Describe in detail about the assessment of nutrition status of the community under five-year child. Give, uh, accordingly from the Park textbook. Give the page number also.
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
I now have all the material needed to compose a detailed, well-structured answer. Here is the complete response from Park's Textbook of Preventive and Social Medicine:
Assessment of Nutritional Status of the Community: Under-Five Child
Source: Park's Textbook of Preventive and Social Medicine
Pages: 744-747
Introduction (p. 744)
The nutritional status of an individual is the result of many interrelated factors. It is influenced by the adequacy of food intake - both in quantity and quality - and by the physical health of the individual. The nutritional status of a community is the sum of the nutritional status of all individuals who form that community.
The main objectives of a "comprehensive" nutritional survey are:
- To obtain precise information on the prevalence and geographic distribution of nutritional problems in a given community
- To identify individuals or population groups "at risk" or in greatest need of assistance
- To develop a health care programme that meets the needs defined by that assessment, including evaluation of the effectiveness of such programmes
In nutritional surveys, it is not necessary to examine all persons. A random and representative sample covering all ages, both sexes, and different socio-economic groups is sufficient to draw valid conclusions. All surveys should be planned with expert statistical advice.
Assessment Methods (p. 744)
Proper evaluation demands a many-angled approach, covering all stages in the natural history of nutritional diseases, including the prepathogenic stage:
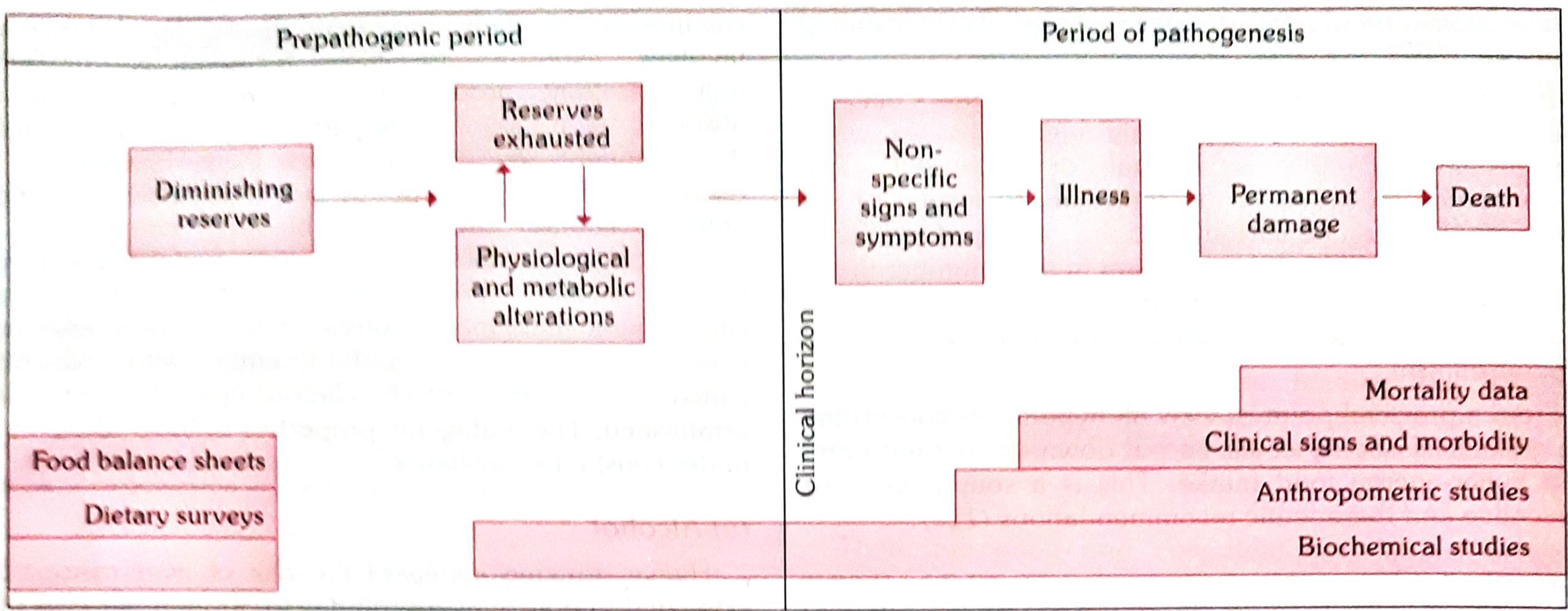
Fig. 5 - Methods of nutritional assessment and their relationship to the natural history of disease (Park's, p. 744)
The assessment methods include:
- Clinical examination
- Anthropometry
- Laboratory and biochemical evaluation
- Functional assessment
- Assessment of dietary intake
- Vital and health statistics
- Ecological studies
These methods are not mutually exclusive; they are complementary.
1. Clinical Examination (p. 744-745)
Clinical examination is the simplest and most practical method of ascertaining nutritional status of a group. There are physical signs - some specific, many non-specific - associated with states of malnutrition.
A WHO Expert Committee classified signs used in nutritional surveys into three categories:
| Category | Examples |
|---|---|
| (a) Not related to nutrition | Alopecia, pyorrhoea, pterygium |
| (b) Needing further investigation | Malar pigmentation, corneal vascularization, geographic tongue |
| (c) Known to be of value | Angular stomatitis, Bitot's spots, calf tenderness, absence of knee/ankle jerks (beri-beri), enlargement of thyroid gland (endemic goitre) |
Drawbacks of clinical examination:
- Malnutrition cannot be quantified on the basis of clinical signs alone
- Many deficiencies are unaccompanied by physical signs
- Lack of specificity and subjective nature of most physical signs
To minimize subjective and objective errors, standard survey forms/schedules covering all areas of the body are used. A specimen nutrition assessment schedule is given as Annexure I at the end of the chapter.
2. Anthropometry (p. 745)
Anthropometric measurements are valuable indicators of nutritional status. Key measurements include:
- Height and weight
- Skinfold thickness
- Arm circumference
In young children (under-five), additional measurements include:
- Head circumference
- Chest circumference
If recorded over time, anthropometric measurements reflect patterns of growth and development and how individuals deviate from the average at various ages in body size, build, and nutritional status. Anthropometric data can be collected by non-medical personnel with sufficient training.
Park's refers further discussion of this to Chapter 11, which covers detailed grading, growth standards, and indices such as:
- Weight-for-age (used when age is known) - reflects both stunting and wasting; used in Gomez classification
- Height-for-age (when age is known) - indicator of stunting (chronic malnutrition)
- Weight-for-height (when age is unknown) - indicator of wasting (acute malnutrition)
- Arm circumference (MUAC - Mid Upper Arm Circumference) - useful when age is unknown; a quick field screening tool
3. Laboratory and Biochemical Assessment (p. 745)
(a) Laboratory Tests
- Haemoglobin estimation - the most important laboratory test in nutrition surveys; useful index of overall nutritional state
- RBC count and haematocrit - also valuable
- Stool examination - for intestinal parasites; history of parasitic infestation, chronic dysentery, diarrhoea provides useful background
- Urine examination - for albumin and sugar
(b) Biochemical Tests
With increasing knowledge of metabolic functions of vitamins and minerals, biochemical tests measure:
- Individual nutrient concentrations in body fluids (e.g., serum retinol, serum iron)
- Abnormal metabolites in urine (e.g., urinary iodine) after a loading dose
- Enzyme activity in which the vitamin is a known co-factor (e.g., in riboflavin deficiency)
Key biochemical tests used in nutrition surveys (Table 33, p. 745):
| Nutrient | Method | Normal Value |
|---|---|---|
| Vitamin A | Serum retinol | 20 mcg/dl |
| Thiamine | TPP stimulation of RBC transketolase | 1.00-1.23 (ratio) |
| Riboflavin | RBC glutathione reductase stimulated by FAD | 1.0-1.2 (ratio) |
| Niacin | Urine N-methyl nicotinamide | (not very reliable) |
| Folate | Serum folate | 6.0 mcg/ml |
| Folate | Red cell folate | 160 mcg/ml |
Limitations: Biochemical tests are time-consuming and expensive; they cannot be applied on a large scale. They are often carried out on a sub-sample of the population. Most reveal only current nutritional status and are useful to quantify mild deficiencies.
4. Functional Assessment (p. 745-746)
Functional indices relate nutrient deficiency to specific body system dysfunction:
| System | Functional Index | Nutrients Involved |
|---|---|---|
| Structural integrity | Erythrocyte fragility, Capillary fragility, Tensile strength | Vit. E, Se; Vit. C; Cu |
| Host defence | Leucocyte chemotaxis, phagocytic capacity, bactericidal capacity, T-cell blastogenesis, Delayed cutaneous hypersensitivity | P/E, Zn; P/E, Fe; P/E, Zn |
| Haemostasis | Prothrombin time | Vit. K |
| Reproduction | Sperm count | Energy, Zn |
| Nerve function | Nerve conduction, Dark adaptation, EEG | P/E, Vit B1, B12; Vit A, Zn |
| Work capacity | Heart rate, Vasopressor response | P/E, Fe; Vit. C |
5. Assessment of Dietary Intake (p. 746)
The value of nutritional assessment is greatly enhanced by supplementing it with assessment of food consumption through dietary surveys.
Methods of diet survey:
- Weighment of raw foods - widely employed in India; survey team visits households and weighs all food to be cooked and eaten, plus wastage. Duration varies from 1-21 days, commonly 7 days ("one dietary cycle")
- Weighment of cooked foods - foods analyzed in the state normally consumed; not easily acceptable
- Oral questionnaire method - used for large populations in short time; inquiries about food eaten during the previous 24 or 48 hours (24-hour dietary recall)
Collected data is translated into:
- Mean intake (grams) of cereals, pulses, vegetables, fruits, milk, meat, fish, and eggs
- Mean intake of nutrients per adult man value or "consumption unit"
A diet survey provides information on dietary intake patterns, specific foods consumed, and estimated nutrient intakes - valuable for planning health education and agriculture/food production policy.
6. Vital Statistics (p. 746)
Analysis of vital statistics (mortality and morbidity data) identifies high-risk groups. Key indices:
- Mortality in age group 1-4 years is particularly related to malnutrition. In developing countries, it may be as much as 20 times that in countries such as Australia, Denmark, or France
- Infant mortality rate
- Second-year mortality rate
- Rate of low birth-weight babies
- Life expectancy
Morbidity data related to:
- Protein energy malnutrition (PEM)
- Anaemia
- Xerophthalmia and other vitamin deficiencies
- Endemic goitre
- Diarrhoea, measles, and parasitic infestations
7. Assessment of Ecological Factors (p. 746)
Malnutrition is the end result of many interacting ecological factors. Ecological assessment comprises:
(a) Food Balance Sheet - Indirect method; food supplies are related to census population to derive per capita food availability. Simpler and cheaper but conceals regional and group differences.
(b) Socio-economic Factors - Family size, occupation, income, education, customs, cultural patterns in relation to feeding practices of children and mothers all influence food consumption.
(c) Health and Educational Services - Primary health care services, feeding programmes, and immunization programmes.
(d) Conditioning Influences - Parasitic, bacterial, and viral infections that precipitate malnutrition.
An "ecological diagnosis" of the various factors is necessary before implementing measures for prevention and control of malnutrition.
Indicators of Nutritional Status - Concise List (Table 36, p. 747)
For Infant and Preschool Child (Under-Five) Nutrition, the recommended indicators are:
| Condition | Indicator |
|---|---|
| Breastfeeding | Proportion being breastfed and on weaning foods, by age in months |
| Child mortality | Mortality rates in children aged 1, 2, 3, and 4 years (emphasis on 2-year-olds) |
| If age is known | Height-for-age; Weight-for-age |
| If age is unknown | Weight-for-height; Arm circumference; Clinical signs and syndromes |
Nutritional Surveillance (p. 747)
Nutritional surveillance is defined as "keeping watch over nutrition, in order to make decisions that will lead to improvement in nutrition in populations." Three distinct objectives:
- To aid long-term planning in health and development
- To provide input for programme management and evaluation
- To give timely warning and intervention to prevent short-term food consumption crises
Summary: Park's textbook (pp. 744-747) outlines seven complementary methods for assessing nutritional status of the community, with specific focus on under-five children using anthropometry (weight-for-age, height-for-age, weight-for-height, MUAC), clinical signs, vital statistics emphasizing 1-4 year mortality rates, and dietary surveys. No single method is sufficient alone - a multi-method approach covering the entire natural history of nutritional disease (from prepathogenic to pathogenic) gives the most complete picture.
- Park's Textbook of Preventive and Social Medicine, pp. 744-747



aa45fd6b-bf77-4867-ba2e-2cb40ee8f3a0.jpeg
+2 more
Give the answers for the questions from this. In similar terms. Similar terms.
analyse_media
analyse_media
analyse_media
The images contain the textbook pages themselves (from Park's), not separate question papers. The user wants me to frame and answer questions based on this textbook content, using the same terminology as the book. I'll now write well-structured Q&A pairs in the exact language/terms of Park's.
Questions & Answers: Assessment of Nutritional Status
(Based on Park's Textbook of Preventive and Social Medicine, pp. 779-781)
Q1. What is the nutritional status of a community?
The nutritional status of a community is the sum of the nutritional status of all individuals who form that community. It is influenced by the adequacy of food intake both in terms of quantity and quality, and also by the physical health of the individual.
Q2. What is the main objective of a "comprehensive" nutritional survey?
The main objective of a comprehensive nutritional survey is to:
- Obtain precise information on the prevalence and geographic distribution of nutritional problems of a given community
- Identify individuals or population groups "at risk" or in greatest need of assistance
In the absence of this information, problems cannot be defined and policies cannot be formulated. The purpose of nutritional assessment is to develop a health care programme that meets the needs defined by that assessment, including evaluation of the effectiveness of such programmes.
Q3. Is it necessary to examine all persons in a nutritional survey? What type of sample is sufficient?
No, it is not necessary to examine all persons in a given community. Examination of a random and representative sample of the population covering:
- All ages
- Both sexes
- Different socio-economic groups
...is sufficient to draw valid conclusions. All surveys should be planned with the aid of expert statistical advice. Decisions must be made in advance regarding: duration of survey, type of survey (cross-sectional or longitudinal), standardization of measurement techniques, and survey instruments.
Q4. What are the assessment methods used to assess nutritional status?
The assessment of nutritional status involves various techniques. Proper evaluation demands a many-angled approach, covering all different stages in the natural history of nutritional diseases, including the prepathogenesis stage (as shown in Fig. 6).
The assessment methods include the following:
- Clinical examination
- Anthropometry
- Biochemical evaluation
- Functional assessment
- Assessment of dietary intake
- Vital and health statistics
- Ecological studies
The different methods used for the appraisal of nutritional status are not mutually exclusive; on the contrary, they are complementary.
Q5. What is the role and importance of clinical examination in nutritional assessment? What are its drawbacks?
Clinical examination is an essential feature of all nutritional surveys since their ultimate objective is to assess levels of health of individuals or population groups in relation to the food they consume. It is the simplest and most practical method of ascertaining the nutritional status of a group of individuals.
A WHO Expert Committee (125) classified signs used in nutritional surveys into three categories:
(a) Not related to nutrition - e.g., alopecia, pyorrhoea, pterygium
(b) That need further investigation - e.g., malar pigmentation, corneal vascularization, geographic tongue
(c) Known to be of value - e.g., angular stomatitis, Bitot's spots, calf tenderness, absence of knee or ankle jerks (beri-beri), enlargement of the thyroid gland (endemic goitre)
Drawbacks of clinical examination:
- (a) Malnutrition cannot be quantified on the basis of clinical signs
- (b) Many deficiencies are unaccompanied by physical signs
- (c) Lack of specificity and subjective nature of most physical signs
To minimize subjective and objective errors, standard survey forms or schedules have been devised covering all areas of the body. A specimen nutrition assessment schedule is given at the end of the chapter (Annexure I).
Q6. What anthropometric measurements are used in nutritional assessment, especially in young children?
Anthropometric measurements such as height, weight, skinfold thickness, and arm circumference are valuable indicators of nutritional status.
In young children, additional measurements such as head and chest circumference are made.
If anthropometric measurements are recorded over a period of time, they reflect the patterns of growth and development, and how individuals deviate from the average at various ages in body size, build, and nutritional status. Anthropometric data can be collected by non-medical personnel, given sufficient training.
Q7. What are the laboratory and biochemical tests used in nutritional assessment?
(a) Laboratory Tests:
- (i) Haemoglobin estimation - the most important laboratory test carried out in nutrition surveys; a useful index of the overall state of nutrition irrespective of its significance in anaemia. An RBC count and haematocrit determination are also valuable.
- (ii) Stools and urine - stools should be examined for intestinal parasites; history of parasitic infestation, chronic dysentery, and diarrhoea provides useful background information. Urine should be examined for albumin and sugar.
(b) Biochemical Tests: These measure:
- Individual nutrient concentration in body fluids (e.g., serum retinol, serum iron)
- Detection of abnormal amounts of metabolites in urine (e.g., urinary iodine), frequently after a loading dose
- Measurement of enzymes in which the vitamin is a known co-factor (e.g., in riboflavin deficiency) - to help establish malnutrition in its preclinical stages
Some biochemical tests used in nutrition surveys (Table 37):
| Nutrient | Method | Normal Value |
|---|---|---|
| Vitamin A | Serum retinol | 20 mcg/dl |
| Thiamine | TPP stimulation of RBC transketolase | 1.00-1.23 (ratio) |
| Riboflavin | RBC glutathione reductase stimulated by FAD | 1.0-1.2 (ratio) |
| Niacin | Urine N-methyl nicotinamide | (not very reliable) |
| Folate | Serum folate / Red cell folate | 6.0 mcg/ml / 160 mcg/ml |
| Vitamin B12 | Serum B12 concentration | 160 mg/L |
| Vitamin C | Leucocyte ascorbic acid | 15 mcg/10⁸ cells |
| Vitamin K | Prothrombin time | 11-16 seconds |
| Protein | Serum albumin / Transferrin / Thyroid-binding pre-albumin | 35 g/L / 20 g/L / 250 mg/L |
Limitations: Biochemical tests are time-consuming and expensive. They cannot be applied on a large scale. They are often carried out on a subsample of the population. Most reveal only current nutritional status and are useful to quantify mild deficiencies.
Q8. What are functional indicators of nutritional status?
Static indices (biochemical indicators) continue to play an important role as they are well established and familiar to practitioners and public health workers. Functional indices of nutritional status are emerging as an important class of diagnostic tools.
Functional indices of nutritional status (Table 38):
| System | Functional Index | Nutrient |
|---|---|---|
| Structural integrity | Erythrocyte fragility | Vit. E, Se |
| Capillary fragility | Vit. C | |
| Tensile strength | Cu | |
| Host defence | Leucocyte chemotaxis | P/E, Zn |
| Leucocyte phagocytic capacity | P/E, Fe | |
| Leucocyte bactericidal capacity | P/E, Fe, Se | |
| T cell blastogenesis | P/E, Zn | |
| Delayed cutaneous hypersensitivity | P/E, Zn | |
| Haemostasis | Prothrombin time | Vit. K |
| Reproduction | Sperm count | Energy, Zn |
| Nerve function | Nerve conduction | P/E, Vit B1, B12 |
| Dark adaptation | Vit. A, Zn | |
| EEG | P/E | |
| Work capacity | Heart rate | P/E, Fe |
| Vasopressor response | Vit. C |
Q9. What are the methods of dietary survey used in nutritional assessment?
A diet survey may be carried out by one of the following methods:
(i) Weighment of raw foods - The method widely employed in India as it is practicable and considered fairly accurate. The survey team visits the households and weighs all food going to be cooked and eaten, as well as that which is wasted or discarded. Duration varies from 1 to 21 days, but commonly 7 days - called "one dietary cycle".
(ii) Weighment of cooked foods - Foods analyzed in the state normally consumed; but this method is not easily acceptable among people.
(iii) Oral questionnaire method - Useful for carrying out a diet survey of a large number of people in a short time. Inquiries are made retrospectively about foods eaten during the previous 24 or 48 hours. If properly carried out, gives reliable results.
The data collected is translated into: (a) mean intake (grams) of cereals, pulses, vegetables, fruits, milk, meat, fish, and eggs, and (b) the mean intake of nutrients per adult man value or "consumption unit". The ICMR publication "Nutritive Value of Indian Foods" is used for this analysis.
Q10. What is the role of vital statistics in nutritional assessment?
An analysis of vital statistics - mortality and morbidity data - will identify groups at high risk and indicate the extent of risk to the community.
- Mortality in the age group 1 to 4 years is particularly related to malnutrition. In developing countries, it may be as much as 20 times that in countries such as Australia, Denmark, or France.
Other rates used:
- Infant mortality rate
- Second-year mortality rate
- Rate of low birth-weight babies
- Life expectancy
Morbidity data (from hospital data or community health surveys) - particularly in relation to protein energy malnutrition, anaemia, xerophthalmia, endemic goitre, diarrhoea, measles, and parasitic infestations - provides additional information contributing to the nutritional status of the community.
Mortality data, however, do not provide a satisfactory picture of the nutritional status of a population alone.
Q11. What is the assessment of ecological factors in nutritional surveys?
Malnutrition is the end result of many interacting ecological factors. In any nutrition survey it is necessary to collect ecological information of the given community to make the nutrition assessment complete. The study of ecological factors comprises:
(a) Food Balance Sheet - Indirect method; food supplies are related to census population to derive levels of food consumption in terms of per capita supply availability. It refers to the country as a whole and conceals regional and group differences. Its great advantage is that it is cheaper and simpler than any method of direct assessment.
(b) Socio-economic Factors - Family size, occupation, income, education, customs, cultural patterns in relation to feeding practices of children and mothers, all influence food consumption patterns.
(c) Health and Educational Services - Primary health care services, feeding and immunization programmes should be taken into consideration.
(d) Conditioning Influences - Parasitic, bacterial, and viral infections which precipitate malnutrition.
It is necessary to make an "ecological diagnosis" of the various factors influencing nutrition in the community before implementing measures for the prevention and control of malnutrition.
Q12. What is nutritional surveillance? What are its objectives?
Nutritional surveillance is defined as "Keeping watch over nutrition, in order to make decisions that will lead to improvement in nutrition in population" (131).
Three distinct objectives have been defined for surveillance systems:
- (a) To aid long-term planning in health and development
- (b) To provide input for programme management and evaluation
- (c) To give timely warning and intervention to prevent short-term food consumption crises
This is a shared conversation. Sign in to Orris to start your own chat.