Types of constipation , rome 4 criteria , transit time , ibs answer in detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the material I need for a comprehensive, well-structured answer. Let me compile it.
Constipation: Types, Rome IV Criteria, Transit Time, and IBS
1. Definition of Constipation
Constipation is not a single symptom but a spectrum of complaints. The traditional medical definition has been 3 or fewer bowel movements per week (the 95th percentile lower limit in healthy adults), but patients themselves most commonly define it as:
- Straining (52%)
- Hard stools (44%)
- Inability to have a bowel movement (34%)
The Rome criteria were developed to standardize this, recognizing that stool frequency is only one of several relevant symptoms.
(Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 271)
2. Types of Constipation
Constipation is broadly divided into primary (functional) and secondary forms.
A. Secondary Constipation
Caused by identifiable extrinsic factors:
- Medications: Opioids, anticholinergics, calcium channel blockers, iron, antidepressants
- Endocrine/Metabolic: Hypothyroidism, hypercalcemia, diabetes mellitus (mean colonic transit time significantly prolonged in diabetics - 34.9 ± 29.6 hours vs. controls)
- Neurological: Parkinson's disease, multiple sclerosis, spinal cord lesions
- Structural/Mechanical: Colorectal cancer, strictures, rectocele
- Dietary/Lifestyle: Low-fiber diet, dehydration, immobility
B. Primary (Functional) Constipation - Three Subtypes
1. Slow-Transit Constipation (STC)
- Results from intrinsic dysmotility of the colon with significant impairment of propulsive colonic motor activity
- High-amplitude propagated contractions (HAPCs) are reduced in frequency and duration
- Some patients have no peristaltic movement over 24 hours; others have fewer and shorter movements than controls
- May involve only the colon or the entire GI tract
- Patients may go days to weeks without bowel movements despite using laxatives and enemas
- Pathology: Reduced numbers and abnormal morphology of interstitial cells of Cajal (ICCs), decreased substance P, increased VIP and nitric oxide in myenteric plexus; the predefecatory period (gastrocolic reflex) is blunted or absent
2. Normal-Transit Constipation (NTC)
- Stool traverses the colon at a normal rate; stool frequency may even be normal
- Patients feel constipated - report hard stools, difficult defecation, bloating, and abdominal pain relieved by defecation
- Significant overlap with IBS-C (constipation-predominant IBS)
- Psychological factors play a larger role; often associated with altered visceral sensation
3. Pelvic Floor / Outlet Obstruction / Defecatory Disorder Constipation
- Caused by failure of coordinated pelvic floor relaxation during defecation (dyssynergic defecation / anismus)
- Also includes mechanical causes: rectocele, enterocele, sigmoidocele, rectal intussusception, full-thickness rectal prolapse, solitary rectal ulcer syndrome
- These disrupt the coordinated transit of stool through the rectum
- A specific subtype - dyssynergic defecation - is defined by paradoxical contraction (or <20% relaxation) of the anal sphincter during defecation attempts
(Sabiston Textbook of Surgery, 28th ed., p. 2174; Yamada's Textbook of Gastroenterology, 7th ed.)
3. Rome IV Criteria
Rome IV Criteria for Functional Constipation
Must include 2 or more of the following (present for the last 3 months, with symptom onset at least 6 months before diagnosis):
| Criterion | Threshold |
|---|---|
| a. Straining during defecations | >25% of defecations |
| b. Lumpy or hard stools (Bristol types 1-2) | >25% of defecations |
| c. Sensation of incomplete evacuation | >25% of defecations |
| d. Sensation of anorectal obstruction/blockage | >25% of defecations |
| e. Manual maneuvers to facilitate defecation (e.g., digital evacuation, pelvic floor support) | >25% of defecations |
| f. Fewer than 3 spontaneous bowel movements per week | - |
Additional requirements:
- Loose stools are rarely present without the use of laxatives
- There are insufficient criteria for IBS (pain is not a predominant feature)
Key change in Rome IV vs. III: Rome IV raises the symptom frequency threshold from "3 days per month" to "at least 1 day per week" - increasing specificity but reducing sensitivity compared to Rome III.
(Sleisenger and Fordtran's GI & Liver Disease, p. 271; Yamada's Textbook of Gastroenterology, 7th ed., p. 730)
Rome IV Diagnostic Criteria for Dyssynergic Defecation
Patients must fulfill all three:
- Diagnostic criteria for functional chronic constipation (Rome IV)
- Dyssynergia demonstrated during repeated attempts to defecate: paradoxical increase in anal sphincter pressure (contraction) OR <20% relaxation of resting pressure, on manometry/imaging/EMG
- One or more of:
- Inability to expel an artificial stool (50 mL water-filled balloon) within 1 minute
- Prolonged colonic transit time (>5 markers retained / ≥20% retention on plain X-ray at 120 hours after ingesting one Sitzmarks capsule)
- Inability to evacuate or ≥50% retention of barium during defecography
(Yamada's Textbook of Gastroenterology, 7th ed., p. 730)
4. Colonic Transit Time
Transit time is measured to confirm and quantify constipation complaints, identify slow transit, and guide treatment. The American and European Neurogastroenterology and Motility Societies recommend three methods:
A. Radiopaque Marker Testing (Sitzmarks)
- Method: Patient ingests plastic beads/rings (24 markers); plain abdominal X-ray at 5 days (120 hours)
- Normal: >80% of markers passed (i.e., <5 markers / <20% retained) by day 5
- Slow transit: ≥5 markers retained, scattered throughout colon
- Outlet obstruction: Markers converge in sigmoid/rectum
- Normal mean colonic transit time: 30-40 hours; upper limit of normal = 72 hours
- Women often have longer maximal transit times than men (70-106 hours vs. 50 hours)
- Patient must be on high-fiber diet; must avoid laxatives/enemas before study
B. Wireless Motility Capsule (SmartPill)
- Method: Patient swallows a capsule after a standardized meal; the capsule measures temperature, pH, and pressure continuously as it travels the GI tract; data receiver worn for up to 5 days
- Gastric emptying determined by rise in pH (entry into duodenum); entry into colon marked by drop in pH
- Also measures gastric emptying time and small bowel transit time
- Normal colonic transit time: 10-59 hours
- Abnormal (delayed): >44 hours in men, >59 hours in women
- No radiation exposure
- Specificity 0.95, sensitivity 0.46 for identifying abnormal transit
C. Scintigraphy
- Uses radiolabeled isotopes to track stool movement in real time through the colon
- Allows assessment of segmental colonic transit
- Quantitative and functional but involves radiation; less widely available
(Sleisenger and Fordtran's GI & Liver Disease, pp. 283-284; Yamada's Textbook of Gastroenterology, 7th ed.)
5. IBS (Irritable Bowel Syndrome)
Rome IV Criteria for IBS
Recurrent abdominal pain, on average at least 1 day per week in the last 3 months, associated with 2 or more of the following:
- Related to defecation
- Associated with a change in frequency of stool
- Associated with a change in form (appearance) of stool
- Criteria fulfilled for the previous 3 months, with symptom onset at least 6 months before diagnosis
- Abdominal pain is mandatory - IBS should NOT be diagnosed in its absence
Key Rome IV change from Rome III: Removed "onset associated with" and replaced it with "associated with"; also changed symptom frequency from "≥3 days/month" (Rome III) to "≥1 day/week" (Rome IV), increasing specificity.
(Sleisenger and Fordtran's GI & Liver Disease, p. 2469; Yamada's Textbook of Gastroenterology, 7th ed.)
IBS Subtypes (Based on Bristol Stool Form Scale)
IBS is classified by predominant stool pattern. The 25% threshold applies:
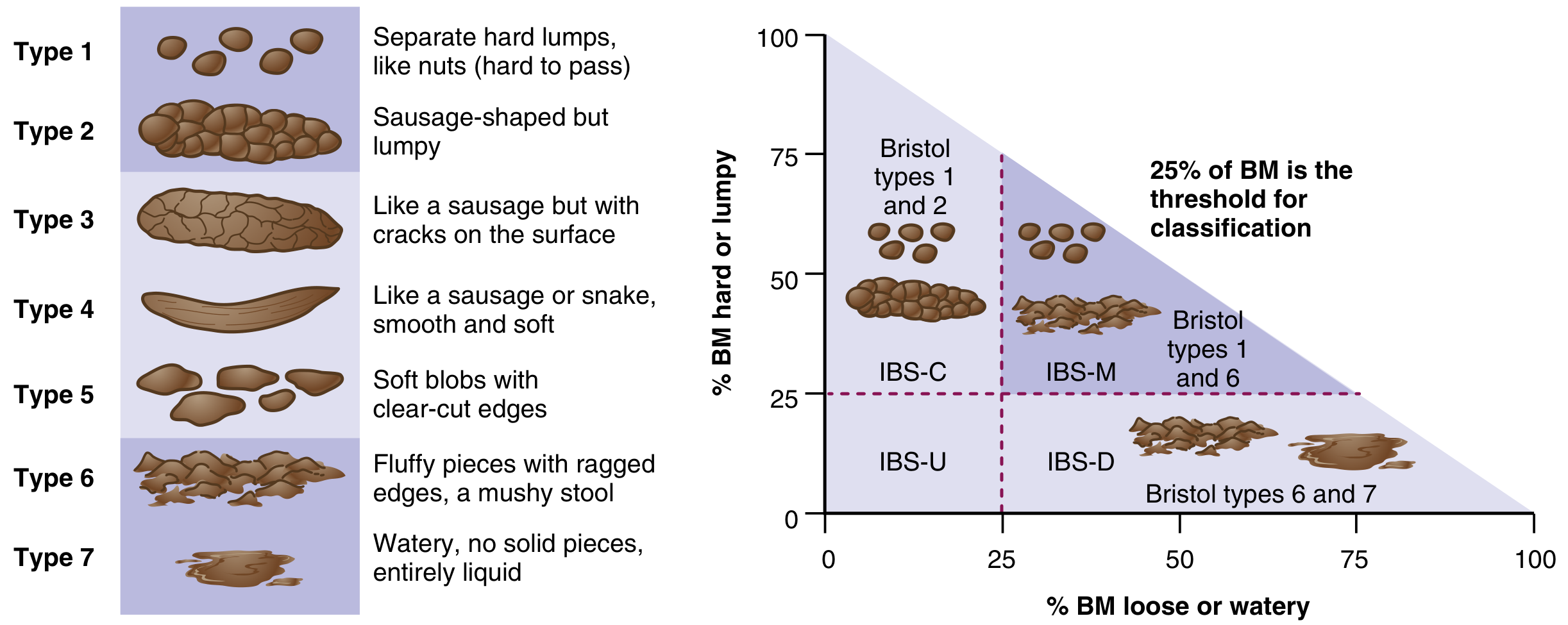
| Subtype | Definition (when not on stool-altering meds) |
|---|---|
| IBS-C (constipation-predominant) | ≥25% of BMs are Bristol types 1-2 (hard/lumpy); <25% are types 6-7 |
| IBS-D (diarrhea-predominant) | ≥25% of BMs are Bristol types 6-7 (loose/watery); <25% are types 1-2 |
| IBS-M (mixed) | ≥25% of BMs are Bristol types 1-2 AND ≥25% are types 6-7 |
| IBS-U (unsubtyped) | Insufficient abnormality of stool consistency to meet IBS-C, D, or M |
Note: Stool patterns in IBS are unstable - patients commonly shift subtypes over time.
(Adapted from Mearin F, Lacy BE, Chang L, et al. Gastroenterology 2016;150:1393-1407)
Historical Diagnostic Criteria for IBS
Manning Criteria (1978) - Positive diagnosis requires ≥3 of 6:
- Abdominal distention
- Abdominal pain eased after bowel movement
- Feeling of incomplete emptying
- Looser stools at onset of abdominal pain
- More frequent bowel movements at onset of abdominal pain
- Mucus per rectum
Kruis Criteria (1984) - Score-based; IBS excluded if any physical finding or lab abnormality:
- Patient history: abdominal pain, flatulence, irregularity, mixed diarrhea/constipation, pellet stools/mucus, symptoms >2 years
- Physician assessment: no abnormal findings, normal ESR, normal CBC, no blood in stool
(Sleisenger and Fordtran's GI & Liver Disease, p. 2469)
Pathophysiology of IBS
IBS involves a complex interaction of multiple mechanisms (biopsychosocial model):
1. Altered Motility
- IBS-D: Increased high-amplitude propagated contractions, enhanced gastrocolic reflex, rectal hypersensitivity
- IBS-C: Increased segmental (non-propulsive) contractions, decreased HAPCs, reduced rectal sensation
- Colonic and small bowel transit are delayed in IBS-C and accelerated in IBS-D
- Autonomic dysfunction: sympathetic adrenergic dysfunction in diarrhea; vagal dysfunction in constipation
2. Visceral Hypersensitivity
- Balloon distention of the rectum induces pain at lower volumes in IBS patients (up to 60% of patients)
- Serves as a potential biomarker; explains awareness of bowel activity and urgency
3. Gut-Brain Axis Dysregulation
- Altered central pain processing (central sensitization)
- Psychological stress exacerbates symptoms; anxiety and depression are common comorbidities
4. Post-Infectious IBS (PI-IBS)
- Occurs after acute gastroenteritis (bacterial, viral, parasitic)
- Risk factors: female sex, prolonged illness, psychological distress at time of infection, elevated mucosal inflammatory markers
- Mediated by increased mucosal enterochromaffin cells, increased 5-HT, altered microbiome
5. Altered Gut Microbiome
- Dysbiosis documented; role in symptom generation under active investigation
6. Serotonin (5-HT) Dysregulation
- 95% of serotonin is in the gut (enterochromaffin cells)
- 5-HT4 agonists (e.g., prucalopride) help IBS-C; 5-HT3 antagonists (e.g., alosetron) help IBS-D
(Sleisenger and Fordtran's GI & Liver Disease, pp. 2471-2473)
IBS: Alarm Features (Red Flags - require further investigation)
- Rectal bleeding
- Unexplained weight loss
- Iron deficiency anemia
- Nocturnal symptoms (40% of IBS patients report this, but low PPV for organic disease)
- Onset after age 50 (OR 2.65 for organic disease)
- Family history of colon cancer, IBD, or celiac disease
Important: Alarm features do NOT exclude IBS; 83% of IBS patients report at least one red flag. They guide additional workup, not exclusion of the diagnosis.
IBS vs. Functional Constipation: Key Distinction
| Feature | Functional Constipation | IBS-C |
|---|---|---|
| Abdominal pain | Absent or minimal | Present (mandatory) |
| Pain-defecation relationship | Not required | Pain linked to defecation |
| Stool changes | Yes | Yes |
| Bloating | Variable | Common (60%+) |
| Rome IV requirement | 2 of 6 stool symptoms | Recurrent pain + 2 of 3 criteria |
These conditions exist on a spectrum - Rome IV explicitly recognizes overlap and that many patients move between functional constipation and IBS-C over time.
Sources:
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, pp. 271-284, 2469-2473
- Yamada's Textbook of Gastroenterology, 7th ed., pp. 730, 1465-1466
- Sabiston Textbook of Surgery, 28th ed., p. 2174
- Rome IV: Mearin F, Lacy BE, Chang L, et al. Gastroenterology 2016;150:1393-1407
This is a shared conversation. Sign in to Orris to start your own chat.