Dysuria
Reading File
Finding Sources
Searching PubMed
dysuria evaluation management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive overview of Dysuria based on authoritative medical textbooks.
Dysuria
Dysuria is painful, burning, or uncomfortable urination. It is one of the most common presenting complaints in primary care, emergency medicine, and urology, and it nearly always points to inflammation or irritation somewhere in the urogenital tract.
Definition and Character of the Pain
The pain is classically described as a burning sensation and is located:
- Distal urethra in men - present only during voiding and resolves soon after.
- Urethra in women - often described as "internal" dysuria.
- Bladder (suprapubic, at the end of voiding) - suggests bladder inflammation as the primary site.
Pain at the beginning of urination suggests urethral pathology; pain at the end (terminal dysuria) suggests bladder neck or trigone involvement.
- Smith and Tanagho's General Urology, 19th Edition
- Harrison's Principles of Internal Medicine, 22nd Ed.
Differential Diagnosis
Dysuria has a broad differential. The most common causes are:
Infectious
| Category | Causes |
|---|---|
| Urinary Tract Infection (UTI) / Cystitis | E. coli (most common), Klebsiella, Staphylococcus saprophyticus |
| Urethritis (STI-related) | N. gonorrhoeae, C. trachomatis, M. genitalium, U. urealyticum, T. vaginalis, HSV, adenovirus |
| Vaginitis | Candida albicans, Trichomonas vaginalis, bacterial vaginosis |
| Prostatitis | Bacterial (acute or chronic) |
| Pyelonephritis | Upper tract extension of UTI |
Non-infectious
-
Calculi (urinary stones)
-
Meatal stenosis
-
Neoplasm - bladder, prostate, vulvovaginal, penile
-
Interstitial cystitis / urethral syndrome
-
Atrophic vaginitis/urethritis (postmenopausal women)
-
Trauma - foreign body, postcoital, mechanical
-
Chemical/irritant urethritis - soaps, spermicides, hygiene products
-
Medications
-
Somatization
-
Spondyloarthropathy-associated urethritis
-
Textbook of Family Medicine, 9th Ed. (Table 40-3)
Key History Points
- Onset and character - acute vs. gradual; internal ("bladder") vs. external ("skin contact with urine")
- Associated symptoms - frequency, urgency, hematuria, flank pain, fever (point toward UTI/pyelonephritis)
- Vaginal/urethral discharge - strongly suggests STI or vaginitis rather than simple cystitis
- Sexual history - new or multiple partners, condom use, partner symptoms
- Vaginal symptoms - pruritus, odor, discharge (suggest vaginitis as a cause of external dysuria)
- Medications and hygiene products - irritant causes
- Systemic symptoms - fever, chills, rigors suggest upper tract or systemic infection
The distinction between internal dysuria (felt inside the urethra/bladder, typical of cystitis/urethritis) and external dysuria (pain as urine contacts the vulva/perineum, typical of vaginitis/herpetic lesions) is clinically important.
Approach by Patient Group
The flowchart below from Harrison's Principles of Internal Medicine (22nd Ed.) summarizes the clinical decision-making:
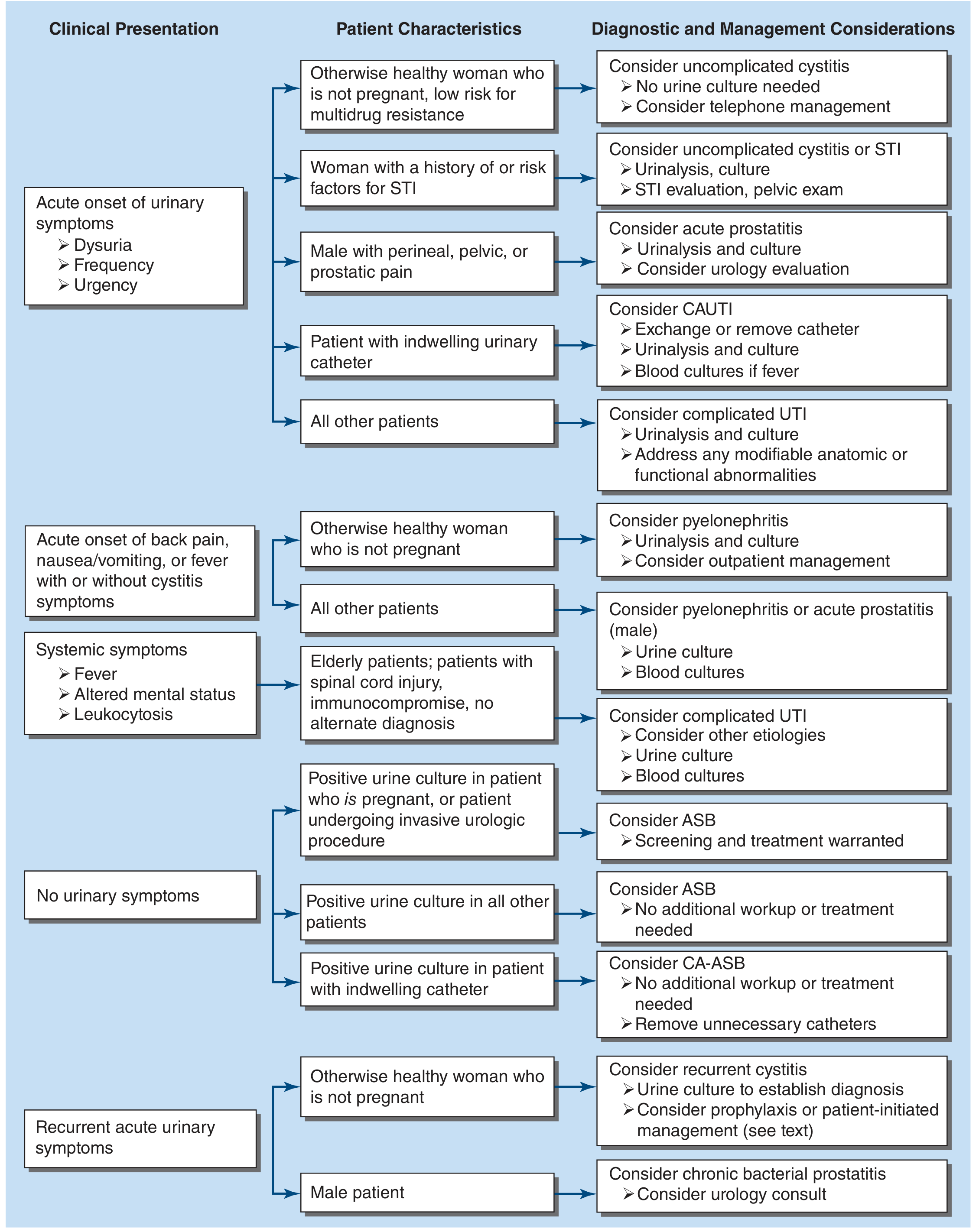
Women
-
Acute dysuria + frequency/urgency, no discharge, no vaginal symptoms - most likely uncomplicated cystitis. Urine culture may not be necessary in healthy, non-pregnant, low-risk women.
-
Dysuria + vaginal discharge, new partner, or STI risk factors - consider urethritis (chlamydia, gonorrhea), cervicitis, or vaginitis. Send urinalysis, urine culture, and STI screen (NAAT for C. trachomatis and N. gonorrhoeae); perform pelvic exam.
-
Dysuria + external burning + pruritus + discharge, no pyuria - suggest vaginitis (Candida, Trichomonas). No urgency/frequency in these cases.
-
Dysuria caused by urethritis - more gradual onset, associated with cervicitis or vulvovaginal herpetic lesions; pyuria present but hematuria rare.
-
Postmenopausal women - atrophic urethritis/vaginitis is common; physical exam shows thinning of vaginal mucosa.
-
Berek & Novak's Gynecology; Harrison's Principles of Internal Medicine 22E
Men
- Dysuria is less common in young men and more frequent with advancing age (e.g., BPH-related).
- Young sexually active man + urethral discharge - urethritis (gonococcal vs. non-gonococcal) is the leading diagnosis.
- Gram stain: >2 neutrophils/HPF confirms urethritis; gram-negative intracellular diplococci = gonorrhea.
- No diplococci = NGU (most likely C. trachomatis or M. genitalium).
- Dysuria without evidence of urethritis - evaluate for prostatitis (digital prostate exam, urine culture) or cystitis.
- Harrison's Principles of Internal Medicine, 22nd Ed.
Special populations
- Indwelling catheter - consider catheter-associated UTI (CAUTI); exchange/remove catheter, send urinalysis and culture.
- Elderly patients / immunocompromised / spinal cord injury - complicated UTI with atypical presentations; obtain urine and blood cultures.
- Pregnant women - negative dipstick does NOT rule out bacteriuria; urine culture required for screening.
Investigations
| Test | Use |
|---|---|
| Urine dipstick | Leukocyte esterase (pyuria surrogate) + nitrites (Enterobacterales only); negative for both argues against UTI but not 100% sensitive |
| Urinalysis (microscopy) | Pyuria in nearly all cystitis; hematuria in ~30%; >10 WBC/HPF traditional threshold but specificity is poor |
| Urine culture | Required for complicated UTI, pyelonephritis, pregnancy, recurrent/treatment-failure cases |
| NAAT (urine or swab) | For C. trachomatis and N. gonorrhoeae when STI suspected |
| Gram stain of urethral discharge | First-line to distinguish gonococcal from non-gonococcal urethritis |
| Vaginal wet mount / KOH prep | For vaginitis workup (Trichomonas, Candida, bacterial vaginosis) |
| Blood cultures | In febrile/systemically unwell patients (pyelonephritis, urosepsis) |
- Harrison's Principles of Internal Medicine, 22nd Ed.
Management Principles
Uncomplicated cystitis (women)
- Nitrofurantoin 100 mg modified-release twice daily x 5 days, or trimethoprim-sulfamethoxazole 160/800 mg twice daily x 3 days (where resistance rates allow), or fosfomycin 3 g single dose.
Urethritis - Gonococcal
- Ceftriaxone IM single dose (per current CDC guidelines; dose has changed to 500 mg or 1 g over time - confirm local guidelines).
Urethritis - Non-gonococcal (NGU)
- Doxycycline 100 mg orally twice daily x 7 days (first-line).
- Azithromycin 1 g single dose (alternative, but rising M. genitalium resistance is a concern).
- Treat current sexual partner(s).
- No test of cure needed if symptoms resolve.
Vaginitis
- Candida - fluconazole 150 mg single oral dose or topical antifungals.
- Trichomonas - metronidazole 500 mg twice daily x 7 days (or 2 g single dose).
- Bacterial vaginosis - metronidazole 500 mg twice daily x 7 days.
Pyelonephritis
-
Outpatient: levofloxacin 750 mg daily x 7 days, or TMP-SMX x 14 days.
-
Inpatient: parenteral ceftriaxone, levofloxacin, or gentamicin.
-
Berek & Novak's Gynecology; Harrison's Principles of Internal Medicine 22E; Textbook of Family Medicine 9E
Important Clinical Pearls
- Dysuria alone does NOT confirm UTI - empiric antibiotics based on this symptom alone leads to unnecessary antibiotic use. Combining it with frequency, urgency, hematuria, and absence of vaginal discharge significantly increases the likelihood of UTI. - Textbook of Family Medicine, 9th Ed.
- A negative dipstick (nitrite AND leukocyte esterase both negative) should prompt alternative diagnoses.
- Vaginal discharge + dysuria - do not treat as simple UTI; evaluate for STI/vaginitis.
- In men with suspected urethritis who lack objective evidence of urethritis, repeated antibiotic courses are not beneficial - consider other etiologies.
- Asymptomatic bacteriuria (ASB) should NOT be treated in most patients; treatment is only warranted in pregnancy and before invasive urologic procedures.
This is a shared conversation. Sign in to Orris to start your own chat.