Microbiology of torch infection
Reading File
Finding Sources
Finding Sources
Searching the Web
TORCH infections microbiology toxoplasma rubella cytomegalovirus herpes
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have extensive content from multiple authoritative textbooks. Let me compile the comprehensive answer.
TORCH Infections - Microbiology
What is TORCH?
TORCH is an acronym coined in the early 1970s for a group of congenital/perinatal infections that share overlapping presentations - skin lesions, ocular disease, and CNS involvement. The letters stand for:
| Letter | Organism |
|---|---|
| T | Toxoplasma gondii (protozoan parasite) |
| O | Other - syphilis (Treponema pallidum), VZV, parvovirus B19, Zika virus, Listeria, enteroviruses, HIV, HBV, HCV |
| R | Rubella virus (Togavirus) |
| C | Cytomegalovirus - CMV (Herpesviridae) |
| H | Herpes Simplex Virus - HSV-1/2 (Herpesviridae) |
The "O" (Other) has expanded considerably since the original description. Some formulations use TORCHES or STORCH to explicitly include Syphilis.
- Sherris & Ryan's Medical Microbiology, 8th Ed.
- Tietz Textbook of Laboratory Medicine, 7th Ed.
Routes of Transmission
| Route | Organisms |
|---|---|
| Transplacental | T. gondii, rubella virus, CMV, syphilis, HIV, Zika virus, parvovirus B19, VZV |
| Intrapartum (birth canal) | HSV-2, CMV (cervical secretions), GBS, N. gonorrhoeae, C. trachomatis |
| Breast milk | CMV, HIV, HCV |
The gestational age at infection is more important than the specific organism in determining the pattern of CNS injury. - Grainger & Allison's Diagnostic Radiology
T - Toxoplasma gondii
- Type: Obligate intracellular protozoan parasite
- Source: Ingestion of oocysts from undercooked meat or cat feces (maternal primary infection)
- Transmission: Transplacental; rate increases from ~30% at 6 months' gestation approaching 100% at term
- Incidence: ~0.01-0.1% of live births (about 1/10th the rate of congenital CMV)
- Classic triad: Chorioretinitis + Hydrocephalus + Intracranial calcifications (the complete triad is rare)
- Other features: 70-90% asymptomatic at birth; anemia, thrombocytopenia, jaundice, hepatosplenomegaly, seizures
- Imaging: Parenchymal calcifications similar to CMV; ventriculomegaly from obstructive hydrocephalus (ependymitis); notably NO cerebellar hypoplasia or polymicrogyria
- Treatment: Pyrimethamine + sulfadiazine + folinic acid
O - "Other" Agents
Treponema pallidum (Syphilis)
- Type: Gram-negative spirochete bacterium
- Transmission: Transplacental at any stage of pregnancy
- Early features: Snuffles (nasal discharge), mucous membrane lesions, hepatosplenomegaly, maculopapular rash, osteochondritis, anemia, thrombocytopenia
- Late features (months-years later): Hutchinson's teeth, keratitis, saddle nose, saber shins, CNS syphilis
- Prevention/Treatment: Maternal screening + penicillin G
Varicella-Zoster Virus (VZV)
- Type: Herpesvirus (DNA)
- Transmission: Transplacental
- Features: Skin scarring, limb hypoplasia, neurological defects, chorioretinitis
- Prevention: VZV vaccination before pregnancy
Parvovirus B19
- Type: Single-stranded DNA virus (Erythrovirus)
- Transmission: Transplacental
- Key effect: Hydrops fetalis from aplastic crisis (infects erythroid precursors)
Zika Virus
- Type: Flavivirus (RNA), transmitted by Aedes mosquitoes (unique among TORCH)
- Features: Microcephaly, hypertonia, ocular abnormalities, hearing loss, seizures ("congenital Zika syndrome")
- Note: No specific treatment; first recognized clinically in 2015 (Brazil outbreak)
R - Rubella Virus
- Type: Togavirus (single-stranded positive-sense RNA), genus Rubivirus
- Transmission: Transplacental (respiratory droplet-acquired in mother, then crosses placenta)
- Timing matters: First 8 weeks - cataracts, glaucoma, cardiac defects; severity decreases as pregnancy progresses; third trimester infection may be asymptomatic
- Classic triad (Congenital Rubella Syndrome - CRS): Sensorineural hearing loss + Cataracts + Cardiac defects (PDA, pulmonary artery stenosis) - in a small-for-gestational-age infant
- Other features: Microphthalmia, chorioretinitis, "blueberry muffin rash" (purpura/petechiae from thrombocytopenia), hepatosplenomegaly
- Epidemiology: Eliminated in the US since 2004 after MMR vaccination; still >100,000 cases/year worldwide; immigrant populations remain at risk
- Prevention: MMR vaccination (live-attenuated) before pregnancy
C - Cytomegalovirus (CMV)
- Type: Herpesviridae (double-stranded DNA); Human Herpesvirus 5 (HHV-5)
- Transmission: Transplacental (primary or reactivation), intrapartum (cervix), breast milk
- Most common serious congenital viral infection in developed countries: 0.5-1% of all births (~40,000 infants/year in the US)
- ~90% are asymptomatic at birth
- Symptomatic features: Small for gestational age, petechiae/purpura, thrombocytopenia, jaundice/hepatitis, chorioretinitis, microcephaly, periventricular intracranial calcifications (most characteristic), sensorineural hearing loss (can develop up to 2 years post-birth)
- Imaging signature: Periventricular calcifications (vs. scattered calcifications in toxoplasmosis); lenticulostriate vasculopathy on cranial US; timing of infection determines pattern:
- 2nd trimester: lissencephaly, thin cortex, cerebellar hypoplasia, ventriculomegaly
- Later: polymicrogyria, parenchymal damage, temporal pole cysts
- Pathogenesis: Direct viral insult to germinal matrix cells (periventricular); vascular insult; vertical transmission risk much higher with primary vs. recurrent CMV
- Treatment: Valganciclovir (reduces hearing loss and improves neurodevelopmental outcomes)
H - Herpes Simplex Virus (HSV)
- Type: Herpesviridae (double-stranded DNA); HSV-1 and HSV-2
- Transmission: Primarily perinatally - direct contact with maternal genital lesions during vaginal delivery (HSV-2 most common); congenital (transplacental) infection is quite rare
- Three clinical presentations of neonatal HSV:
- SEM disease - Skin, Eyes, Mucous membranes (visible vesicular lesions; best prognosis)
- CNS disease - encephalitis (rapidly disseminating, diffuse - unlike adult pattern of temporal lobe involvement)
- Disseminated - liver and lungs most commonly; highest mortality
- Imaging (CNS): Widespread asymmetrical regions of T2 hyperintensity in white matter; progressive cortical swelling; cerebral atrophy and cystic encephalomalacia develop rapidly (as early as week 2)
- Treatment: IV acyclovir (high doses; limits neurologic complications)
Summary Comparison Table
| Feature | Toxoplasma | Rubella | CMV | HSV |
|---|---|---|---|---|
| Organism type | Protozoan | RNA virus (Togavirus) | DNA virus (Herpesvirus) | DNA virus (Herpesvirus) |
| Main route | Transplacental | Transplacental | Transplacental/perinatal | Perinatal (birth canal) |
| Incidence (congenital) | 0.01-0.1% | Rare (vaccine eliminated) | 0.5-1% (most common) | Rare (congenital) |
| Calcifications | Diffuse/scattered | Uncommon | Periventricular | Not typical |
| Hearing loss | Possible | Yes (sensorineural) | Yes (progressive) | Possible |
| Chorioretinitis | Yes (classic) | Yes | Yes | Yes (rare) |
| Classic triad/feature | Chorioretinitis + Hydrocephalus + Calcifications | Hearing loss + Cataracts + Cardiac defects | Periventricular calcifications + Microcephaly + Deafness | SEM / CNS / Disseminated disease |
| Treatment | Pyrimethamine + sulfadiazine + folinic acid | None (prevention by MMR) | Valganciclovir | IV Acyclovir |
CT Scan of Congenital TORCH Infection
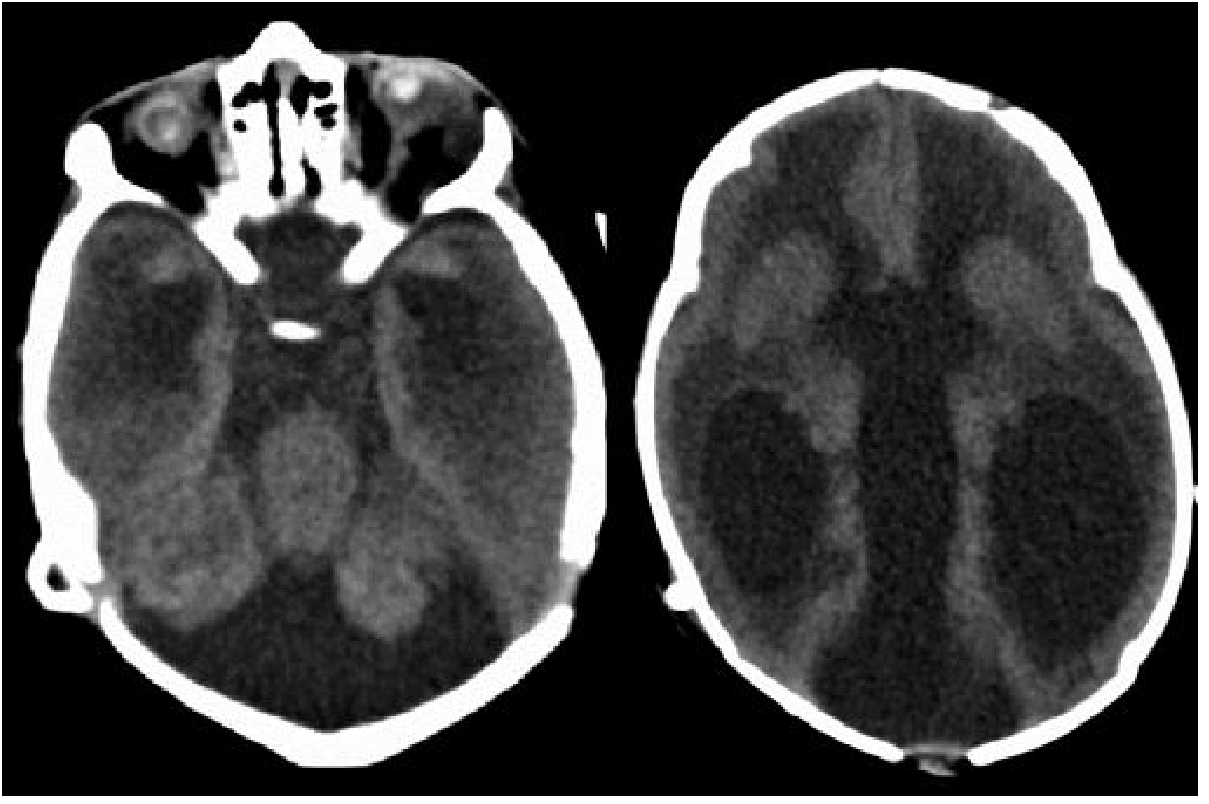
CT of a neonate with congenital TORCH infection. Note the small, calcified globes (phthisis bulbi), Dandy-Walker malformation, and hydrocephalus with transependymal edema. - Grainger & Allison's Diagnostic Radiology
Key Diagnostic Points
- TORCH titers have limited utility alone - serology cannot precisely determine timing of infection; can lead to unnecessary invasive procedures
- CMV is the most common cause - always include in workup for congenital infection
- The "O" category now includes VZV, enteroviruses, parvovirus B19, Zika virus, syphilis, HIV, HBV, HCV
- Gestational timing determines severity: infections before 16-18 weeks (neuronal migration phase) cause the most severe CNS malformations (lissencephaly); later infections cause gliosis, cystic change, calcification
Sources: Sherris & Ryan's Medical Microbiology 8th Ed. | Tietz Textbook of Laboratory Medicine 7th Ed. | Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.