Bladder outflow obstruction
Reading File
Finding Sources
Finding Sources
Searching PubMed
"bladder outlet obstruction" management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive material from three authoritative textbooks plus recent guidelines. Let me compose the full answer.
Bladder Outflow Obstruction (BOO)
Definition
BOO is a urodynamic concept defined by the combination of low urinary flow rates in the presence of high voiding pressures. It can only be diagnosed definitively by pressure-flow studies, because symptoms are non-specific and can also result from detrusor instability, neurological dysfunction, or weak bladder contractions.
- Bailey and Love's Short Practice of Surgery, 28th Ed., p. 1545
Causes
In men (most common):
- Benign prostatic hyperplasia (BPH) - the most frequent cause
- Bladder neck stenosis
- Bladder neck dyssynergia / functional bladder neck obstruction
- Bladder neck hypertrophy
- Prostate cancer
- Urethral stricture
- Functional obstruction from neuropathic conditions
In women (less common, diagnostically challenging):
-
Post anti-incontinence surgery (e.g. sling procedures)
-
Pelvic organ prolapse / cystocele
-
Primary bladder neck obstruction
-
Dysfunctional voiding
-
Urethral stricture
-
Bailey and Love's, p. 1545; Campbell-Walsh-Wein Urology, p. 3381
Urodynamic Parameters
Normal flow rate
The voided volume should be >200 mL for interpretation to be reliable.
| Flow Rate | Interpretation |
|---|---|
| >15 mL/s (voided vol >200 mL) | Normal |
| 10-15 mL/s | Equivocal |
| <10 mL/s | Low (suggestive of BOO) |
Voiding pressures (detrusor pressure at max flow)
| Pressure | Interpretation |
|---|---|
| >80 cmH₂O | High (obstructed) |
| 60-80 cmH₂O | Equivocal |
| <60 cmH₂O | Normal |
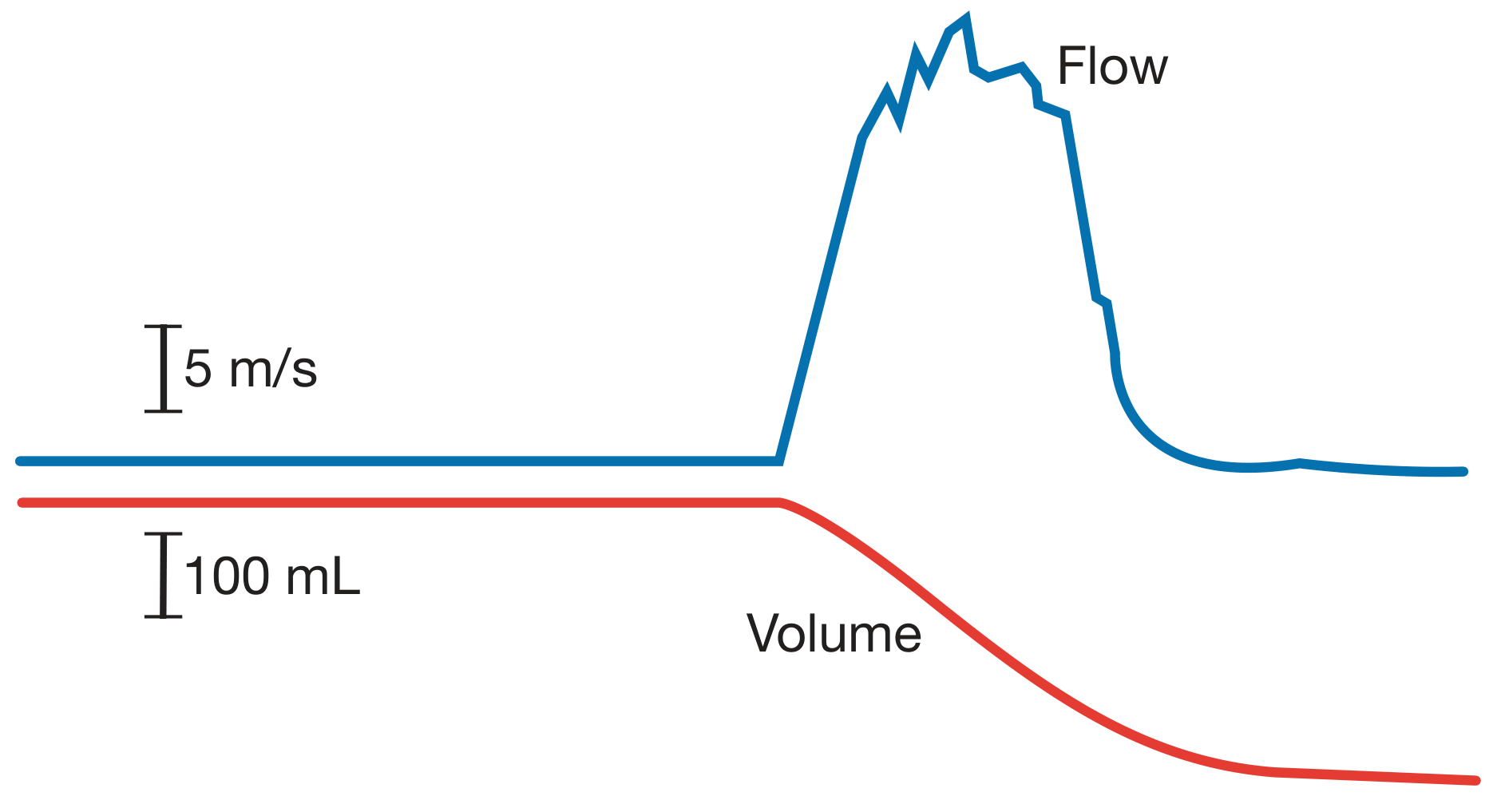
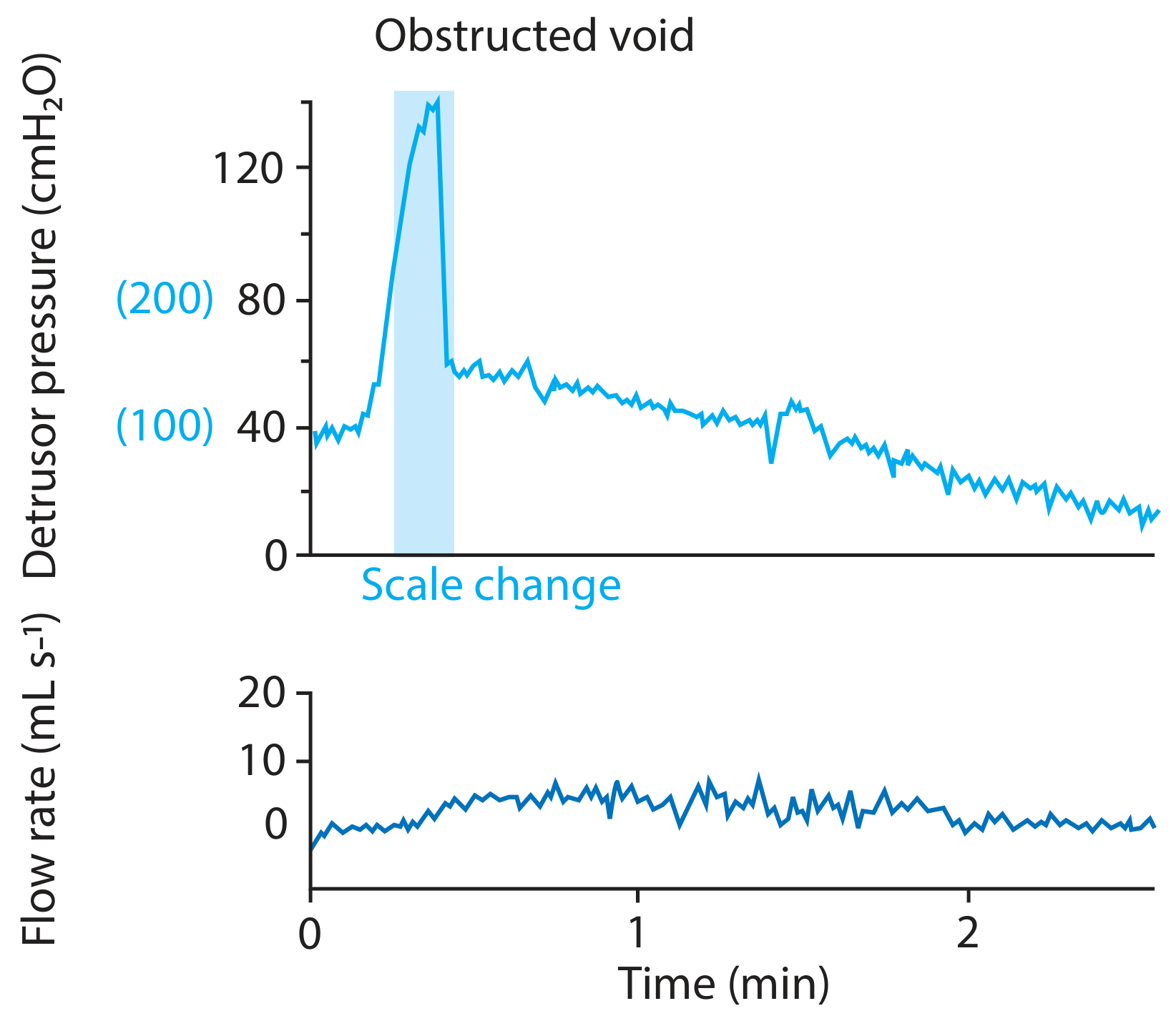
Obstructed void trace
BOO in women
Nomogram criteria differ from men (women can void by pelvic floor relaxation alone). The commonly used thresholds for obstruction in women are:
-
Qmax ≤ 11-15 mL/s plus pdetQmax ≥ 20-25 cmH₂O
-
Videourodynamics (fluoroscopic imaging) adds precision by localizing the site of obstruction
-
Campbell-Walsh-Wein, p. 3381
Pathophysiology - Effects on the Bladder
Immediate / functional changes
- Detrusor hypertrophy - the bladder wall hypertrophies in response to chronic high-pressure voiding; muscle cell size increases massively
- Detrusor overactivity (DO) - obstruction-induced DO with irritative symptoms is attributed to:
- Denervation supersensitivity (increased cholinergic contractile responses)
- Altered contractile proteins (SM-A isoform expression)
- Upregulation of Cx43 (gap-junction protein) leading to enhanced smooth muscle coupling and coordinated myogenic contractions
- Increased NGF (nerve growth factor) in bladder tissue and urine
- Spinal reflex enhancement - a spinal micturition reflex is enhanced in BOO
Long-term effects
-
Bladder decompensation - detrusor contraction becomes progressively less efficient; residual urine accumulates - chronic retention
-
Increased bladder irritability - decreased functional capacity, detrusor overactivity, urgency/frequency
-
High-pressure chronic retention - residual volume >250 mL raises intramural wall tension, causing functional obstruction of the upper tracts and bilateral hydronephrosis, upper tract infection, and renal impairment
-
Bailey and Love's, p. 1545-1546; Campbell-Walsh-Wein, p. 3291
Complications
| Complication | Notes |
|---|---|
| Acute urinary retention | Sometimes the first presentation; painful |
| Chronic retention | Low-pressure (no upper tract damage) or high-pressure (hydronephrosis, renal failure) |
| Overflow incontinence / enuresis | Clue to high-pressure chronic retention |
| Urinary tract infection | From stasis and residual urine |
| Bladder calculi | Stasis promotes stone formation |
| Bladder diverticula | Herniation through areas of muscular weakness |
| Haematuria | May relate to prostatic vascularity; other causes must be excluded |
| Renal failure | From chronic high-pressure back-pressure |
Investigation
- Uroflowmetry - screening; >200 mL voided for reliability
- Post-void residual (PVR) ultrasound - >300 mL warrants further workup; >250 mL suggests chronic retention
- Pressure-flow urodynamics - gold standard for diagnosis
- Videourodynamics - especially valuable in women to localize site of obstruction
- Renal ultrasound - to detect hydronephrosis / upper tract damage
- PSA + prostate size - to guide BPH management
- CT urography + cystoscopy + urine cytology - when haematuria is present
Management
Conservative (watchful waiting)
- Fluid manipulation: avoid fluid binges, limit late-night intake
- Reduce caffeinated and alcoholic drinks
- Appropriate for mild-moderate symptoms
Medical therapy
| Drug class | Agents | Mechanism |
|---|---|---|
| α-blockers | Tamsulosin, alfuzosin, silodosin | Relax smooth muscle of bladder neck and prostate |
| 5α-reductase inhibitors | Finasteride, dutasteride | Reduce prostatic volume (best for large glands) |
| Combination | α-blocker + 5ARI | Superior outcome for glands >35 g |
Note: Medical therapy is not safe in high-pressure chronic retention given the risk of worsening renal failure - these patients need surgical or catheter management.
Strong indications for surgery
- Acute retention in fit men without reversible cause (accounts for ~25% of prostatectomies)
- Chronic retention + renal impairment - residual >200 mL, hydro(ureter)nephrosis, uraemia (~15% of prostatectomies)
- Complications - stone, infection, diverticulum, recurrent haematuria
- Severe symptoms not responding to drugs, Qmax <10 mL/s, residual 100-250 mL (~60% of prostatectomies)
Surgical options
| Procedure | Notes |
|---|---|
| TURP (transurethral resection) | Gold standard for decades |
| HoLEP (holmium laser enucleation) | Preferred for large glands (>100 g), patients on anticoagulation; 7-year data shows equivalent QoL to TURP with fewer reoperations |
| Greenlight laser vaporization | Reduced bleeding and catheter time |
| Open / robotic simple prostatectomy | Large glands |
| PAE (prostate artery embolisation) | Minimally invasive |
| Rezūm (water vapour therapy) | Minimally invasive, preserves sexual function |
| UroLift (prostatic urethral lift) | No thermal energy, day-case procedure |
| Aquablation (water jet) | Robotic-assisted, anatomy-guided |
Patients with very large PVR (>1 L) often benefit more from intermittent self-catheterization or a permanent catheter, because detrusor weakness from chronicity reduces the chance of surgical success.
- Bailey and Love's, p. 1546-1548; Comprehensive Clinical Nephrology, 7th Ed., p. 2502-2504
Recent Evidence (2024-2026)
The AUA 2026 Guideline on LUTS/BPH medical management provides updated recommendations on pharmacotherapy for BOO from BPH (PMID 42095477). A 2025 French systematic review and Clinical Practice Guideline covers surgical and interventional options (PMID 41271373). A 2025 systematic review on primary bladder neck obstruction in women highlights that this remains an underdiagnosed entity (PMID 41102538).
Key teaching point: BOO is confirmed urodynamically - not by symptoms alone. Low flow rate (<10 mL/s) combined with high voiding pressure (>80 cmH₂O) on pressure-flow study is diagnostic. Always assess the upper tracts (renal ultrasound) to rule out high-pressure chronic retention, which changes management fundamentally.
This is a shared conversation. Sign in to Orris to start your own chat.