Stye
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Searching PubMed
hordeolum stye treatment
Here is a comprehensive overview of the stye (hordeolum):
Stye (Hordeolum)
Definition & Types
A hordeolum (stye) is an acute bacterial abscess of an eyelid gland. There are two types:
| Feature | External Hordeolum (Stye) | Internal Hordeolum |
|---|---|---|
| Gland involved | Lash follicle + gland of Zeis (sebaceous) or Moll (sweat) | Meibomian gland |
| Location | Lid margin, at the base of a lash | Tarsal plate (inner surface of eyelid) |
| Pointing | Anteriorly through the skin | On the inner palpebral conjunctival surface |
| Demographics | Common in children and young adults | Similar |
— Kanski's Clinical Ophthalmology, p. 81; Tintinalli's Emergency Medicine, p. 1581
Causative Organism
Staphylococcus aureus is the predominant pathogen. Acute blepharitis frequently co-exists with or predisposes to hordeolum formation.
Clinical Features
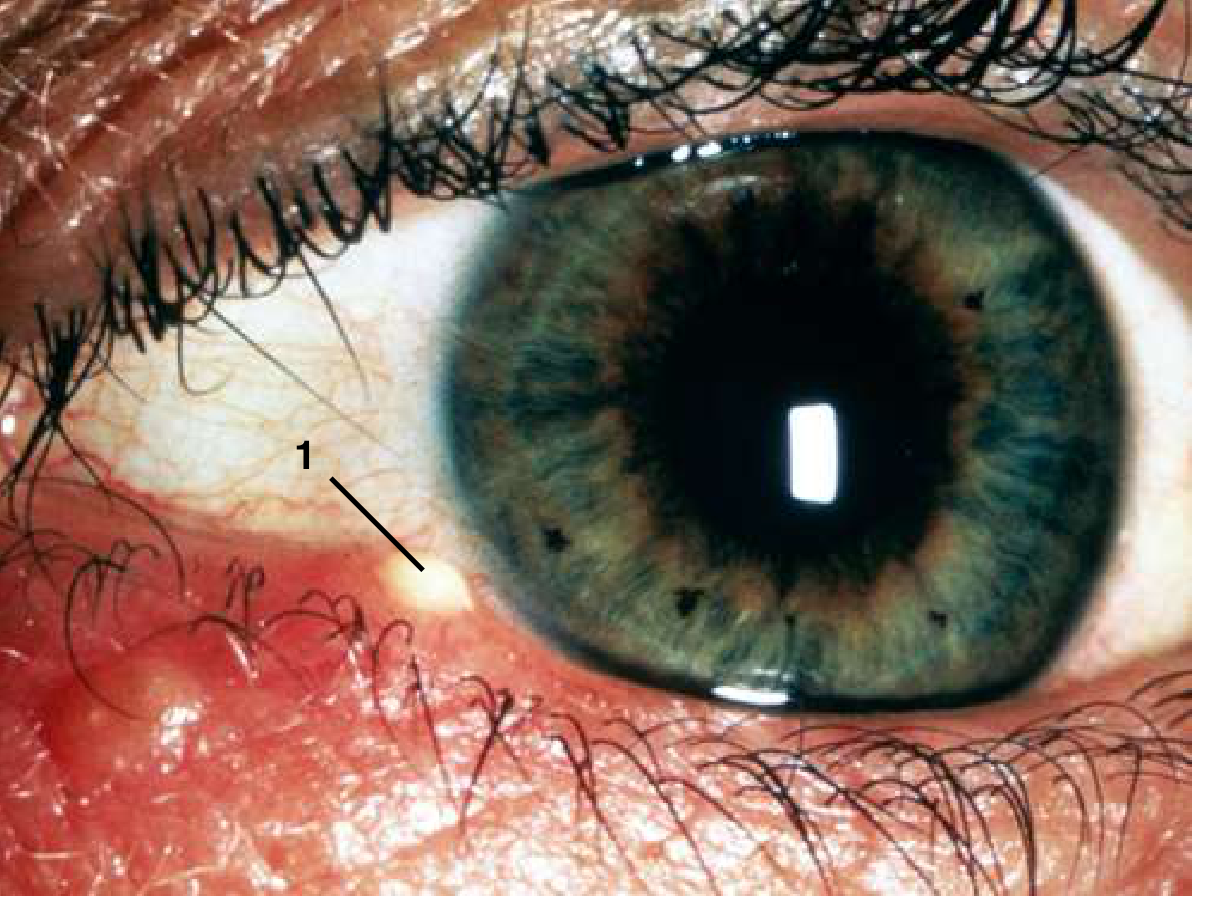
- Acute tender, erythematous swelling at the lid margin
- Small pustule at the margin, often with a lash at the apex (external type)
- Pain, edema, and erythema of the eyelid
- May be accompanied by eyelid cellulitis (erythema, edema, and tenderness of surrounding skin)
- Spontaneous drainage typically occurs within 5–7 days
- Multiple lesions may occur simultaneously, occasionally involving the entire lid margin
Differentiating from Chalazion
| Feature | Hordeolum | Chalazion |
|---|---|---|
| Onset | Acute | Subacute to chronic |
| Tenderness | Marked, tense, fluctuant | Mild or absent |
| Pus | Yes | No (lipogranulomatous content) |
| Cellulitis | Often present | Minimal or absent |
| Gland | Zeis, Moll, or meibomian | Meibomian (occluded) |
| Resolution | Usually drains in 5–7 days | May persist weeks |
⚠️ If swelling is nasal to the medial canthus, consider dacryocystitis — refer to ophthalmology promptly, as it can dissect posteriorly to the cavernous sinus.
— Pfenninger and Fowler's Procedures for Primary Care, p. 458
Treatment
Conservative (first-line)
- Warm compresses — applied frequently (4×/day); promotes spontaneous drainage
- Topical antibiotics — erythromycin or bacitracin ointment, or fluoroquinolone drops (moxifloxacin, gatifloxacin) for 7–10 days
- Epilation of the associated lash (external hordeolum)
- Systemic antibiotics if significant surrounding cellulitis is present
Incision and Drainage (I&D) — when indicated
- Failure of medical management
- Significant pain
- Significant localized pus collection
- Associated or prior eyelid cellulitis
Technique: After topical/local anesthesia (2% lidocaine with epinephrine), the hordeolum is incised from the side that allows the best access — externally if pointing through the skin, internally if pointing through the conjunctiva. A tongue blade or metal elevator supports the lid; a no. 11 blade scalpel is used to incise and drain.
Contraindication to I&D: Lesion near the lacrimal punctum (nasal to medial canthus) → refer to ophthalmology to avoid damaging the lacrimal drainage system.
— Pfenninger and Fowler's Procedures for Primary Care, p. 459; Goldman-Cecil Medicine; Tintinalli's Emergency Medicine, p. 1581
When to Refer
- No improvement within 48 hours of conservative treatment
- Suspected lacrimal involvement (nasal location)
- Recurrent lesions in the same location (may indicate an underlying carcinoma in the case of chalazia)
- Significant orbital or preseptal cellulitis
This is a shared conversation. Sign in to Orris to start your own chat.