Help me build concepts of corticospinal tract
Reading File
Finding Sources
Finding Sources
Searching Images
corticospinal tract anatomy diagram
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive, well-sourced material. Let me compile the full conceptual breakdown of the corticospinal tract.
Corticospinal Tract — Complete Conceptual Guide
1. Overview & Clinical Significance
The corticospinal tract (CST) — also called the pyramidal tract — is the most clinically important descending motor pathway in the human nervous system. It controls voluntary movement of the extremities and face, and lesions along its course produce characteristic, localizable deficits.
"The corticospinal tract is the most clinically important descending motor pathway in the nervous system. This pathway controls movement of the extremities, and lesions along its course produce characteristic deficits that often enable precise clinical localization." — Neuroanatomy through Clinical Cases, 3e
2. Cortical Origin
The CST is a two-neuron pathway: Upper Motor Neuron (UMN) → Lower Motor Neuron (LMN).
Cortical areas contributing to the CST:
| Brodmann Area | Region | % Contribution |
|---|---|---|
| Area 4 | Primary motor cortex (precentral gyrus) | ~31% |
| Area 6 | Premotor + Supplementary Motor Area | ~29% |
| Areas 3, 1, 2, 5, 7 | Somatosensory + parietal cortex | ~40% |
- Neurons are pyramidal-shaped, located in cortical layer V
- ~3% are giant Betz cells (~60 µm diameter; only in M1) — the largest neurons in the human nervous system, conducting at ~70 m/s
- The remaining 97% are small (<4 µm) fibers carrying tonic background signals
- Total fibers per tract: >1 million
Somatotopic organization (Homunculus):
- Face/mouth → lateral (near Sylvian fissure)
- Arm/hand → midportion (disproportionately large representation)
- Trunk → near apex
- Leg/foot → medial surface (dips into longitudinal fissure)
More than half the primary motor cortex is dedicated to hands and speech muscles. — Guyton & Hall Medical Physiology
3. Course of the Tract — Segment by Segment
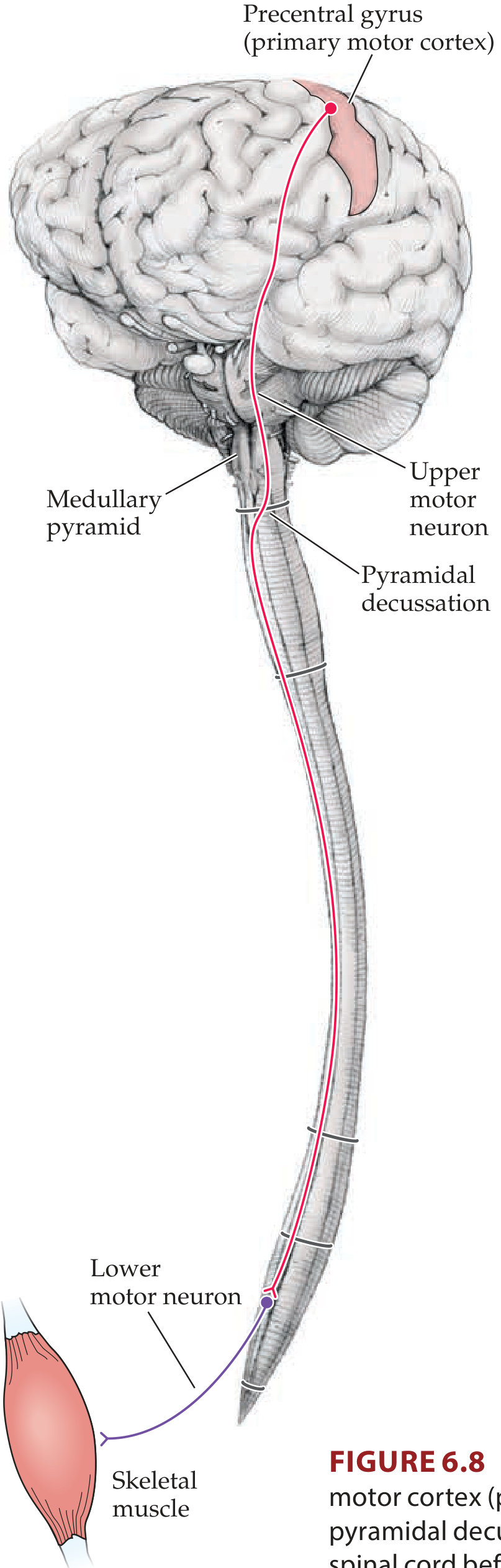
Step 1 — Corona Radiata
Axons from cortex enter the corona radiata (upper cerebral white matter), converging downward in a fan-like arrangement toward the internal capsule.
Step 2 — Internal Capsule
- CST passes through the posterior limb of the internal capsule (between caudate nucleus and putamen)
- Corticobulbar fibers pass through the genu
- Somatotopy is maintained: face anteriorly, leg posteriorly within the posterior limb
Step 3 — Cerebral Peduncle (Midbrain)
- Fibers traverse the basis pedunculi (anterior 3/5 of the cerebral peduncle)
- Corticospinal fibers occupy the middle portion; corticobulbar fibers are medial to them
Step 4 — Basilar Pons
- Fibers are broken into bundles by transverse pontine fibers and pontine nuclei
Step 5 — Medullary Pyramids
- Fibers re-aggregate to form the prominent pyramids on the ventral medulla
- At the caudal medulla: Pyramidal (Motor) Decussation
Step 6 — Decussation & Spinal Cord Tracts
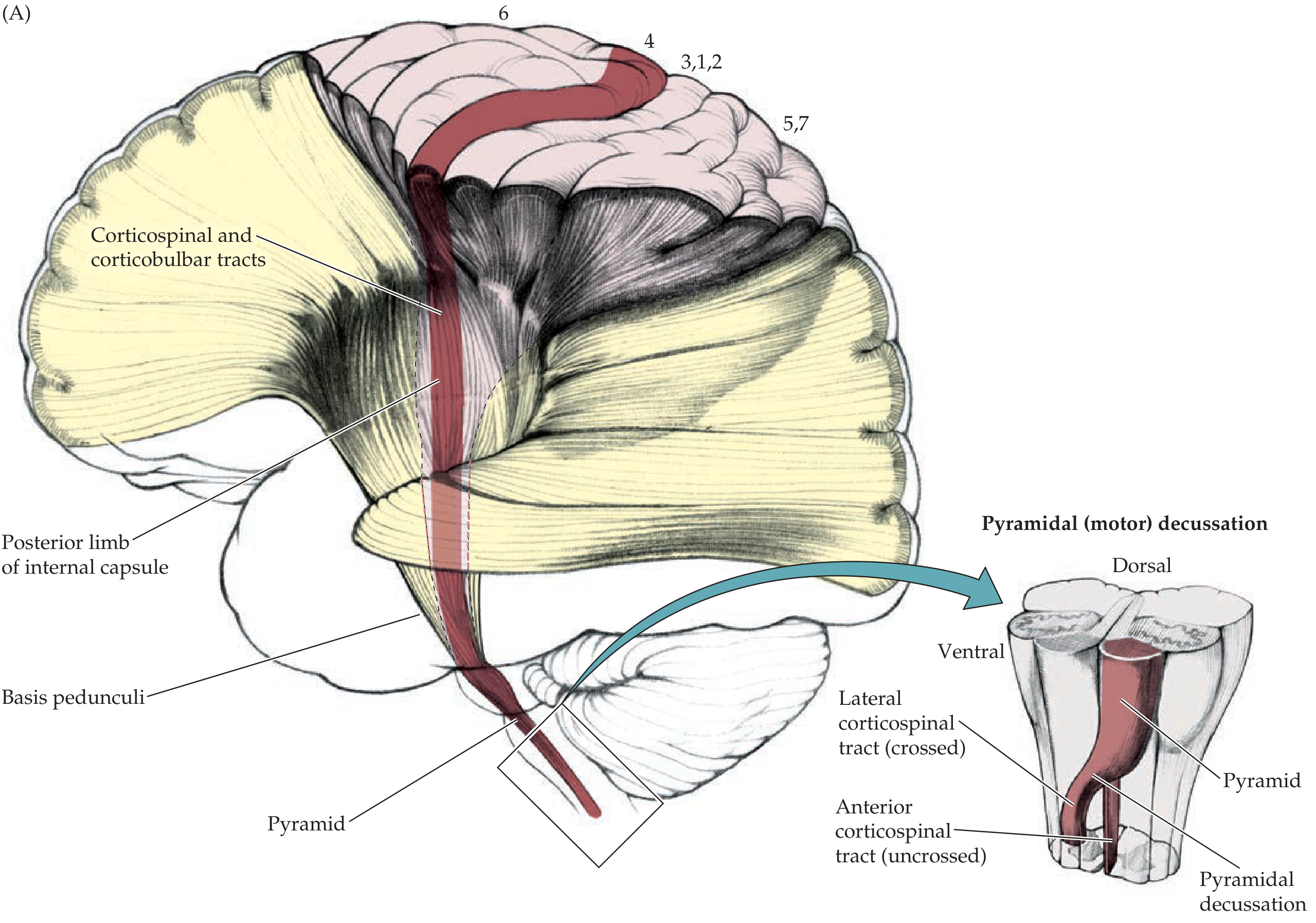
| Tract | % of Fibers | Side | Spinal Location | Function |
|---|---|---|---|---|
| Lateral corticospinal tract | ~85–90% | Crossed (contralateral) | Lateral funiculus | Controls distal limb muscles; fine voluntary movement |
| Anterior (ventral) corticospinal tract | ~10–15% | Uncrossed (ipsilateral) | Anterior funiculus | Eventually crosses via ventral white commissure at cervical/upper thoracic levels; controls bilateral axial/postural muscles |
Step 7 — Spinal Cord Termination
- Lateral CST terminates in spinal laminae IV–VII and IX (via interneurons + direct monosynaptic connections to alpha motor neurons)
- Direct monosynaptic connections are especially prominent for fine distal movements (e.g., individual finger control)
- Somatotopic arrangement within lateral CST: Cervical fibers most medial; lumbosacral fibers most lateral
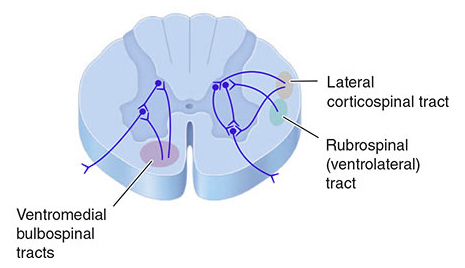
4. Spinal Cord Position of Descending Motor Tracts
5. UMN vs. LMN — The Crucial Clinical Distinction
| Feature | UMN Lesion (above anterior horn) | LMN Lesion (anterior horn / nerve) |
|---|---|---|
| Tone | Spasticity (increased) | Flaccidity (decreased) |
| Weakness | Yes | Yes |
| Reflexes | Hyperreflexia | Hyporeflexia / areflexia |
| Babinski sign | Present (extensor plantar) | Absent |
| Atrophy | Mild (disuse) | Severe (denervation) |
| Fasciculations | Absent | Present |
| Clonus | May be present | Absent |
"Damage to upper motor neurons is associated with spastic paralysis, hyperreflexia, and a positive Babinski sign. Damage to lower motor neurons is associated with flaccid paralysis, muscular atrophy, fasciculations, hypotonia, and hyporeflexia." — Ganong's Review of Medical Physiology, 26e
6. Clinically Important Lesion Levels
Understanding where the CST crosses is key to localization:
| Lesion Site | Deficit |
|---|---|
| Motor cortex (M1) | Contralateral monoparesis (arm > leg if lateral, leg > arm if medial) |
| Internal capsule | Contralateral hemiplegia (face + arm + leg, all equal — fibers are packed tightly) |
| Midbrain/cerebral peduncle | Contralateral hemiplegia + ipsilateral CN III palsy (Weber's syndrome) |
| Pons | Contralateral hemiplegia + ipsilateral CN VI/VII palsy (Millard-Gubler) |
| Medulla (above decussation) | Contralateral hemiplegia |
| Spinal cord (below decussation) | Ipsilateral weakness (same side as lesion) |
| Hemisection of cord (Brown-Séquard) | Ipsilateral UMN weakness + dorsal column loss; contralateral pain/temperature loss |
Clinical pearl: Lesions above the decussation → contralateral deficit; lesions below → ipsilateral deficit.
7. Somatotopy Within the Internal Capsule
The posterior limb of the internal capsule carries fibers in a precise order (anterior → posterior):
- Face
- Upper limb
- Trunk
- Lower limb (most posterior)
This explains why a small lacunar infarct in the posterior limb can cause pure motor hemiplegia affecting face + arm + leg proportionally.
8. The "Pyramidal Tract" Terminology
The term pyramidal tract is used (and often misused) to refer to the CST because the fibers form the pyramids on the ventral medulla. However, this is technically imprecise:
- The pyramids contain both CST fibers and some reticulospinal fibers
- "Pyramidal signs" (hyperreflexia, Babinski) are really UMN signs, not strictly pyramid lesion signs
9. Other Descending Motor Tracts (Context)
The CST works alongside extrapyramidal pathways:
| Tract | Origin | Function |
|---|---|---|
| Rubrospinal | Red nucleus (midbrain) | Fine limb movements (minor in humans; largely subsumed by CST) |
| Reticulospinal | Reticular formation (pons + medulla) | Posture, tone, autonomic control |
| Vestibulospinal | Lateral vestibular nucleus | Balance, postural reflexes |
| Tectospinal | Superior colliculus | Head/neck turning toward visual stimuli |
10. Summary Pathway (Memory Aid)
Motor Cortex (Layer V pyramidal cells, areas 4, 6, 3,1,2)
↓ Corona Radiata
↓ Posterior Limb of Internal Capsule
↓ Basis Pedunculi (midbrain)
↓ Basilar Pons (dispersed)
↓ Medullary Pyramids
↓ PYRAMIDAL DECUSSATION (caudal medulla)
↙ 85-90% ↘ 10-15%
Lateral CST Anterior CST
(crossed, lateral funiculus) (uncrossed → crosses later)
↓ ↓
Alpha motor neurons (LMN) Axial/postural motor neurons
Laminae IV–VII, IX
↓
Skeletal Muscle
Sources:
- Neuroanatomy through Clinical Cases, 3e — Chapters 6 & detailed tract anatomy
- Guyton and Hall Textbook of Medical Physiology — Ch. 56
- Ganong's Review of Medical Physiology, 26e — Ch. 12
- Localization in Clinical Neurology, 8e — Corticospinal Tract section
- Harrison's Principles of Internal Medicine, 21e — Motor tract diagrams
This is a shared conversation. Sign in to Orris to start your own chat.