

IMG-20260620-WA0019.jpg
IMG-20260620-WA0018.jpg
Diagnosis and treatment
Reading File
Searching PubMed
obstructive jaundice elevated direct bilirubin diagnosis
Finding Sources
Finding Sources
Searching PubMed
"jaundice"[MeSH Terms] AND "cholestasis"[MeSH Terms]
Reading File
Reading File
Reading File
I now have enough textbook information to provide a thorough analysis. Here is the complete report:
Lab Report Analysis - Mathurbhai Pateliya (50 yr/M, 20/06/2026)
ABNORMAL VALUES SUMMARY
| Test | Result | Reference | Status |
|---|---|---|---|
| Haemoglobin | 12.9 g/dL | 13.5-17.0 | LOW |
| Total RBC | 3.92 mill/cmm | 4.6-6.2 | LOW |
| PCV | 37.60% | 40-54% | LOW |
| MCH | 32.91 pg | 27-31 pg | HIGH |
| SGPT (ALT) | 90 U/L | up to 40 | HIGH (2.25x) |
| Total Bilirubin | 12.0 mg/dL | 0.0-1.0 | HIGH (12x) |
| Direct Bilirubin | 10.0 mg/dL | up to 0.25 | HIGH (40x) |
| Indirect Bilirubin | 2.0 mg/dL | 0.1-1.0 | HIGH |
| Urine Bile Pigments | PRESENT (+) | Absent | ABNORMAL |
| Urine Bile Salts | PRESENT (+) | Absent | ABNORMAL |
| Urine Pus Cells | 12-14/hpf | <5 | HIGH |
PRIMARY DIAGNOSIS
Obstructive (Cholestatic) Jaundice
The pattern here is classic for obstructive/post-hepatic jaundice:
- Direct (conjugated) bilirubin is the dominant fraction - Direct 10.0 out of Total 12.0 mg/dL = 83% of total bilirubin is direct. In obstructive jaundice, direct bilirubin accounts for >50% of the total bilirubin elevation (Current Surgical Therapy 14e).
- Bile pigments AND bile salts both present in urine - conjugated bilirubin is water-soluble and spills into urine; this is a hallmark of post-hepatic obstruction.
- SGPT moderately elevated at 90 U/L (2.25x ULN) - mild-moderate liver injury. In obstructive jaundice, ALT elevation is typically well below the thousands seen in viral/ischemic hepatitis (Current Surgical Therapy 14e). This pattern fits.
The most common causes of extrahepatic cholestasis to consider here are:
- Choledocholithiasis (CBD stone) - most common benign cause; typically painful
- Cholangiocarcinoma or pancreatic head carcinoma - painless progressive jaundice; must be ruled out at age 50
- Biliary stricture
- Cholangitis (if fever is present)
SECONDARY FINDINGS
Mild Normocytic Anaemia
- Hb 12.9, RBC 3.92, PCV 37.6% - all mildly low
- MCV 95.92 fL (normal range 80-96) - normocytic
- This can be due to chronic disease/liver disease, or a component of haemolysis (indirect bilirubin is also mildly raised at 2.0 mg/dL)
Urinary Tract Infection (likely)
- 12-14 pus cells/hpf (normal <5) with raised epithelial cells (6-8)
- Bacteria noted (though "dashes" may mean trace/present)
- No red cells, casts, or crystals
RECOMMENDED WORKUP (Further Investigations)
To determine the CAUSE of obstructive jaundice, the following are needed urgently:
- Abdominal Ultrasound (USG) - First-line, non-invasive; assesses bile duct dilation, gallstones, liver parenchyma, pancreatic masses (Goldman-Cecil Medicine)
- Alkaline Phosphatase (ALP) + GGT - Key cholestatic enzymes; not done in this report. A 3-4x elevation in ALP supports cholestasis
- MRCP (Magnetic Resonance Cholangiopancreatography) - Best non-invasive imaging for biliary tree
- Serum Albumin + Prothrombin Time - Assess liver synthetic function
- Hepatitis B/C serology - Rule out viral hepatitis contributing to jaundice
- CA 19-9, CEA - Tumour markers if malignancy suspected
- Urine culture and sensitivity - Confirm UTI organism and guide antibiotic choice
- ERCP - Diagnostic and therapeutic if CBD stone confirmed
TREATMENT APPROACH
1. Obstructive Jaundice
- Definitive treatment depends on the cause - must image first
- If CBD stone: ERCP with sphincterotomy and stone removal is the treatment of choice
- If malignancy: surgical resection (Whipple procedure for pancreatic head) or biliary stenting for palliation
- Ursodeoxycholic acid may be used to relieve cholestasis symptoms
- Treat pruritus (from bile salt deposition): cholestyramine or antihistamines
- Ensure vitamin K supplementation (fat-soluble vitamin absorption is impaired with bile duct obstruction)
- Monitor for cholangitis (fever, RUQ pain, jaundice = Charcot's triad) - if present, broad-spectrum IV antibiotics + urgent biliary drainage
2. Urinary Tract Infection
- Urine culture result awaited
- Empirical oral antibiotic: Nitrofurantoin 100 mg BD x 5 days or Co-trimoxazole or Ciprofloxacin 500 mg BD x 3-5 days (pending culture)
- Increased fluid intake
3. Anaemia
- Investigate cause further (iron studies, B12/folate if needed)
- Treat underlying liver/biliary disease
IMMEDIATE CLINICAL PRIORITIES
This patient needs urgent imaging (USG abdomen) today. A Total Bilirubin of 12 mg/dL is severely elevated and the cause must be established urgently. If the patient has fever and/or right upper quadrant pain, cholangitis must be ruled out - which is a medical emergency requiring hospital admission and IV antibiotics.
Red flag symptoms to ask about:
- Fever and chills (suggests cholangitis)
- Clay/pale-colored stools (complete biliary obstruction)
- Dark tea-colored urine (already confirmed by urinalysis)
- Right upper quadrant or epigastric pain
- Weight loss (suggests malignancy)
- Itching/pruritus (bile salt deposition)
Sources: Harrison's Principles of Internal Medicine 22E | Goldman-Cecil Medicine | Current Surgical Therapy 14e - Sleisenger and Fordtran's Gastrointestinal and Liver Disease
Disclaimer: This analysis is for informational purposes and should be reviewed by the treating physician. Clinical correlation and further investigations are mandatory before diagnosis confirmation and definitive treatment.
What imaging findings would confirm CBD stone vs. pancreatic cancer?
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Excellent - I now have authoritative textbook images and data. Here is the complete imaging guide:
Imaging Findings: CBD Stone vs. Pancreatic Cancer
STEP 1 - Start with Abdominal Ultrasound (USG)
The first-line investigation for any patient with obstructive jaundice. Fast, cheap, no radiation.
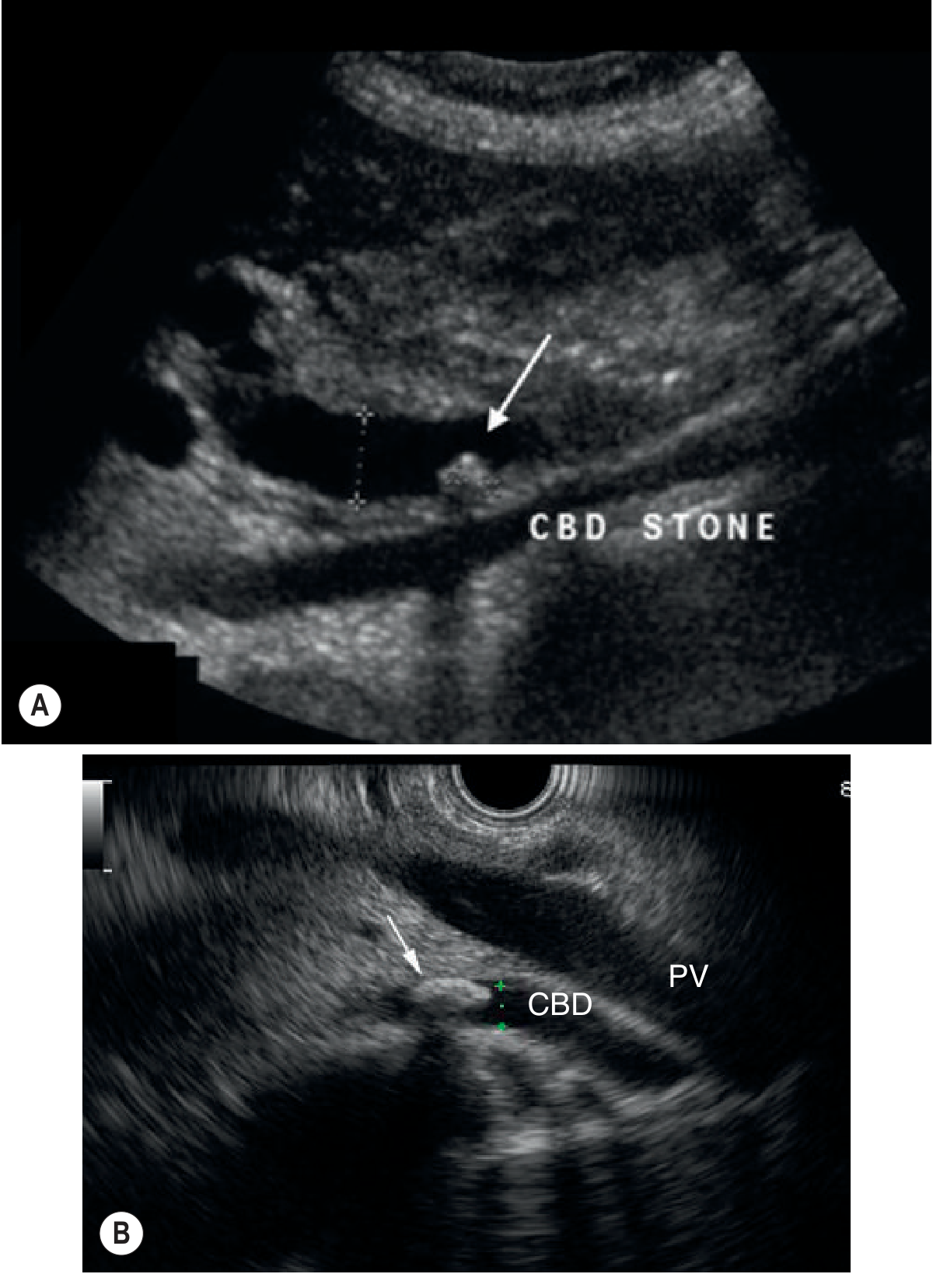
CBD Stone on USG
- Echogenic (bright/hyperechoic) focus within the duct lumen - seen in both longitudinal and transverse planes
- Acoustic shadowing posterior to the stone (dark shadow below the bright spot)
- CBD dilatation (>6 mm is significant; >8 mm strongly suggests obstruction)
- Gallstones may also be visible in the gallbladder
- USG sensitivity for CBD stones: 50-80%, specificity ~95%
- A CBD diameter <4 mm carries a high negative predictive value for stones
Pancreatic Cancer on USG
- Hypoechoic (dark) solid mass in the head of the pancreas
- CBD dilation + main pancreatic duct (MPD) dilation visible together
- Gallbladder may be dilated and palpable (Courvoisier's sign)
- USG is often limited by bowel gas for deep pancreatic lesions - not reliable enough to exclude cancer
STEP 2 - MRCP / CT Abdomen (Second-line, Definitive)
CBD Stone on MRCP
- Filling defect (dark rounded signal void) within the bright bile duct on T2 images
- Meniscus sign: crescent of bile around the stone
- No pancreatic duct dilation - this is key
- The CBD ends in a smooth, rounded obstruction
- MRCP pooled sensitivity 92-94%, specificity 99% for cholelithiasis
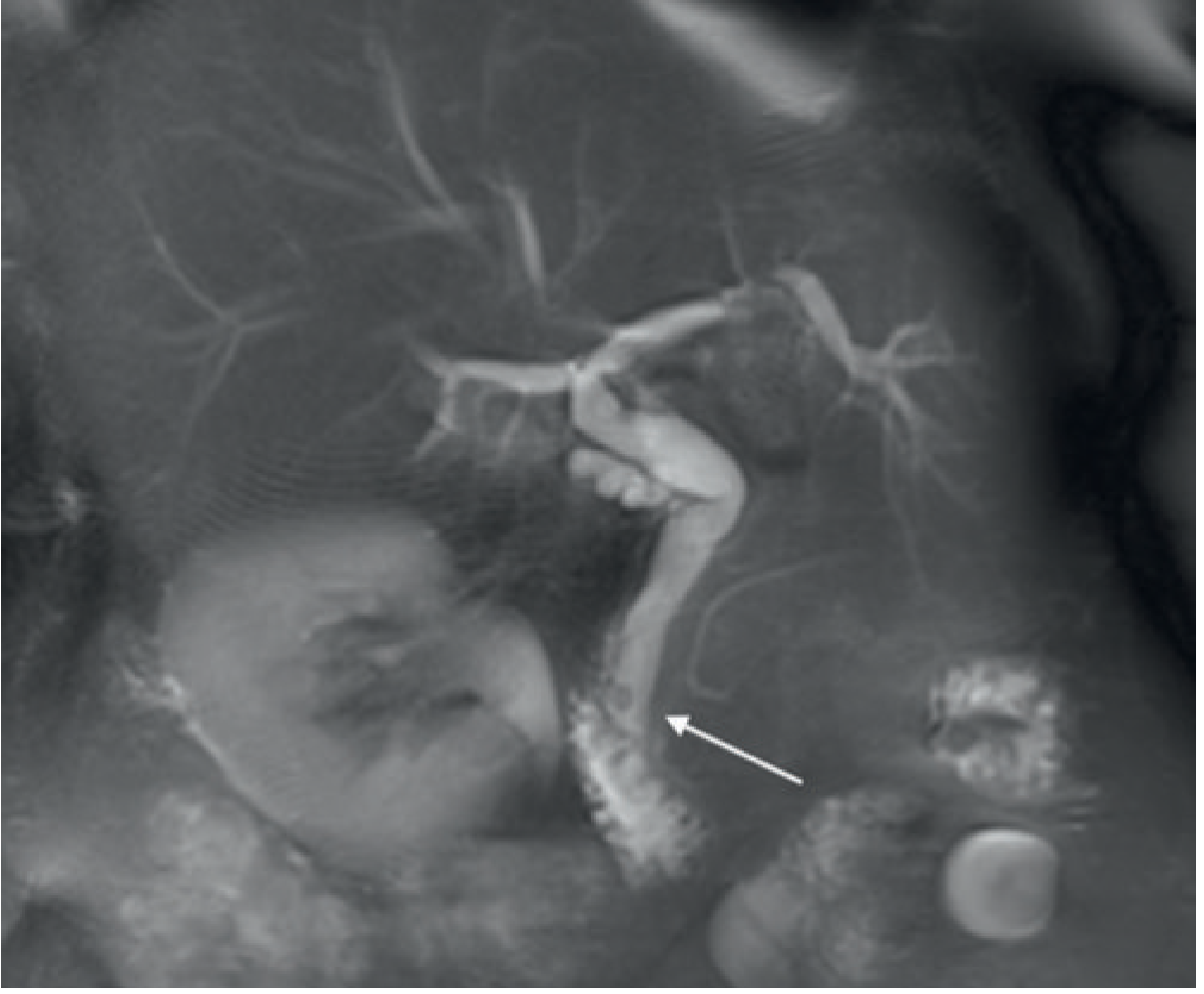
Pancreatic Cancer on CT/MRCP - The KEY Signs
Direct signs (CT - contrast enhanced):
- Hypoattenuating (hypodense) mass in the pancreatic head that enhances poorly compared to surrounding normal pancreatic tissue
- The tumour is hypovascular - this is best seen in the pancreatic parenchymal phase (~40 sec after contrast)
- 11% of tumours are isoattenuating on CT and may be invisible - rely on indirect signs then
Indirect signs (when no obvious mass is visible):
| Sign | Meaning |
|---|---|
| Double Duct Sign | BOTH CBD and main pancreatic duct dilated simultaneously - most specific sign |
| Biliary duct dilation alone | Suggests obstruction at head |
| Pancreatic duct dilation + upstream atrophy | Obstructed MPD → gland wastes away |
| Abrupt duct cut-off on MRCP | Sharp, shouldered or blunt cut-off rather than smooth tapering |
| Focal loss of pancreatic lobulation | Subtle early sign |
| Distorted pancreatic contour | Mass effect from tumour |
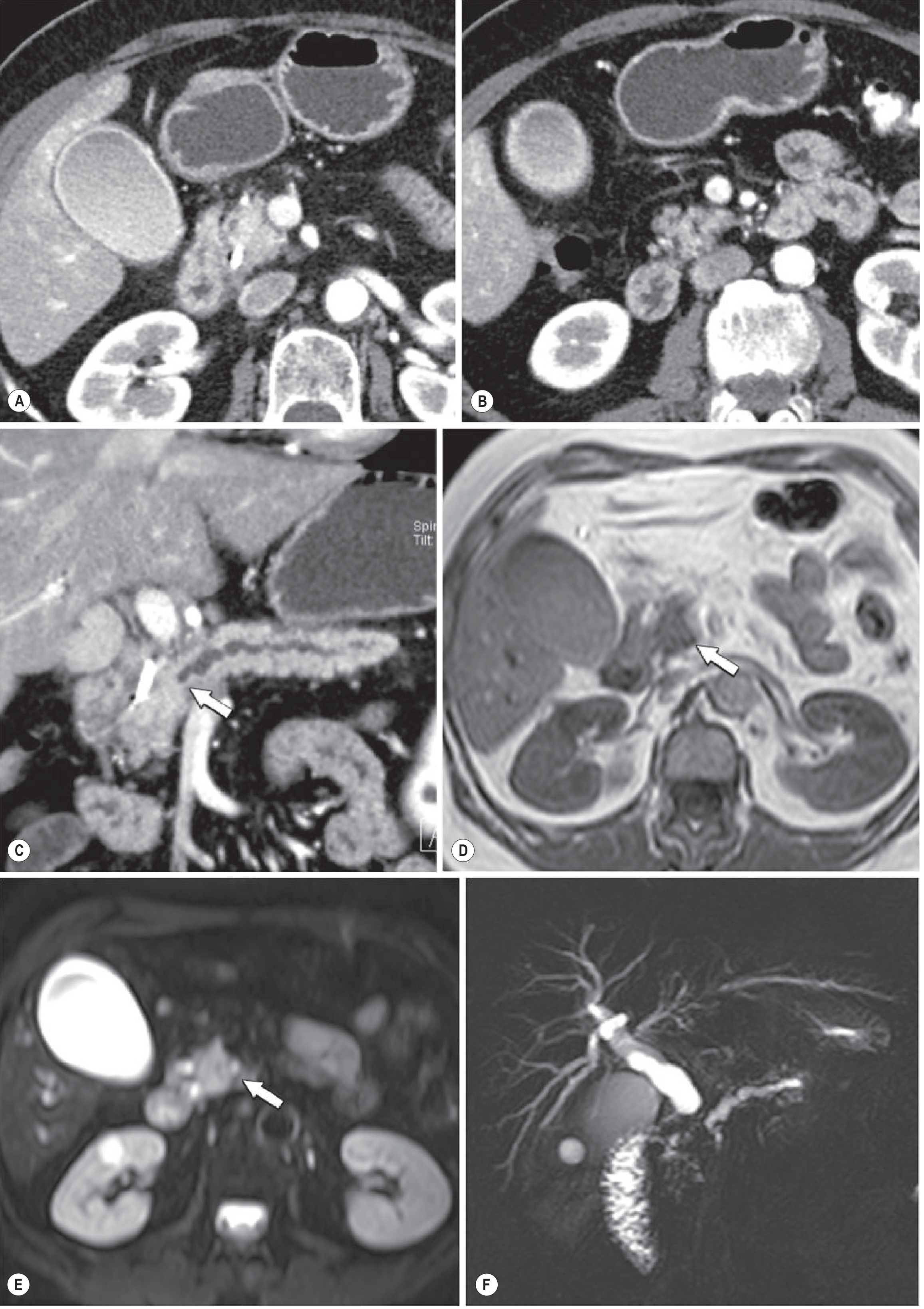
The double-duct sign on MRCP (simultaneous dilation of CBD + MPD) occurs in 77% of pancreatic head carcinomas and is highly suspicious for malignancy (Yamada's Textbook of Gastroenterology). On cholangiography, pancreatic carcinoma produces a tight, shouldered stricture with a blunt or convex cut-off of the bile duct - very different from the smooth rounded filling defect of a stone.
HEAD-TO-HEAD COMPARISON TABLE
| Feature | CBD Stone | Pancreatic Cancer |
|---|---|---|
| USG | Echogenic focus + acoustic shadow in duct | Hypoechoic mass in pancreatic head |
| CBD dilation | Yes | Yes |
| MPD (pancreatic duct) dilation | No | Yes - key differentiator |
| Double duct sign | Absent | Present in 77% |
| CT mass | No mass | Hypodense, poorly enhancing mass |
| MRCP filling defect | Rounded, smooth dark defect with bile crescent | Tight shouldered/blunt duct cut-off |
| Gallbladder | May have stones | Enlarged, non-tender (Courvoisier) |
| Vascular involvement | None | SMA/SMV encasement indicates unresectability |
| Liver metastases | Absent | May be present (advanced disease) |
| Clinical clue | Often painful, colicky | Often painless progressive jaundice |
STEP 3 - EUS (Endoscopic Ultrasound) - If Still Uncertain
- Sensitivity >90% for CBD stones, higher than transabdominal USG
- For pancreatic cancer: allows direct visualisation and EUS-guided fine needle aspiration (FNA) for tissue diagnosis - this is how you confirm cancer histologically
- Also assesses regional lymph nodes and vascular involvement
STEP 4 - ERCP - Therapeutic, not just Diagnostic
- If CBD stone confirmed on MRCP/EUS: proceed to ERCP + sphincterotomy + stone extraction
- If stricture with suspicion of malignancy: ERCP allows biliary stenting for palliation + brush cytology biopsy
- For pancreatic cancer, ERCP also shows the "tight shouldered stricture" of the distal CBD
Recommended Sequence for This Patient
USG Abdomen (today, urgent)
|
Stone seen? → Yes → ERCP (diagnostic + therapeutic)
|
No / Inconclusive
|
MRCP
|
Double duct sign / Pancreatic mass? → Yes → Contrast CT Abdomen for staging
+ EUS-FNA for tissue diagnosis
+ CA 19-9, CEA markers
|
No → Consider other causes (cholangiocarcinoma, stricture, ampullary carcinoma)
Sources: Grainger & Allison's Diagnostic Radiology | Yamada's Textbook of Gastroenterology 7e | Current Surgical Therapy 14e | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.