Just give me and explain me heparin and warfarrin moa toxicity contraindications everything
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a thorough answer. Let me compile the complete response.
Heparin and Warfarin - Complete Pharmacology Guide
HEPARIN
Chemistry
Heparin is a heterogeneous mixture of sulfated mucopolysaccharides (glycosaminoglycans), isolated from mammalian tissues rich in mast cells. Most commercial preparations are derived from porcine intestinal mucosa. It is a polymer of alternating D-glucuronic acid and N-acetyl-D-glucosamine residues, with a molecular weight range of 5,000-30,000 Da.
Mechanism of Action (MOA)
Heparin does not act directly - it works through antithrombin (AT-III), an endogenous serine protease inhibitor made in the liver.
Step-by-step:
- Heparin binds to antithrombin via a unique pentasaccharide sequence (found on only ~1/3 of commercial heparin chains).
- This binding causes a conformational change in antithrombin, exposing its active site.
- The activated antithrombin then rapidly inhibits clotting factors - especially thrombin (IIa) and factor Xa, but also IXa, XIa, XIIa.
- Heparin is released intact and recycled - it acts as a cofactor, not consumed.
Key distinction:
- For factor Xa inhibition: the pentasaccharide-antithrombin conformational change is enough (no need for long chain).
- For thrombin inhibition: heparin must bridge antithrombin and thrombin simultaneously - requires chains of at least 18 saccharide units. This is why UFH (long chains) inhibits both Xa and IIa equally (ratio 1:1), while LMW heparins (shorter chains) preferentially inhibit Xa.
Heparin also causes release of Tissue Factor Pathway Inhibitor (TFPI) from endothelium.
Pharmacokinetics
| Feature | UFH | LMWH (e.g. enoxaparin) |
|---|---|---|
| Route | IV or SC (NOT IM) | SC |
| Bioavailability | ~30% (SC) | ~90% (SC) |
| Half-life | ~1 hour | ~4 hours |
| Renal excretion | No | Yes |
| Monitoring | aPTT (target 1.5-2.5x normal) | Not usually needed |
| Antidote | Protamine (complete) | Protamine (partial ~60%) |
Indications
- DVT and PE treatment and prophylaxis
- Acute coronary syndromes (NSTEMI, STEMI)
- Prevention of thrombosis in cardiac/arterial surgery (e.g. cardiopulmonary bypass)
- Bridging anticoagulation (when stopping warfarin peri-procedurally)
- Pregnancy (does not cross placenta - safe)
Monitoring
- UFH: aPTT - therapeutic range is 1.5-2.5x the control value (or 60-100 seconds). Can also monitor by anti-Xa units (therapeutic: 0.3-0.7 unit/mL).
- LMWH: anti-Xa levels in special populations (renal insufficiency, obesity, pregnancy). Therapeutic peak for enoxaparin (twice-daily): 0.5-1 unit/mL at 4 hrs post-dose.
Toxicity / Adverse Effects
1. Bleeding (Major)
The primary adverse effect. Risk is higher in elderly women and patients with renal failure. Managed by:
- Stopping heparin (half-life only ~1 hour for UFH)
- Protamine sulfate for reversal (1 mg per 100 units UFH; neutralizes by forming stable salt complex). Protamine only partially reverses LMWH (~60% of anti-Xa activity).
2. Heparin-Induced Thrombocytopenia (HIT)
This is the most serious non-bleeding complication.
- Occurs in 1-4% of UFH patients (surgical > medical patients)
- HIT Type I (non-immune): mild, transient fall in platelets within 1-2 days, self-limiting
- HIT Type II (immune-mediated, more serious): antibodies form against heparin-PF4 complex, activating platelets paradoxically, causing a pro-thrombotic (not bleeding) state
- Onset: 5-14 days after starting heparin
- Characterized by: thrombocytopenia + new thrombosis (venous or arterial)
- Platelet count typically drops >50% from baseline
- Management: stop all heparin immediately (including flushes), switch to a direct thrombin inhibitor (e.g. argatroban)
- Do NOT give warfarin until platelets recover (risk of skin necrosis via protein C depletion)
3. Osteoporosis
Long-term heparin use (>3-6 months) can cause bone demineralization and spontaneous fractures via osteoclast activation.
4. Other
- Transient alopecia (hair loss)
- Hypoaldosteronism (mineralocorticoid deficiency) - can cause hyperkalemia
- Release of lipoprotein lipase - can cause hyperlipidemia reduction (triglyceride clearing)
- Hypersensitivity (animal origin)
Contraindications
- Active HIT or history of HIT
- Active uncontrolled bleeding or hemorrhagic disorders (hemophilia, significant thrombocytopenia, purpura)
- Intracranial hemorrhage or recent brain/spinal cord/eye surgery
- Severe uncontrolled hypertension
- Infective endocarditis (relative)
- Active peptic ulcer / GI ulcerative lesions
- Threatened abortion / visceral carcinoma
- Advanced hepatic or renal disease
- Hypersensitivity to heparin
WARFARIN
History & Chemistry
Warfarin (Wisconsin Alumni Research Foundation + "-arin" from coumarin) was initially developed as a rodenticide before becoming an antithrombotic agent in humans in the 1950s. It is a vitamin K antagonist (VKA) and was the only oral anticoagulant for over 60 years.
Mechanism of Action (MOA)
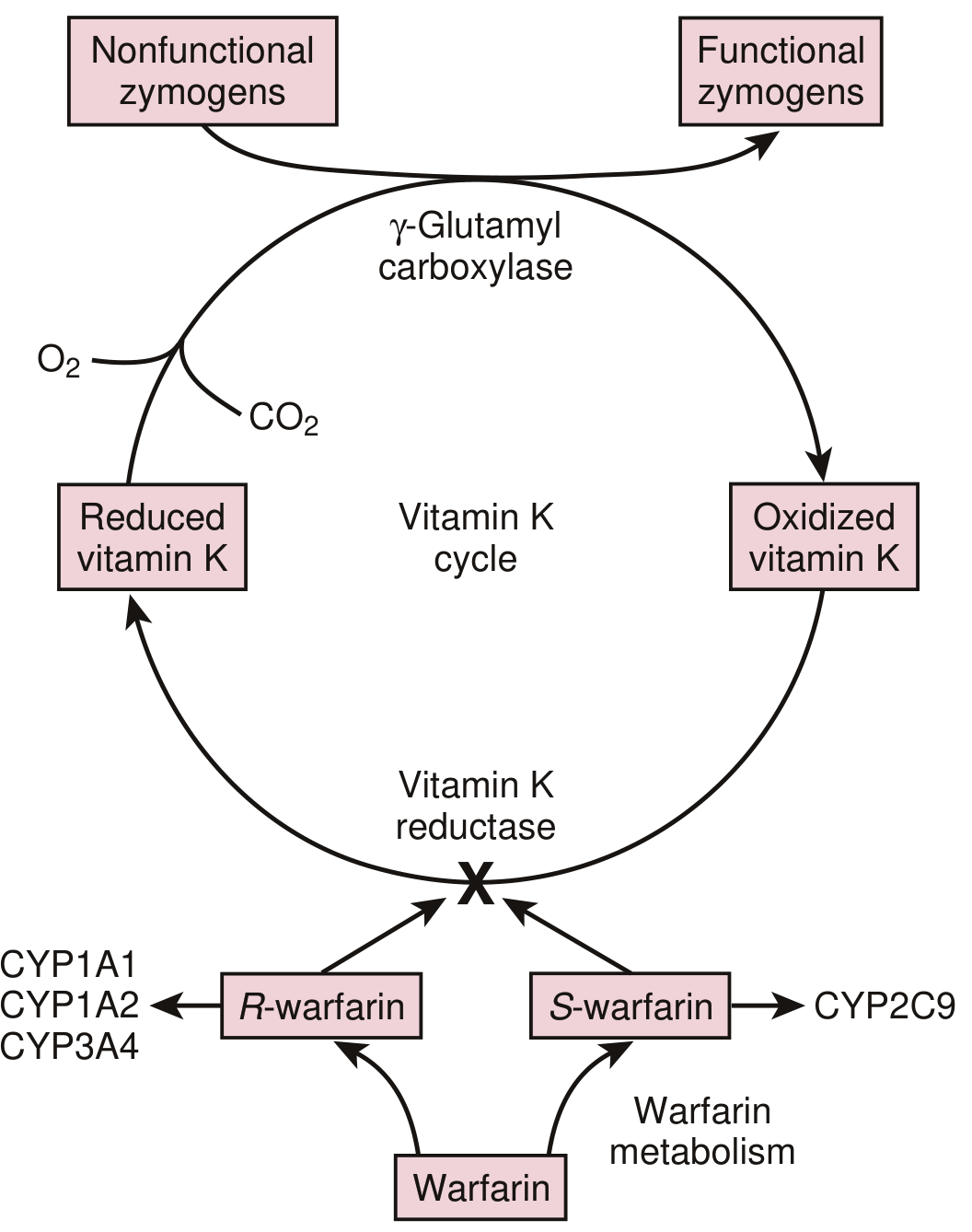
Warfarin works by blocking the Vitamin K Cycle:
-
Normal physiology: Dietary vitamin K is reduced to vitamin K hydroquinone (KH₂) by vitamin K reductase. KH₂ acts as a cofactor for gamma-glutamyl carboxylase, which adds a carboxyl group to glutamic acid residues on clotting factors (gamma-carboxylation). This carboxylation is essential for calcium-dependent binding of factors to phospholipid surfaces (activation). During this process, KH₂ is oxidized to vitamin K epoxide, then recycled back by vitamin K epoxide reductase (VKORC1).
-
Warfarin's action: Warfarin inhibits VKORC1 - blocking the regeneration of active reduced vitamin K. Without active vitamin K, gamma-carboxylation fails, producing clotting factors that are structurally present but functionally inactive ("PIVKA" - proteins induced by vitamin K absence).
-
Affected factors: Warfarin impairs synthesis of factors II (prothrombin), VII, IX, X (clotting factors) and also Protein C and Protein S (anticoagulants).
Important consequence: Protein C has the shortest half-life (~6 hours), so it falls first when warfarin is started - causing a transient pro-thrombotic state in the first 1-2 days. This is why heparin bridging is required at initiation in high-risk patients.
Pharmacokinetics
- Route: Oral; 100% bioavailability
- Absorption: Rapid, peak levels at ~90 minutes
- Plasma protein binding: >99% bound to albumin (only free fraction is active)
- Half-life: 36-42 hours (racemic mixture)
- Distribution: Small volume of distribution (albumin space); accumulates in the liver
- Metabolism: Hepatic
- S-warfarin (4x more potent): metabolized by CYP2C9
- R-warfarin: metabolized by CYP1A2, CYP3A4
- Excretion: Urinary (as metabolites); no unchanged drug in urine
Onset of anticoagulation: Delayed by 3-5 days (time needed for existing active clotting factors to be cleared - prothrombin has a half-life of 72 hours).
Pharmacogenomics
Two key genetic variants affect warfarin dosing:
| Gene | Variant | Effect |
|---|---|---|
| CYP2C9 | *2, *3 alleles | Reduced S-warfarin metabolism → need lower doses; increased bleeding risk |
| VKORC1 | A haplotype (common in Asians) | More sensitive to warfarin → need much lower doses |
~25% of white patients carry at least one CYP2C9 variant allele. Asians have much higher frequency of the VKORC1 A haplotype (~63%), explaining their lower dose requirements.
Indications
- Atrial fibrillation (stroke prevention)
- Mechanical heart valves (mandatory - DOACs not used here)
- DVT/PE treatment and secondary prevention
- Antiphospholipid syndrome
- Rheumatic mitral stenosis with AF
Monitoring
- INR (International Normalized Ratio) - derived from prothrombin time (PT)
- Target INR: 2.0-3.0 for most indications (AF, DVT/PE)
- Target INR: 2.5-3.5 for mechanical mitral valves
- Must be monitored regularly (especially at initiation, dose changes, illness, new medications)
Toxicity / Adverse Effects
1. Bleeding (Major - Most Common)
Any site: GI, intracranial (most dangerous), urinary, skin, surgical sites.
Reversal strategy based on urgency:
- Mild bleeding / elevated INR only: Reduce or hold dose; oral vitamin K
- Significant bleeding: IV/oral vitamin K + Fresh Frozen Plasma (FFP) (contains all clotting factors)
- Life-threatening bleeding: IV vitamin K + 4-factor Prothrombin Complex Concentrate (4F-PCC) or FFP - fastest reversal
- INR correction with vitamin K takes 6-24 hours even IV; PCC is immediate
2. Warfarin-Induced Skin Necrosis
- Rare but serious complication, typically occurring in days 3-5 of therapy
- Caused by early depletion of Protein C (short half-life) before factors II, IX, X are depleted
- Leads to microvascular thrombosis in skin - painful necrotic skin lesions in fatty areas (breasts, buttocks, thighs, abdomen)
- Higher risk in patients with Protein C or S deficiency
- Prevention: overlap with heparin until full therapeutic INR is established
3. Teratogenicity (Warfarin Embryopathy)
- Warfarin crosses the placenta - absolutely contraindicated in 1st trimester
- Causes: warfarin embryopathy (nasal hypoplasia, stippled epiphyses, skeletal abnormalities) in weeks 6-12
- Also causes fetal/neonatal hemorrhage and CNS abnormalities
4. "Purple Toe Syndrome"
- Rare - cholesterol microembolization to toes after warfarin initiation, causing painful purple discoloration
5. Drug Interactions (Extensive)
Warfarin has more clinically significant drug interactions than almost any other drug:
Drugs that INCREASE warfarin effect (increase bleeding risk):
- CYP2C9 inhibitors: amiodarone, fluconazole, metronidazole, ciprofloxacin
- Protein displacement from albumin: NSAIDs, aspirin
- Decreased vitamin K synthesis: broad-spectrum antibiotics (kill gut flora)
- Direct additive: aspirin, NSAIDs (platelet effects + GI bleeding)
Drugs that DECREASE warfarin effect (increase clotting risk):
- CYP inducers: rifampin (most potent), carbamazepine, phenytoin, barbiturates, St. John's Wort
- Vitamin K supplementation or diet high in leafy greens (spinach, broccoli, kale)
- Cholestyramine (reduces warfarin absorption)
Contraindications
- Pregnancy (especially 1st trimester and near term) - absolute
- Active uncontrolled bleeding
- Hemorrhagic stroke or intracranial hemorrhage
- Severe uncontrolled hypertension
- Protein C or S deficiency (risk of skin necrosis - use with extreme caution; must bridge with heparin)
- Recent brain, spinal cord, or eye surgery
- Patients unable to comply with monitoring (INR monitoring is mandatory)
- Significant hepatic disease (already impaired clotting factor synthesis)
- Falls risk / history of recurrent falls (relative contraindication)
Side-by-Side Comparison
| Feature | Heparin (UFH) | Warfarin |
|---|---|---|
| Route | IV / SC | Oral |
| Onset | Immediate | 3-5 days (delayed) |
| MOA | Activates antithrombin → inhibits IIa & Xa | Inhibits VKORC1 → blocks Vit K recycling → reduces II, VII, IX, X, Protein C, S |
| Monitoring | aPTT | INR (PT) |
| Crosses placenta? | No (safe in pregnancy) | Yes (teratogenic) |
| Reversal | Protamine sulfate | Vitamin K + FFP/PCC |
| HIT risk | Yes (1-4%) | No |
| Skin necrosis | Possible in HIT setting | Yes (Protein C depletion, days 3-5) |
| Drug interactions | Fewer | Extensive (CYP2C9, food, many drugs) |
| Use in pregnancy | Safe | Contraindicated (1st trimester) |
Key clinical pearl: When starting anticoagulation in an acute thrombus, heparin is used first because warfarin's onset is delayed AND warfarin's early effect is actually pro-thrombotic (Protein C falls first). Heparin must overlap with warfarin for at least 5 days AND until INR is therapeutic for 2 consecutive days before heparin is stopped.
Sources: Katzung's Basic and Clinical Pharmacology, 16th Ed.; Braunwald's Heart Disease, 15th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.