A long answer on evaluation of patients with CVS disease for anasesthesia mentioning MACE, NICE guidelines, AHA guidelines, RCRI, CHADVsC score, and JNC guidelines for HTN .And any other relevant guidelines
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
preoperative cardiovascular evaluation anaesthesia MACE RCRI AHA NICE guidelines 2024
Reading File
Reading File
Finding Sources
Finding Sources
Reading Web Page
https://www.ccjm.org/content/92/4/213
Finding Sources
Finding Sources
Finding Sources
Searching the Web
NICE guideline NG45 preoperative tests routine 2016 updated cardiovascular risk assessment
Reading File
Reading File
Loading Image
Searching the Web
JNC 8 hypertension guidelines perioperative management blood pressure threshold anaesthesia 2024
I now have comprehensive data from textbooks, the 2024 ACC/AHA guidelines, NICE NG45, JNC 8, and the ESC 2022 guidelines. Let me now compose the full detailed answer.
Preoperative Cardiovascular Evaluation for Anaesthesia: A Comprehensive Review
1. Principles and Goals
The concept of "cardiac clearance" is a misnomer and should be abandoned. The real goal of preoperative cardiovascular evaluation is cardiac risk stratification - identifying risks, optimising the patient medically, selecting appropriate monitoring strategies, and in rare cases, deferring surgery for revascularisation. Prophylactic revascularisation to reduce perioperative risk is only indicated where it would be warranted anyway in the non-surgical setting (i.e., acute coronary syndrome or >50% left main coronary stenosis).
A multidisciplinary team approach - involving the surgeon, anaesthesiologist, cardiologist, and the patient - is central to all major guidelines.
2. Defining MACE
Major Adverse Cardiac Events (MACE) refers to a composite endpoint of perioperative cardiac death, non-fatal myocardial infarction, and non-fatal cardiac arrest. The 2024 AHA/ACC guidelines frame the entire preoperative evaluation around estimating the risk of MACE. A risk of <1% is considered low risk and generally permits proceeding directly to surgery, whereas ≥1% is elevated risk and triggers further assessment.
The spectrum of myocardial damage in the perioperative period ranges from subclinical troponin elevation (myocardial injury after noncardiac surgery - MINS) through to overt MI and sudden cardiac death. Patients with a history of cardiovascular disease or known cardiac risk factors undergoing major surgery are specifically at risk of MACE. The highest risk of a further event is within the first month post-surgery.
3. The ACC/AHA Stepwise Algorithm (2024 Guidelines)
The 2024 AHA/ACC/ACS/ASNC/HRS/SCA/SCCT/SCMR/SVM Guideline for Perioperative Cardiovascular Management for Noncardiac Surgery (published September 2024, superseding the 2014 guidelines) provides a revised stepwise algorithm. The 2014 framework has been updated with new evidence, new timing definitions, and an expanded set of risk modifiers.
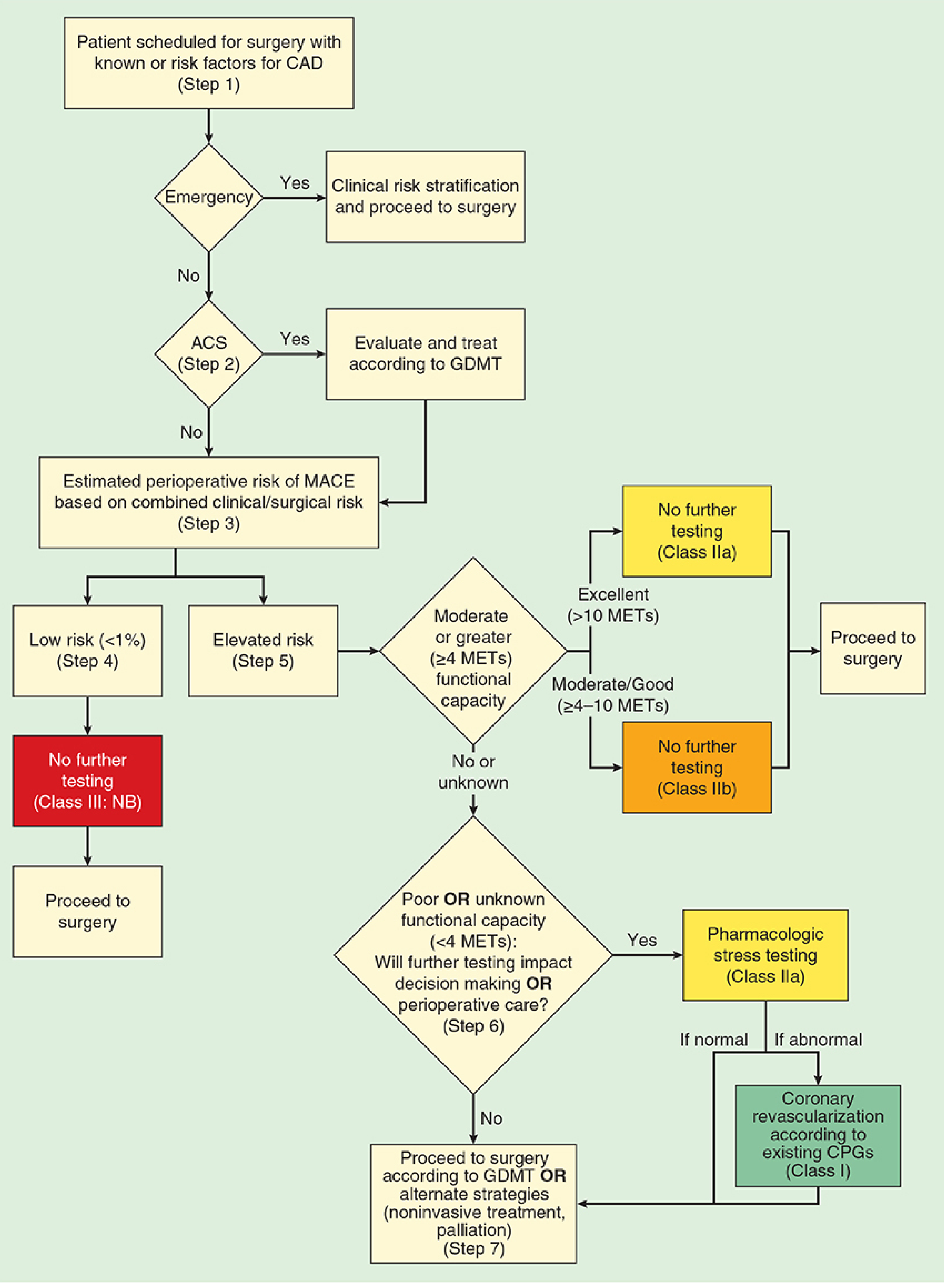
Step 1: Determine Urgency of Surgery
Revised 2024 Definitions:
| Category | Timeframe |
|---|---|
| Emergency | < 2 hours (previously < 6 hours) |
| Urgent | 2-24 hours (previously 6-24 hours) |
| Time-sensitive | Up to 3 months (previously 1-6 weeks) |
| Elective | Deferrable beyond 3 months |
For emergency surgery: proceed immediately. Identify clinical risk factors that influence perioperative management and use them to guide monitoring and treatment intraoperatively.
Step 2: Screen for Acute Coronary Syndrome (ACS)
If the patient has active cardiac conditions, elective surgery must be postponed:
- Acute coronary syndrome (STEMI, NSTEMI, unstable angina)
- Decompensated heart failure
- Significant arrhythmias (high-degree AV block, symptomatic ventricular arrhythmias, SVT with uncontrolled rate)
- Severe valvular heart disease (new category in 2024)
These patients must be referred for cardiology evaluation and treated according to guideline-directed medical therapy (GDMT).
Timing after PCI/revascularisation (2024 recommendations):
- ACS/MI within 60 days: delay surgery
- Bare-metal stent (BMS): delay at least 30 days
- Drug-eluting stent (DES): optimally delay 6 months; minimum 3 months if time-sensitive; avoid within 1 month
- High-risk PCI features: consider delay up to 12 months
Step 3: Estimate Perioperative Risk of MACE
Using the combined clinical/surgical risk, estimate MACE probability using validated tools (see Section 4 on RCRI and MICA). The 2024 guidelines give a Class IIa recommendation to use a validated risk prediction tool.
- Low risk (<1% MACE): Proceed to surgery - no further testing needed (Class III: No Benefit)
- Elevated risk (≥1% MACE): Assess functional capacity
Step 4: Assess Functional Capacity
Metabolic Equivalents (METs) are the standard measure:
| METs | Capacity |
|---|---|
| > 10 | Excellent |
| 7-10 | Good |
| 4-6 | Moderate |
| < 4 | Poor |
1 MET = resting/basal O₂ consumption of a 70-kg, 40-year-old man (~3.5 mL/kg/min)
Representative activities:
- 1 MET: Self-care, eating, dressing
- 4 METs: Walking on level ground at 4 mph, climbing one flight of stairs
- 7 METs: Playing doubles tennis
-
10 METs: Strenuous sports (swimming, singles tennis)
The 2024 guidelines add a Class IIa recommendation to use the Duke Activity Status Index (DASI) as a structured tool for functional capacity assessment - a DASI score ≤34 is associated with increased odds of 30-day death or myocardial ischaemia.
- METs ≥4: Proceed to surgery without further testing (Class IIa for excellent; Class IIb for moderate-good)
- METs <4 or unknown: Ask: "Will further testing change management or perioperative care?"
Step 5: Further Testing (for Poor/Unknown Functional Capacity)
If further testing will change management:
- Pharmacologic stress testing (Class IIa) - preferred when patient cannot exercise adequately
- If normal: Proceed to surgery with GDMT
- If abnormal: Coronary revascularisation according to existing guidelines (Class I)
If further testing will NOT change management - proceed to surgery with GDMT or consider alternative strategies (noninvasive treatment, palliation).
4. Risk Stratification Scores
4.1 Revised Cardiac Risk Index (RCRI)
The RCRI, developed by Lee et al. (1999) and validated in multiple large studies, is the most widely used and guideline-endorsed preoperative cardiac risk tool. It is endorsed by the ACC/AHA, ESC, ESA, and AHA guidelines.
| Variable | Points |
|---|---|
| High-risk surgery (intraperitoneal, intrathoracic, or suprainguinal vascular) | 1 |
| History of ischaemic heart disease | 1 |
| History of congestive heart failure | 1 |
| History of cerebrovascular disease (stroke or TIA) | 1 |
| Insulin therapy for diabetes mellitus | 1 |
| Preoperative serum creatinine >2.0 mg/dL (>177 µmol/L) | 1 |
Risk Classification:
| RCRI Score | Risk Class | Estimated Complication Risk |
|---|---|---|
| 0 | I (Very Low) | 0.4% |
| 1 | II (Low) | 0.9% |
| 2 | III (Moderate) | 7.0% |
| ≥3 | IV (High) | 11.0% |
The RCRI's main advantages are its ease of use and objective criteria. Its limitations include moderate discriminatory power between low and high risk and the fact that it was not designed for specific high-risk populations.
4.2 Gupta MICA Calculator (ACS NSQIP)
The Myocardial Infarction or Cardiac Arrest (MICA) calculator is derived from the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) dataset. It is endorsed as an alternative/supplement to RCRI by the ACC/AHA.
Variables included: Type of surgery, functional status, serum creatinine, ASA physical status class, and age.
The 2024 ACC/AHA guidelines recommend using RCRI, MICA, or the ACS Surgical Risk Calculator (ACS-SRC) for MACE estimation.
4.3 AUB-HAS2 Cardiovascular Risk Index
A newer score from the American University of Beirut, validated using ACS NSQIP data. Predictors include:
- History of heart disease
- Symptoms of heart disease (angina or dyspnoea)
- Age ≥75 years
- Anaemia (Hb <12 g/dL)
- Vascular or emergency surgery
4.4 CHA₂DS₂-VASc Score
Although primarily used to estimate thromboembolic risk in atrial fibrillation (AF) to guide anticoagulation therapy, the CHA₂DS₂-VASc score is relevant to perioperative cardiovascular evaluation because:
- AF management perioperatively - patients with AF scheduled for surgery require risk-stratified decisions about bridging anticoagulation and rate/rhythm control. A higher CHA₂DS₂-VASc score indicates greater stroke risk during the perioperative anticoagulation interruption window.
- Risk modifier - AF itself is a marker of underlying structural heart disease and increases operative risk.
- Postoperative AF (POAF) - the 2024 ACC/AHA guidelines explicitly address POAF management; the CHA₂DS₂-VASc is used to guide anticoagulation decisions post-POAF.
| Variable | Points |
|---|---|
| Congestive heart failure | 1 |
| Hypertension | 1 |
| Age ≥75 years | 2 |
| Diabetes mellitus | 1 |
| Stroke/TIA/thromboembolism history | 2 |
| Vascular disease (prior MI, PAD, aortic plaque) | 1 |
| Age 65-74 years | 1 |
| Sex category (female) | 1 |
Score interpretation: Score ≥2 (males) or ≥3 (females) - anticoagulation recommended. In the perioperative setting, if anticoagulation must be withheld, bridging therapy decisions hinge on this score.
5. Surgical Risk Classification
Surgery itself contributes to perioperative cardiac risk independently of patient factors. The ESC 2022 and ACC/AHA guidelines stratify surgical risk as:
| Risk Level | 30-Day MACE | Examples |
|---|---|---|
| Low | <1% | Endoscopic, superficial, breast, cataract, minor orthopaedic, ambulatory |
| Intermediate | 1-5% | Intraperitoneal, intrathoracic, orthopaedic spine, prostate |
| High | >5% | Aortic/major vascular, peripheral vascular |
6. Preoperative Diagnostic Testing
The decision to order tests must be guided by whether the result will change management - not obtained routinely.
ECG
- Indicated for patients with known CAD, arrhythmia, peripheral artery disease, or cerebrovascular disease
- May be considered in asymptomatic patients before intermediate- or high-risk procedures
- Not required before low-risk procedures
Echocardiography
- Reasonable for dyspnoea of unknown origin or progressive heart failure
- Should be considered for known LV dysfunction if no assessment within 1 year or if functional status has declined
- 2024 NICE NG45 added resting echocardiography to the guideline framework
Stress Testing (Exercise/Pharmacologic)
- Reserved for elevated-risk patients with poor/unknown functional capacity where results will change management
- Dobutamine stress echocardiography or myocardial perfusion imaging are the preferred modalities when the patient cannot exercise
- Exercise ECG is less sensitive for detecting ischaemia in multivessel disease
Biomarkers
- BNP/NT-proBNP: The 2024 guidelines include preoperative natriuretic peptides as a Class IIa recommendation for risk stratification in elevated-risk patients
- High-sensitivity troponin: Useful for postoperative MINS surveillance
- NT-proBNP values above the upper limit of normal (adjusted for age) indicate higher perioperative risk
7. NICE Guidelines (NG45, 2016, updated 2024)
NICE Guideline NG45: Routine Preoperative Tests for Elective Surgery (published April 2016, last updated 2024) covers adults aged >16 years undergoing elective surgery. It does NOT cover cardiothoracic procedures, neurosurgery, or pregnant patients.
The core philosophy is reducing unnecessary testing while ensuring appropriate testing for patients with comorbidities (cardiovascular disease, renal disease, respiratory disease, diabetes, and obesity). Tests are recommended according to:
- Grade of surgery: Minor / Intermediate / Major or Complex
- Patient comorbidities: ASA grade essentially maps onto this
Key cardiovascular-relevant NICE NG45 recommendations:
| Test | When indicated (cardiovascular) |
|---|---|
| 12-lead ECG | Cardiovascular disease (all grades); consider in ASA 3+ for intermediate/major surgery |
| Resting echocardiogram | Suspected heart failure, known LV dysfunction, significant murmur before major surgery |
| Full blood count | Major surgery; cardiovascular disease with major/complex surgery |
| Renal function (U&E) | Cardiovascular disease patients; those on diuretics, ACE inhibitors, ARBs; major surgery |
| HbA1c | Diabetic patients (added to NG45 in 2016 update) |
NG45 explicitly states that routine testing without clinical indication (e.g., ECG in a healthy young person having minor surgery) should not be performed, as false positives lead to unnecessary investigations, anxiety, and delays.
8. Hypertension and Anaesthesia: JNC Guidelines
JNC 7 Classification (2003)
| Category | Systolic (mmHg) | Diastolic (mmHg) |
|---|---|---|
| Normal | <120 | <80 |
| Prehypertension | 120-139 | 80-89 |
| Stage 1 HTN | 140-159 | 90-99 |
| Stage 2 HTN | ≥160 | ≥100 |
| Hypertensive crisis | ≥180 | ≥120 |
JNC 8 (2014) - Key Changes from JNC 7
JNC 8 took a more practical, evidence-based approach focused on treatment initiation thresholds and goals rather than staging:
| Population | Treatment Threshold | BP Goal |
|---|---|---|
| Age ≥60 years | BP ≥150/90 mmHg | <150/90 mmHg |
| Age 18-59 years (no DM/CKD) | BP ≥140/90 mmHg | <140/90 mmHg |
| Diabetes mellitus (any age) | BP ≥140/90 mmHg | <140/90 mmHg |
| CKD (any age) | BP ≥140/90 mmHg | <140/90 mmHg |
Drug choices per JNC 8:
- Non-Black patients: thiazide, ACE inhibitor/ARB, or calcium channel blocker (CCB)
- Black patients: thiazide or CCB as first-line
- CKD patients: ACE inhibitor or ARB mandatory
Note: The ACC/AHA 2017 hypertension guidelines (replacing JNC 8) lowered the definition of hypertension to ≥130/80 mmHg and defined Stage 1 HTN as 130-139/80-89 and Stage 2 as ≥140/90. This is the currently operational standard in the USA, though JNC 8 threshold remains in many perioperative discussions.
Perioperative Hypertension Management
Should surgery be cancelled for hypertension?
The 2014 ACC/AHA perioperative guidelines stated that Stage 1 and Stage 2 hypertension (SBP <180 mmHg and DBP <110 mmHg) is not an independent risk factor for perioperative cardiac events. However, Stage 3 hypertension (SBP ≥180 mmHg or DBP ≥110 mmHg) is generally regarded as a threshold warranting postponement of elective surgery.
The Association of Anaesthetists (UK) guideline targets SBP <160 mmHg and DBP <100 mmHg before elective surgery, with optimisation in primary care before referral.
Clinical rationale for postponing high-stage HTN:
- Hypertensive patients show exaggerated haemodynamic lability under anaesthesia
- Abrupt disruption of high peripheral resistance by induction agents causes severe hypotension
- Risk of myocardial ischaemia, stroke, and acute kidney injury
Perioperative antihypertensive drug management:
| Drug Class | Perioperative Recommendation |
|---|---|
| Beta-blockers | Continue perioperatively (do NOT abruptly stop - rebound hypertension/tachycardia) |
| ACE inhibitors/ARBs | Continue or withhold morning dose (risk of intraoperative hypotension; surgeon/anaesthetist discretion) |
| Calcium channel blockers | Continue |
| Diuretics | Withhold morning dose (hypokalaemia, hypovolaemia risk) |
| Alpha-2 agonists (clonidine) | Continue (abrupt withdrawal causes rebound hypertension) |
| Renin inhibitors | Continue |
The 2024 ACC/AHA guidelines emphasise caution when continuing antihypertensives in patients with low/low-normal perioperative BPs, those aged ≥65 years, and patients at high risk for perioperative hypotension.
Intraoperative BP targets:
Harm from hypotension begins accruing below:
- Mean arterial pressure (MAP) <65 mmHg
- Systolic BP <90-100 mmHg
9. ESC 2022 Guidelines on Cardiovascular Assessment for Non-cardiac Surgery
The 2022 ESC Guidelines on Cardiovascular Assessment and Management of Patients Undergoing Non-Cardiac Surgery provide a European counterpart to the ACC/AHA guidelines. Key additions include:
- Specific recommendations on frailty assessment as a risk modifier
- Lee RCRI as the primary risk tool, supplemented by NSQIP calculators
- NT-proBNP/BNP integrated into the risk stratification pathway for all elevated-risk patients
- Endorsement of high-sensitivity troponin surveillance postoperatively
- Specific guidance on chronic coronary syndrome (CCS) vs. ACS distinction
- Pulmonary hypertension listed as a major cardiac risk condition
- Dedicated sections on specific diseases (HF, valvular disease, arrhythmias, cardiomyopathies, congenital heart disease)
10. Heart Failure in Preoperative Assessment
Heart failure (HF) is the strongest individual predictor of perioperative MACE among the RCRI components. Key considerations:
- Decompensated HF - absolute contraindication to elective surgery; must be optimised with diuresis, ACE inhibitor/ARB, beta-blockers, and aldosterone antagonists
- Stable, compensated HF - quantify LV function (echocardiography), optimise GDMT
- EF ≥50% (HFpEF) - often underappreciated risk; diastolic dysfunction leads to poor tolerance of fluid shifts
- EF <40% (HFrEF) - higher risk; BNP/NT-proBNP useful for baseline and risk stratification
- BNP thresholds (2024 ACC/AHA): Elevated BNP associated with significantly increased perioperative risk; NT-proBNP >300 pg/mL (age-adjusted upper limit) signals elevated risk
11. Valvular Heart Disease
| Condition | Perioperative Implications |
|---|---|
| Severe aortic stenosis (AS) | Highest risk; AVR or TAVR should be considered before elective major surgery; haemodynamic maintenance critical (sinus rhythm, preload, afterload) |
| Mitral stenosis | High risk with tachycardia (reduces diastolic filling time); rate control essential |
| Severe AR/MR | Usually tolerated better; afterload reduction helpful |
| Prosthetic valves | Anticoagulation management (bridging); endocarditis prophylaxis |
12. Coronary Artery Disease - Specific Considerations
- Stable, known CAD with coronary evaluation (stress test/catheter) in the past year and no change in symptoms - proceed to surgery
- CABG >5 years ago or prior PCI with restenosis symptoms - requires reassessment
- Perioperative beta-blocker therapy: should be continued in patients already on them; initiating new beta-blockade immediately before surgery is not recommended (increased risk of stroke and death per the POISE trial)
13. Arrhythmias
- Atrial fibrillation (AF): Most common perioperative arrhythmia. Control rate (target HR <100 bpm) before elective surgery. Anticoagulation management depends on CHA₂DS₂-VASc score and bleeding risk (HAS-BLED score).
- Ventricular arrhythmias: Sustained VT requires investigation and treatment before elective surgery
- Cardiac implantable electronic devices (CIEDs): Pacemakers and ICDs require specific perioperative management - electrosurgical interference, reprogramming, and post-procedure device interrogation
14. Frailty
The 2024 ACC/AHA guidelines newly incorporate frailty as a risk modifier. Frailty is an independent predictor of adverse perioperative outcomes beyond what is captured by traditional cardiac risk indices. Tools include:
- Clinical Frailty Scale (CFS)
- Fried Frailty Phenotype
- FRAIL questionnaire
Frail patients have higher rates of MACE, prolonged hospitalisation, and loss of independence post-surgery.
15. Summary Algorithm (Practical Approach)
Patient scheduled for non-cardiac surgery
│
▼
Emergency? ──YES──► Proceed; manage risk factors intraoperatively
│ NO
▼
Active cardiac conditions (ACS, decompensated HF,
severe arrhythmia, severe VHD)?
YES──► Postpone; treat per GDMT
│ NO
▼
Estimate MACE risk (RCRI/MICA/ACS-SRC)
+ Surgery risk category (low/intermediate/high)
│
MACE <1%──► Proceed (no further testing)
│
MACE ≥1%──► Assess functional capacity (METs/DASI)
│
METs ≥4──► Proceed to surgery
│
METs <4/unknown──► Will testing change management?
YES──► Pharmacologic stress test
NO──► Proceed with GDMT/palliation
16. Preoperative Laboratory Testing Summary
| Investigation | Indication |
|---|---|
| 12-lead ECG | Known CVD, arrhythmia, PAD, cerebrovascular disease; age >65 with major surgery |
| Echocardiogram | Dyspnoea of unknown cause; known LV dysfunction (if not assessed within 1 year); severe valvular disease |
| Stress test | Poor functional capacity (<4 METs); elevated MACE risk; result will change management |
| BNP/NT-proBNP | Elevated-risk patients; HF patients |
| FBC | Major surgery; age ≥65; anticipated significant blood loss |
| Renal function | CVD patients; diuretics/ACEi/ARB use; major surgery |
| Electrolytes | Age ≥65 with major surgery; HTN, DM, CVD on relevant medications |
| HbA1c | Diabetics undergoing vascular or orthopaedic surgery |
| Coagulation | Anticoagulant use; known coagulopathy; major haemorrhage-risk surgery |
Key Guideline References
| Guideline | Focus |
|---|---|
| 2024 AHA/ACC Perioperative Cardiovascular Management for Noncardiac Surgery | Comprehensive US guideline; stepwise algorithm; RCRI, MICA, DASI, frailty |
| 2022 ESC Guidelines on Cardiovascular Assessment for Non-Cardiac Surgery | European guideline; NT-proBNP integral; frailty; chronic vs. acute coronary states |
| NICE NG45 (2016, updated 2024) | UK: Routine preoperative tests; comorbidity-based matrix; reduces over-testing |
| JNC 8 (2014) | Hypertension management; treatment thresholds; BP goals by patient population |
| ACC/AHA 2017 HTN Guidelines | Redefined HTN ≥130/80; currently operational US standard |
| RCRI - Lee et al. (1999) | Six-factor validated cardiac risk index for noncardiac surgery |
| Association of Anaesthetists UK | BP thresholds (<160/100 mmHg) before elective surgery |
A note on currency: The 2024 ACC/AHA guideline is the most up-to-date major international perioperative cardiovascular guideline as of June 2026. It supersedes the 2014 ACC/AHA guideline and updates definitions of surgical urgency, introduces DASI and frailty assessment, reinforces a conservative approach to prophylactic revascularisation, and expands guidance on postoperative care including POAF and MINS.
This is a shared conversation. Sign in to Orris to start your own chat.