptokinase-plasminogen complex → activates plasminogen | Acute MI |
| Urokinase | Endogenous serine protease | Directly activates plasminogen | DVT, PE, catheter occlusion |
| Tenecteplase, Reteplase | Recombinant tPA variants | Modified tPA with longer half-life | Acute MI (single IV bolus) |
3. Enzyme Inhibitors as Drugs
Many important drugs act by selectively inhibiting an enzyme that is overactive or involved in disease:
| Drug | Enzyme Inhibited | Disease |
|---|
| ACE inhibitors (enalapril, lisinopril) | Angiotensin-converting enzyme | Hypertension, heart failure |
| Statins (atorvastatin, rosuvastatin) | HMG-CoA reductase | Hypercholesterolemia |
| Allopurinol | Xanthine oxidase | Gout (reduces uric acid synthesis) |
| Methotrexate | Dihydrofolate reductase (DHFR) | Cancer, rheumatoid arthritis |
| Aspirin | Cyclooxygenase (COX-1/2) | Anti-platelet, anti-inflammatory |
| Protease inhibitors (ritonavir) | HIV protease | HIV/AIDS |
| Oseltamivir (Tamiflu) | Neuraminidase | Influenza |
| Neostigmine | Acetylcholinesterase | Myasthenia gravis |
| Etoposide | Topoisomerase II | Cancer |
4. Digestive Enzyme Therapy
| Enzyme Preparation | Enzymes Contained | Use |
|---|
| Pancreatin / Pancrelipase | Lipase, protease, amylase | Exocrine pancreatic insufficiency (chronic pancreatitis, cystic fibrosis, post-Whipple's surgery) |
| Dornase alfa (DNase I) | Recombinant human DNase | Cystic fibrosis (cleaves extracellular DNA in mucus, reducing viscosity and improving lung function) |
5. Anticancer Enzymes
- L-Asparaginase: Catalyzes hydrolysis of serum asparagine → aspartate + NH₃. Cancer cells (especially in ALL - acute lymphoblastic leukemia) cannot synthesize asparagine and depend on serum supply. L-asparaginase depletes serum asparagine, selectively starving tumor cells. Used as a key drug in ALL treatment protocols.
6. Other Therapeutic Uses
| Enzyme | Use |
|---|
| Hyaluronidase | "Spreading factor" - breaks down hyaluronic acid in connective tissue, facilitating subcutaneous drug absorption and dispersal of injected fluids |
| Collagenase | Wound debridement (necrotic tissue); treatment of Dupuytren's contracture (Clostridial collagenase) |
| Trypsin | Mucolytic in wound healing; previously used in cystic fibrosis |
| Chymotrypsin | Anti-inflammatory in soft tissue injuries; used ophthalmically for cataract surgery (zonulolysis) |
| Streptokinase + Streptodornase | Wound debridement in surgical infections |
| Urokinase | Clearing thrombosed catheters/AV shunts |
Summary - Key Points for Examination
- Diagnostic principle: Cell injury → membrane disruption → intracellular enzymes leak into blood → elevated serum enzyme levels
- Organ-specific enzymes: ALT (liver), CK-MB (myocardium), PSA (prostate), amylase/lipase (pancreas)
- Isoenzymes improve specificity: LDH1>LDH2 = MI (flipped pattern); CK-MB >5% = MI
- MI cardiac markers (in order of rise): CK-MB (4-8 hrs) → Troponin (4-6 hrs, persists 3-10 days) - Troponin is gold standard
- Reagent enzymes measure metabolites (glucose oxidase, urease, cholesterol oxidase)
- ELISA uses reporter enzymes (HRP/ALP) to detect antigens/antibodies
- ERT replaces deficient lysosomal enzymes in storage disorders (Gaucher, Pompe, Fabry)
- Thrombolytics (tPA, streptokinase) = plasminogen activators for clot dissolution
- Enzyme inhibitor drugs = major pharmacological strategy (statins, ACE inhibitors, allopurinol)
- L-asparaginase = treats ALL by depleting serum asparagine
Sources: Lippincott's Illustrated Reviews: Biochemistry, 8th Ed. (Chapter 5); Harper's Illustrated Biochemistry, 32nd Ed. (Chapter 7). Content maps directly to Satyanarayana's Biochemistry, Chapter on Enzymes - Clinical/Diagnostic/Therapeutic Applications.