Explain me about chronic peptic ulcer
Reading File
Finding Sources
Searching PubMed
"peptic ulcer"[MeSH Terms] AND ("pathogenesis" OR "management")
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have excellent, comprehensive information from multiple authoritative textbooks. Let me compose the full answer.
Chronic Peptic Ulcer
A chronic peptic ulcer is a persistent, full-thickness mucosal defect in a region exposed to acid-pepsin secretions. Unlike acute stress ulcers (which are shallow and superficial), chronic peptic ulcers penetrate through the mucosa into the muscularis, producing a fibrous scar base - hence the word "chronic." The duodenum (first part) and gastric lesser curvature near the antrum-body junction are the two most common sites.
1. Epidemiology
- Affects more than 4 million individuals per year in the United States alone.
- Lifetime risk: ~10% in males, ~4% in females.
- Incidence of H. pylori-related ulcers is falling as infection rates decline, but NSAID-related ulcers (especially in those over 60) are rising.
- Duodenal ulcers are more common than gastric ulcers; both share largely indistinguishable symptoms.
(Robbins & Kumar Basic Pathology, p. 715; Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 717)
2. Etiology and Risk Factors
The fundamental mechanism is an imbalance between mucosal defense and acid-peptic attack. Despite its name, pepsin itself is of secondary importance - acid is the key, as ulcers do not occur in its absence and virtually all can be healed by proton pump inhibitors (PPIs).
Key Causes
| Cause | Mechanism |
|---|---|
| H. pylori infection | Physically burrows through the mucus barrier; releases urease → ammonia → liquefies barrier + stimulates HCl secretion; induces chronic antral gastritis → reduced somatostatin → increased gastrin → increased acid |
| NSAIDs / Aspirin | Inhibit COX-1 → reduced prostaglandin E2 and I2 → reduced mucus + bicarbonate secretion, reduced mucosal blood flow, impaired epithelial renewal |
| Zollinger-Ellison syndrome | Gastrinoma secretes gastrin constitutively → massive acid hypersecretion → multiple ulcers (stomach, duodenum, even jejunum) |
| Cigarette smoking | Reduces mucosal blood flow and healing; increases relapse rate |
| Corticosteroids (high-dose) | Suppress prostaglandin synthesis, impair healing |
| Alcohol | Breaks down the mucosal barrier directly |
Associated Conditions
- Alcohol-related cirrhosis
- Chronic obstructive pulmonary disease
- Chronic renal failure and hyperparathyroidism (hypercalcemia stimulates gastrin → acid)
More than 70% of PUD cases are associated with H. pylori infection. However, only 5-10% of infected individuals develop ulcers, so host factors and bacterial strain variation both matter.
(Guyton & Hall Medical Physiology, p. 825; Robbins, Cotran & Kumar, p. 717; Bailey & Love's Surgery, p. 1179)
3. Pathogenesis in Detail
Normal protection relies on:
- Mucus-bicarbonate layer secreted by surface epithelium and Brunner's glands
- Mucosal blood flow (delivering oxygen and removing acid)
- Epithelial tight junctions
- Prostaglandins (E2 and I2)
- Pancreatic bicarbonate neutralizing duodenal acid
When defenses fail:
- H. pylori in the antrum → antral gastritis → loss of somatostatin-secreting D cells → unchecked gastrin → parietal cell hyperplasia → excess HCl
- H. pylori also directly damages the duodenal mucosa and reduces bicarbonate secretion
- NSAIDs deplete prostaglandins systemically (COX-1 inhibition) even if taken parenterally or rectally
- Both H. pylori and NSAIDs act synergistically, especially with low-dose aspirin in cardiovascular patients
(Guyton & Hall, p. 825; Robbins & Kumar Basic Pathology, p. 715-716)
4. Morphology (Gross and Histological)
Gross Appearance
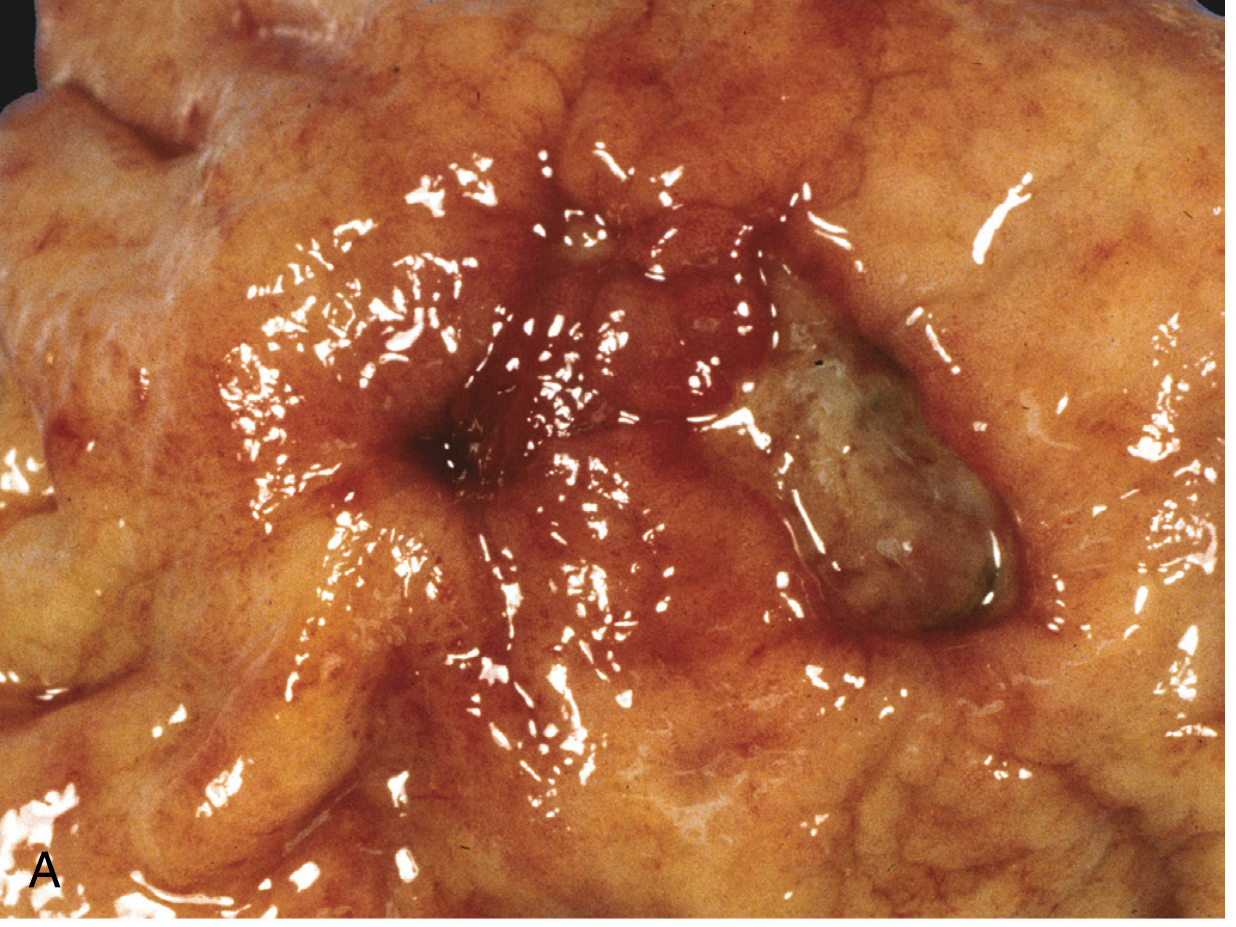
Gross specimen: a round to oval, sharply punched-out mucosal defect with a clean base - the hallmark of benign peptic ulcer (Robbins, Cotran & Kumar, Fig. 17.17A)
Key gross features:
- Solitary in >80% of patients
- Round to oval, sharply punched-out ("cookie cutter") defect
- Mucosal margin is flat or at the same level as surrounding mucosa (heaped/rolled margins suggest malignancy)
- Located most often in the proximal duodenum (within a few cm of the pyloric valve) or lesser curvature of gastric antrum/body junction
- The base is smooth and clean due to peptic digestion of exudate
Histological Appearance
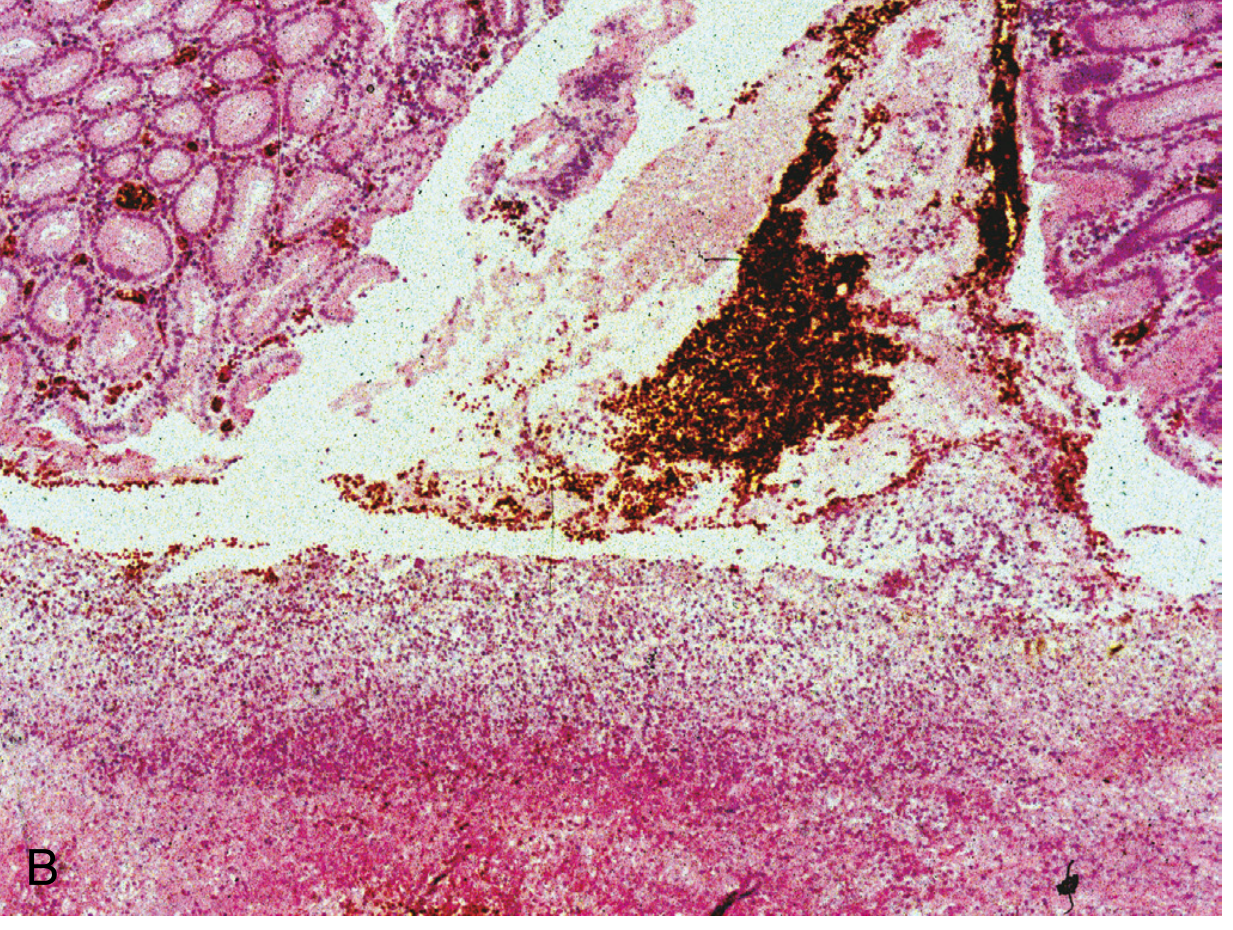
Histology (H&E): ulcer base with granulation tissue and inflammatory infiltrate (Robbins, Cotran & Kumar, Fig. 17.17B)
The histological layers (from surface to deep) in an active chronic peptic ulcer:
- Superficial fibrinoid necrosis - thin layer of fibrinoid debris
- Neutrophilic infiltrate - active inflammation
- Granulation tissue - immature vessels, neutrophils, mononuclear cells
- Fibrous/collagenous scar - the defining feature of "chronic" ulcer; extends through the full thickness of the wall
Additional features:
- Larger vessels in the scarred base are thickened and may be thrombosed - rupture of these causes life-threatening hemorrhage
- Scarring may contract the surrounding mucosa into radiating folds
- Foveolar (gastric-type) metaplasia in the duodenum is common and may be a protective adaptation
- In duodenal chronic peptic disease, the ulcer penetrates the muscular coat, leading to fibrosis and possible deformity (e.g., pyloric stenosis from scarring)
(Robbins, Cotran & Kumar, p. 717-718; Bailey & Love's, p. 1179)
5. Sites of Occurrence
| Site | Notes |
|---|---|
| First part of duodenum | Most common overall; within a few cm of pyloric valve |
| Gastric antrum/lesser curvature | Near antrum-body junction |
| Prepyloric/pyloric channel | Similar behavior to duodenal ulcer; biopsy essential to exclude malignancy |
| Stomal (marginal) | Following gastroenterostomy or Billroth II gastrectomy; on the jejunal side |
| Esophagus | From chronic GERD or ectopic gastric mucosa (inlet patch) |
| Meckel's diverticulum | Contains ectopic gastric mucosa |
6. Clinical Features
Symptoms
- Epigastric pain - gnawing or burning quality, classically 1-3 hours after meals, worse at night (11 pm - 2 am)
- Food/alkali relieves the pain (esp. duodenal ulcers)
- Periodicity - symptoms may disappear for weeks/months and recur (related to spontaneous healing and re-ulceration)
- Nausea, vomiting, bloating, belching
- Weight loss (or rarely weight gain)
- Referred pain to the back, left upper quadrant, or chest (penetrating ulcers)
- Iron deficiency anemia from chronic slow bleeding
Examination
- Epigastric tenderness on palpation
- Gastric outlet obstruction: succussion splash, visible peristalsis, distension
- Acute complications produce peritonism (perforation) or hemodynamic instability (major bleed)
(Bailey & Love's, p. 1179; Robbins, Cotran & Kumar, p. 718)
7. Complications
| Complication | Frequency | Key Points |
|---|---|---|
| Bleeding | 15-20% of patients | Most frequent complication; accounts for 25% of ulcer-related deaths; may be the first presentation; posterior duodenal ulcers erode the gastroduodenal artery |
| Perforation | Up to 5% of patients | Accounts for two-thirds of ulcer-related deaths; anterior duodenal ulcers most prone; presents with free air under the diaphragm on erect CXR |
| Gastric outlet obstruction (stenosis) | ~2% of patients | Mostly chronic ulcers; due to edema or scarring; pyloric channel ulcers most often implicated; causes incapacitating pain and intractable vomiting |
| Penetration | Less common | Ulcer penetrates adjacent organs (pancreas, liver, colon); produces referred back pain or fistula |
| Malignant transformation | Gastric only | Gastric ulcers may be malignant from the start or undergo malignant change; all gastric ulcers must be biopsied; duodenal ulcers are almost never malignant |
(Robbins, Cotran & Kumar, Table 17.4, p. 718; Bailey & Love's, p. 1179)
8. Investigations
- Upper GI endoscopy (OGD): investigation of choice; allows direct visualization + biopsy
- All gastric ulcers require multiple biopsies to exclude malignancy
- CLO (Campylobacter-like organism) test on antral biopsy for H. pylori
- Barium meal: shows ulcer crater (filling defect with radiating folds); largely replaced by endoscopy
- H. pylori testing: urea breath test, stool antigen test, serology, or histology
- Fasting serum gastrin: if Zollinger-Ellison syndrome suspected
- FBC: for iron deficiency anemia
- Erect CXR: free air under diaphragm in perforation
9. Treatment
Medical (First-Line)
1. H. pylori Eradication (Triple Therapy)
- Standard: PPI + Amoxicillin + Clarithromycin for 7-14 days
- Quadruple therapy (PPI + bismuth + metronidazole + tetracycline) for clarithromycin-resistant strains
- Successful eradication reduces recurrence to <20% (vs. ~80% without eradication)
- Confirm eradication with urea breath test (at least 4 weeks after therapy, 2 weeks off PPI)
2. Acid Suppression
- Proton pump inhibitors (PPIs): block H⁺/K⁺-ATPase; mainstay of acid suppression; render patient virtually achlorhydric
- H2-receptor antagonists (e.g., ranitidine): block histamine effect on parietal cells; reduce acid by 70-80%; now largely superseded by PPIs
- Potassium-competitive acid blockers (P-CABs) (e.g., vonoprazan): bind to the K⁺-binding region of the proton pump; faster and more consistent acid suppression
3. Remove Offending Agents
- Stop NSAIDs, COX-2 inhibitors, corticosteroids where possible
- Add PPI for patients who must continue NSAIDs
- Cessation of smoking and alcohol
Endoscopic Management (for Bleeding Ulcers)
- Injection therapy (adrenaline), thermal coagulation, hemoclips
- Rockall score used to stratify risk (see scoring table from Sleisenger & Fordtran)
Surgical Management (Now Rare Electively)
- No longer routine for uncomplicated PUD
- Reserved for emergencies: bleeding that fails endoscopy, perforation, obstruction
- Perforation: omental patch repair (Graham's patch) ± lavage; laparoscopic approach now preferred
- Gastrectomy (Billroth I or II): historical elective operations; now only for emergency or failed endoscopy
- Vagotomy (highly selective or truncal + drainage): reduces acid secretion; largely historical
(Guyton & Hall, p. 825; Bailey & Love's, p. 1179-1182; Robbins, Cotran & Kumar, p. 718)
10. Special Situations
| Situation | Notes |
|---|---|
| Zollinger-Ellison syndrome | Multiple, recurrent, refractory ulcers; high fasting gastrin; treat with long-term high-dose PPI; surgery if tumor resectable |
| NSAID users who cannot stop | Add PPI; consider switching to selective COX-2 inhibitor (though still some risk) |
| Refractory ulcer | Most common cause is persistent H. pylori; consider Zollinger-Ellison; rarely IgG4-related disease |
| Pregnancy | Avoid NSAIDs; PPI use generally considered acceptable; H. pylori eradication often deferred |
| Gastric ulcer follow-up | Mandatory endoscopic re-evaluation at 6-8 weeks to confirm healing and exclude malignancy |
Summary
Chronic peptic ulcer = a full-thickness mucosal defect (through mucosa into muscularis, with a fibrous scar base) caused by acid-peptic digestion exceeding the mucosal defenses. The two dominant causes are H. pylori infection and NSAID use. The ulcer is almost always solitary, round, with a punched-out clean base, and most commonly sited in the duodenal bulb or gastric lesser curvature. Medical management with PPI + H. pylori eradication is the cornerstone of treatment; surgery is reserved for complications.
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease | Robbins & Kumar Basic Pathology | Bailey & Love's Short Practice of Surgery, 28th ed. | Guyton & Hall Medical Physiology | Sleisenger & Fordtran's GI and Liver Disease
I need this from general medicine Davidson
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Unfortunately, Davidson's Principles and Practice of Medicine is not available in our medical textbook library. The library does not have a copy of Davidson's.
However, we do have several excellent general medicine/internal medicine textbooks that cover chronic peptic ulcer disease from a clinical medicine perspective - very similar to how Davidson's approaches it. The best equivalents available are:
| Book | Why it's similar to Davidson's |
|---|---|
| Harrison's Principles of Internal Medicine 22e (2025) | The gold-standard internal medicine reference; covers PUD with the same clinical medicine lens as Davidson's |
| Goldman-Cecil Medicine | Comprehensive internal medicine text, direct Davidson's equivalent |
| Washington Manual of Medical Therapeutics | Practical clinical management focus |
Would you like me to pull the chronic peptic ulcer content from Harrison's or Goldman-Cecil Medicine instead? Both are general/internal medicine texts that cover PUD in essentially the same clinical style as Davidson's - with epidemiology, pathophysiology, diagnosis, and management all in one place.
Pull peptic ulcer content from Harrison's Internal Medicine instead
This is a shared conversation. Sign in to Orris to start your own chat.