Pyogenic liver abscess, Amoebic liver abscess .Clinical, course, diagnosis, differential diagnosis of methods of surgical treatment. Complications of parasitic diseases of the liver. with anatomy of liver
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information from multiple authoritative surgical and internal medicine textbooks. Let me compose the full detailed answer.
Liver Anatomy, Pyogenic & Amoebic Liver Abscess, and Parasitic Liver Disease
PART I: SURGICAL ANATOMY OF THE LIVER
Gross Anatomy
The liver is the largest organ in the body, weighing approximately 1500 g. It resides in the right upper abdominal cavity beneath the diaphragm and is protected by the rib cage. It is covered by visceral peritoneum (serosa) with a layer of connective tissue - Glisson's capsule - underneath. At the porta hepatis, the capsule envelops and travels along portal tracts carrying branches of the hepatic artery, portal vein, and bile ducts.
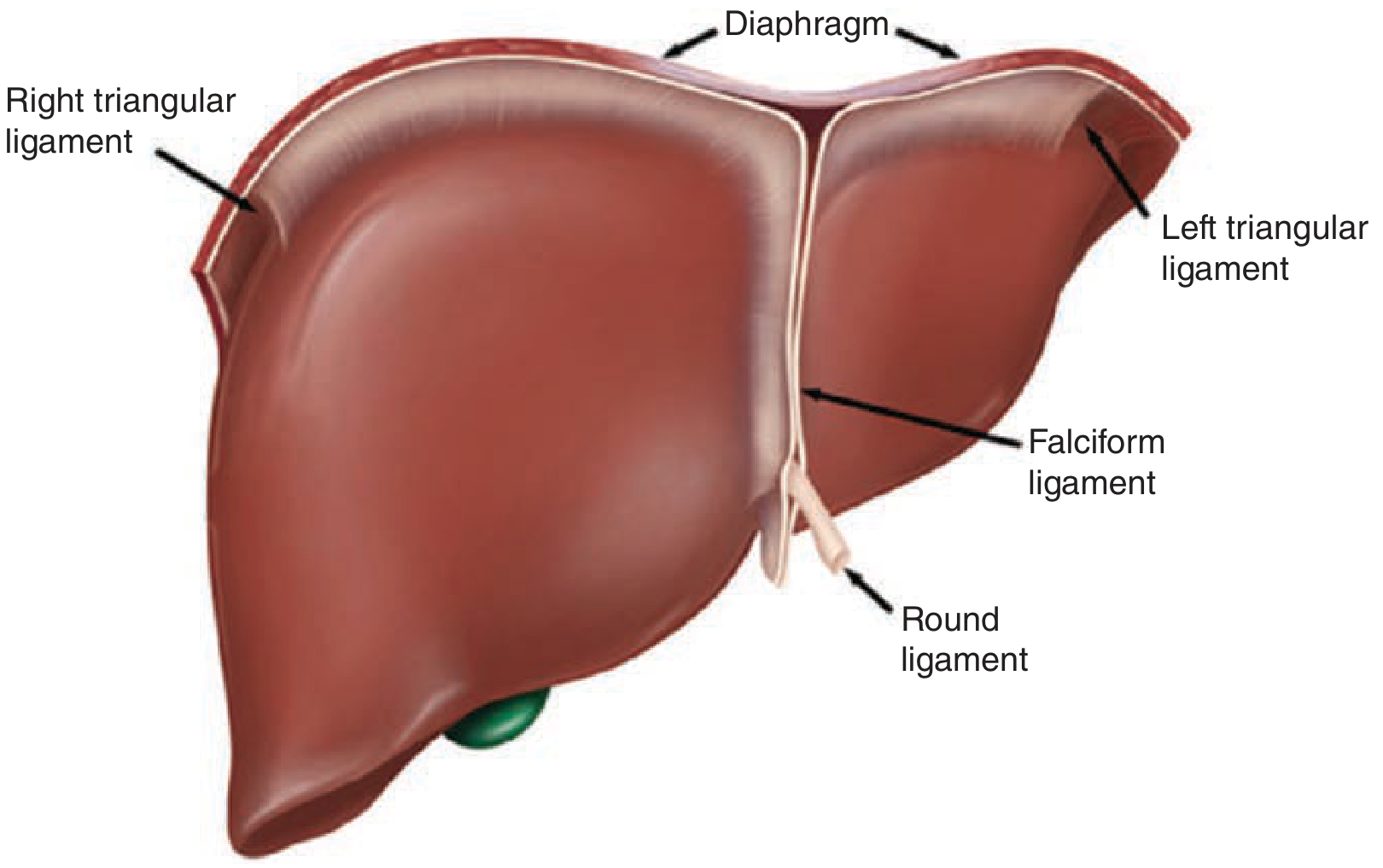
Figure: Hepatic ligaments - right triangular, left triangular, falciform, and round ligament (Schwartz's Principles of Surgery)
Ligaments and Peritoneal Reflections
| Ligament | Origin / Significance |
|---|---|
| Falciform ligament | Remnant of umbilical vein; divides left lateral from left medial segment; anchors liver to anterior abdominal wall |
| Round ligament | Obliterated umbilical vein; enters left liver hilum at the front edge of the falciform ligament |
| Ligamentum venosum | Obliterated ductus venosus (Arantius' ligament); lies between caudate lobe and left lateral segment |
| Right triangular ligament | Fixes right lobe to undersurface of right hemidiaphragm |
| Left triangular ligament | Fixes left lobe to diaphragm; division mobilises the liver |
| Coronary ligaments | Extend from triangular ligaments anteriorly; right coronary also anchors liver to right retroperitoneum |
| Lesser omentum (hepatoduodenal + gastrohepatic) | Contains portal triad in its right free edge; the hepatoduodenal ligament is the porta hepatis |
The foramen of Winslow (epiploic foramen) is posterior and right of the porta hepatis - clamping the hepatoduodenal ligament here = the Pringle manoeuvre for vascular inflow control.
Segmental (Couinaud) Anatomy
The liver is grossly divided by Cantlie's line (gallbladder fossa to IVC) into right lobe (60-70%) and left lobe + caudate lobe. Couinaud (1950s) divided the liver into 8 functional segments, each with its own portal pedicle and hepatic venous drainage, allowing independent resection:
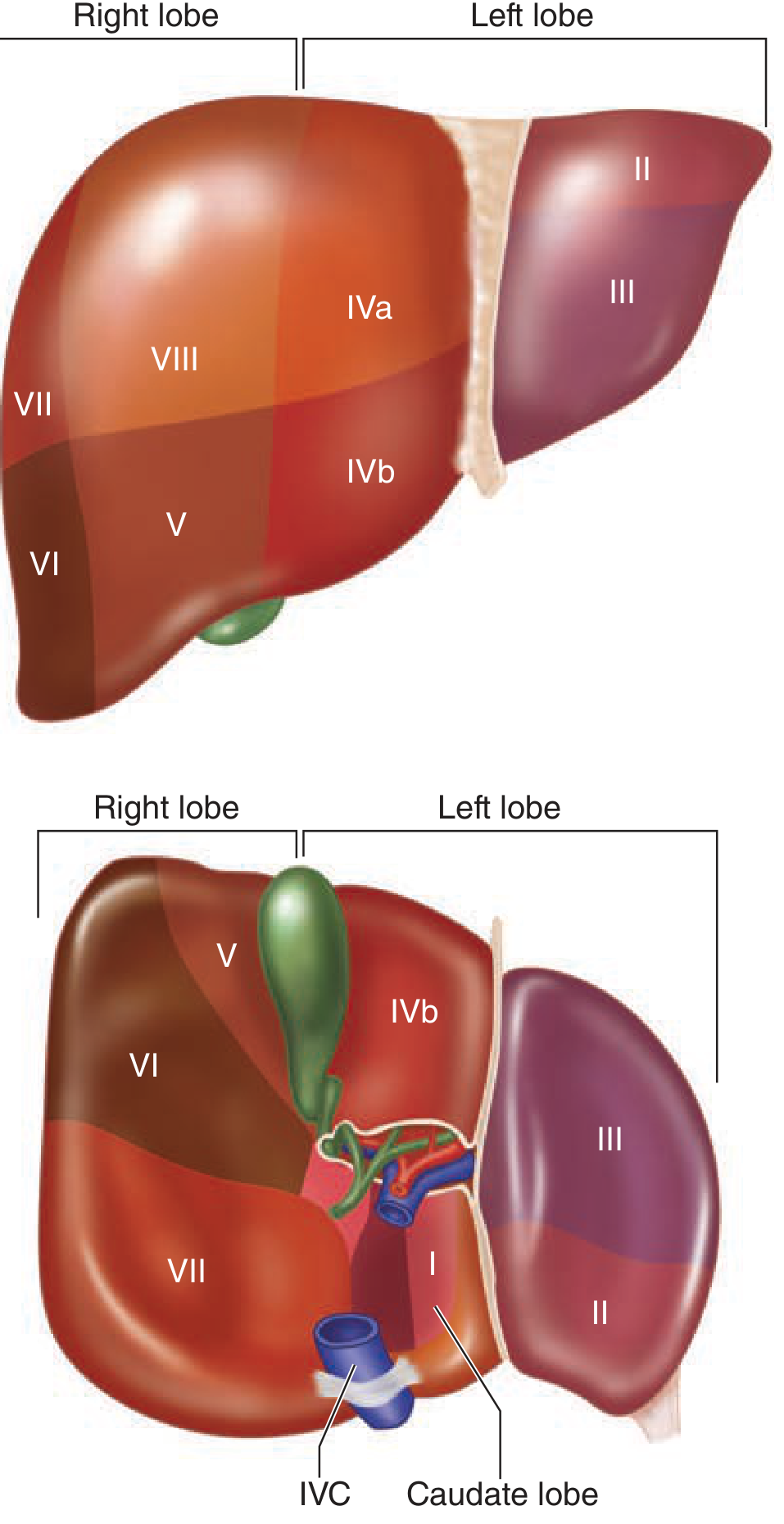
Figure: Couinaud's liver segments I-VIII numbered clockwise. Left lobe = II-IV, right lobe = V-VIII, caudate = I (Schwartz's Principles of Surgery)
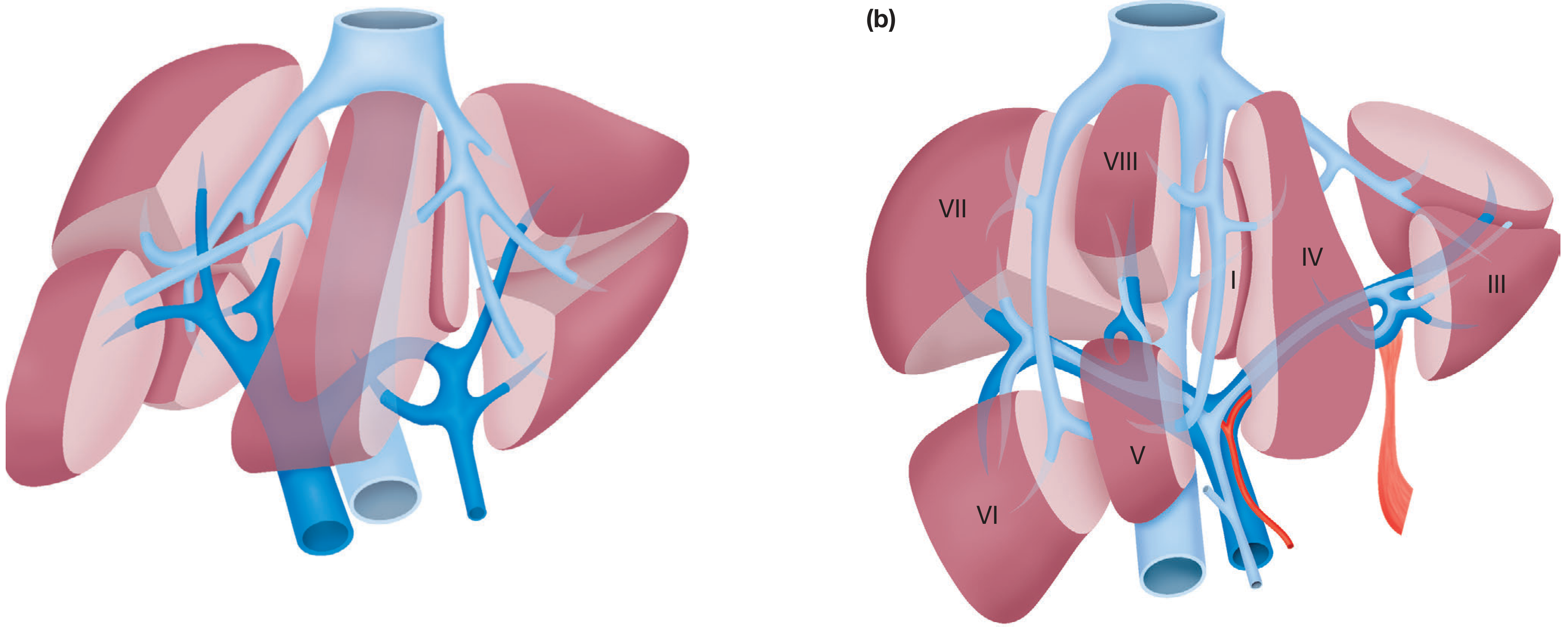
Figure: Functional division of liver segments (Bailey & Love)
- Segment I = Caudate lobe (Spiegel lobe + paracaval + caudate process)
- Segments II-III = Left lateral segment
- Segment IV (IVa cephalad, IVb caudad) = Left medial segment (formerly "quadrate lobe")
- Segments V, VIII = Right anterior sector
- Segments VI, VII = Right posterior sector
Blood Supply
Dual supply: Portal vein (75-80%) + Hepatic artery (20-25%). Both drain into hepatic sinusoids.
Hepatic artery: Arises from the celiac trunk (classic anatomy in ~76%). Common hepatic artery → gastroduodenal artery + hepatic artery proper → right and left hepatic arteries. Variants are common:
- Replaced/accessory right hepatic artery from the SMA (10-15%)
- Replaced/accessory left hepatic artery from left gastric artery (3-10%)
Portal vein: Formed by confluence of splenic vein and superior mesenteric vein posterior to the neck of the pancreas.
Hepatic veins: Three main veins (right, middle, left) drain into the IVC; they define Bismuth's four sectors and the main fissure (containing the middle hepatic vein) separates right and left livers.
PART II: PYOGENIC LIVER ABSCESS (PLA)
Aetiology and Pathophysiology
Pyogenic liver abscess (PLA) occurs at approximately 1/5000 hospital admissions. The routes of infection are:
- Biliary obstruction (most common, ~35%) - from cholelithiasis, malignancy, intrahepatic cholangiopathy, or post-liver transplant biliary stricture - with secondary infection
- Portal pyaemia (~20%) - ascending infection from appendicitis, diverticulitis, Crohn's disease
- Haematogenous spread via hepatic artery - systemic bacteraemia
- Direct spread - from contiguous structures (subphrenic/intra-abdominal abscess)
- Trauma (blunt/penetrating)
- Cryptogenic (~10-15%) - no identifiable source; often monomicrobial Klebsiella pneumoniae; associated with occult colorectal cancer (colonoscopy warranted)
Organisms: Mostly polymicrobial. Of biliary origin: E. coli, Klebsiella, Enterococcus. Of enteric origin: Bacteroides fragilis and other anaerobes. Streptococcus milleri group is notable. Cryptogenic: K. pneumoniae (monomicrobial). Fungal abscesses in immunosuppressed patients carry highest mortality.
Risk factors: Diabetes mellitus, elderly, immunosuppression, biliary instrumentation, liver transplant, PPI use (possibly via loss of gastric acid barrier).
Clinical Features
| Symptom/Sign | Frequency |
|---|---|
| Fever, rigors | ~90% |
| Abdominal pain (RUQ) | ~60% |
| Malaise, anorexia, weight loss | Common |
| Jaundice | Variable |
| Right shoulder tip pain (diaphragmatic irritation) | Present in some |
| Hepatomegaly / tender liver | Frequent |
Laboratory: Leukocytosis (90%), elevated alkaline phosphatase (80%), hyperbilirubinaemia (50%), transaminitis (50%). Blood cultures positive in >50%.
Diagnosis
- Ultrasonography: First-line, less sensitive but widely available. Shows hypoechoic/cystic mass, may reveal loculations.
- CT with IV contrast: Most sensitive. PLA appears hypoattenuating with possible loculations and peripheral rim enhancement (uncommon but specific). Also reveals the underlying aetiology.
- MRI: Used for further characterisation.
- Aspiration: Confirms diagnosis, guides microbiology and culture, and is therapeutic.
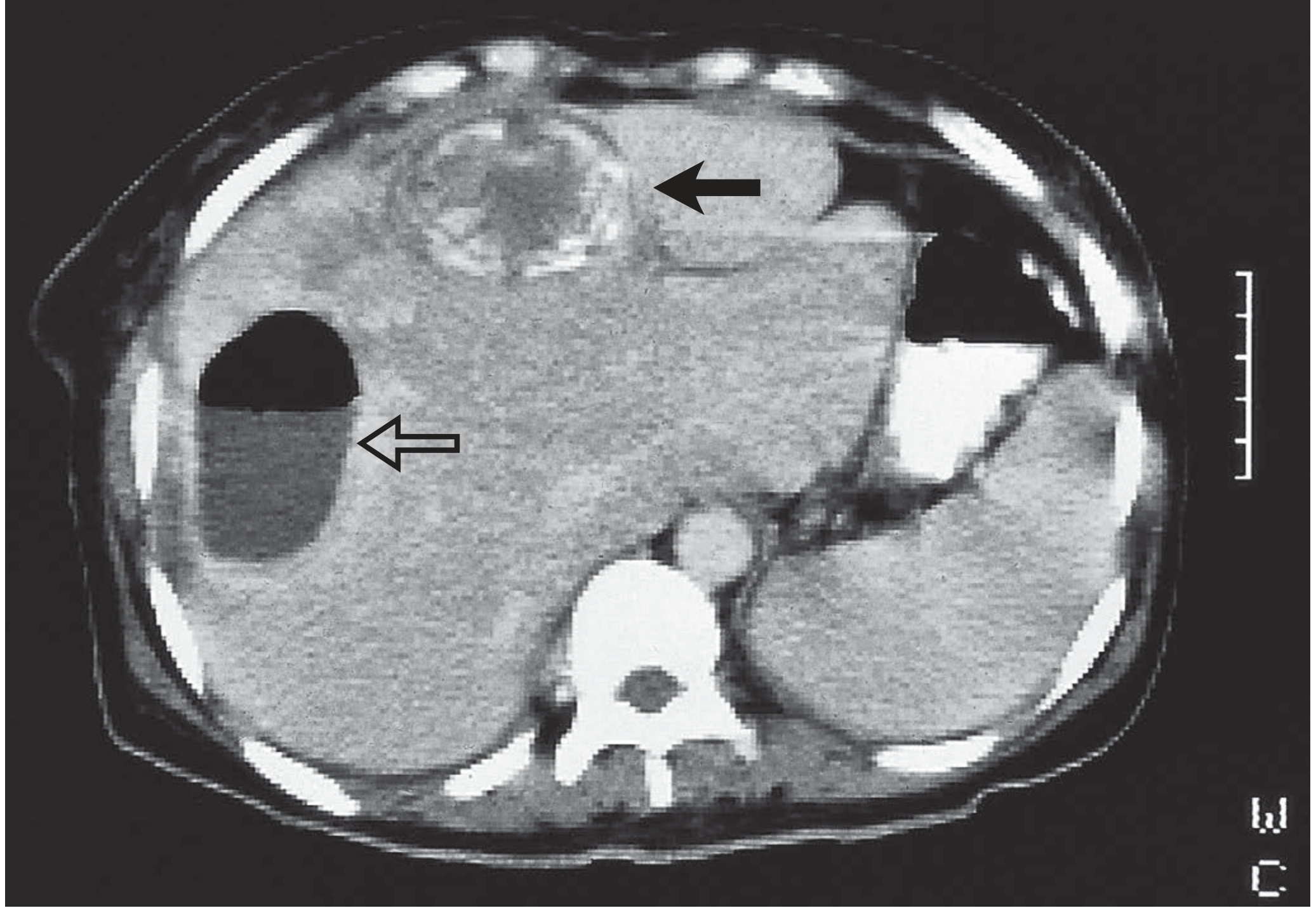
Figure: CT of pyogenic liver abscess with air-fluid level and rim enhancement (Bailey & Love)
Differential Diagnosis
| Condition | Distinguishing features |
|---|---|
| Amoebic liver abscess | Travel history, serology, "anchovy paste" aspirate, solitary right lobe, responds to metronidazole alone |
| Hepatic hydatid cyst | Echinococcus serology, characteristic CT (daughter cysts, calcification), no fever unless infected |
| Simple hepatic cyst | No wall enhancement, no fever, thin-walled |
| Hepatic haemangioma | Enhancement pattern on contrast CT/MRI ("fill-in"), no fever |
| Necrotic hepatocellular carcinoma | AFP elevated, cirrhosis, arterial phase enhancement of viable rim |
| Cholangiocarcinoma | Biliary dilatation, mass, obstruction pattern |
| Non-infected haematoma | History of trauma |
| Subphrenic abscess | Location below diaphragm, often post-operative |
Treatment
Step 1 - Identify and treat the source
Step 2 - Antibiotics
- Empiric until cultures: piperacillin/tazobactam monotherapy, or ceftriaxone + metronidazole
- Biliary/instrumented patients or ESBL risk: carbapenems
- Metronidazole + clindamycin provide excellent anaerobic coverage and abscess penetration; 3rd-generation cephalosporins/aminoglycosides for Gram-negatives
- Duration: guided by clinical response and imaging resolution at 4-6 weeks
Step 3 - Drainage (Surgical Treatment)
| Method | Indication |
|---|---|
| Needle aspiration (image-guided) | Abscess <3 cm (if technically feasible); repeated aspirations may be needed |
| Percutaneous catheter drainage (PCD) | Standard of care for any abscess >5 cm; superior outcomes vs needle aspiration alone; first-line for all PLAs without rupture; multiple catheters for >10 cm |
| Surgical drainage (laparoscopic or open) | Failure of PCD; ruptured abscess; concurrent intra-abdominal source requiring surgery; multiple abscesses not amenable to PCD; localised complex abscesses |
| Hepatic resection | Rare; refractory or recurrent segmental disease; necrotic tumour as source |
Catheters remain until output is low and clear; follow-up imaging at 4-6 weeks.
Recurrent/Refractory abscesses: Occur when initial abscess was large, multiple, or with persistent biliary communication. Re-aspiration or drain insertion required; occasionally laparoscopy (preferred over laparotomy) to identify the source.
Prognosis: Mortality 4-10%. Worse with diabetes, malignancy, cirrhosis, abscess >10 cm, multiple abscesses.
PART III: AMOEBIC LIVER ABSCESS (ALA)
Aetiology and Pathophysiology
ALA is caused by the protozoan Entamoeba histolytica. It is the most common cause of liver abscess worldwide in endemic regions (tropics/subtropics). In the US/Europe, it is seen predominantly in male patients (8:1 male-to-female ratio) with a travel history to endemic areas.
Pathogenesis:
- Ingestion of mature E. histolytica cysts or trophozoites via faecally contaminated food/water
- Colonic amebiasis with mucosal invasion
- Trophozoites seed the liver via the portal system (typically 2-4 months after colonic symptoms)
- Necrotic hepatocytes and trophozoites form the abscess content - classically described as "anchovy paste" - a thick, dark brown proteinaceous fluid
Clinical Features
| Feature | Detail |
|---|---|
| Fever | ~80% |
| RUQ pain | ~60%; often more acute and severe than PLA |
| Diarrhoea / dysentery | May precede by weeks-months (or absent) |
| Male predominance | 8:1 |
| Endemic region travel | Key history |
| Hepatomegaly | Common |
| Jaundice | Less common |
Important differences from PLA: Eosinophilia is NOT typically seen (despite being a parasite). Usually solitary abscess in the right lobe. Younger patients, less comorbidity.
Laboratory: Leukocytosis, elevated ALP, bilirubin, transaminases. Serology: E. histolytica antibody/antigen testing (highly sensitive; antigen testing more specific as 1/3 of patients with prior infection retain antibodies).
Diagnosis
- Imaging: Ultrasound or CT - cannot reliably differentiate ALA from PLA. Typically solitary, right lobe, round lesion.
- Serology: E. histolytica antibody or antigen - key diagnostic test; rules out ALA effectively.
- Aspiration: Yields "anchovy paste" - but trophozoites are rarely found in the aspirate (they are at the abscess wall).
- 72% of ALA patients without intestinal symptoms still have bowel infection with E. histolytica on stool examination.
Differential Diagnosis from PLA
| Feature | PLA | ALA |
|---|---|---|
| Age/sex | Older, either sex | Younger, male (8:1) |
| Travel history | Usually no | Yes (endemic area) |
| Abscess number | Often multiple | Usually solitary |
| Lobe | Either | Right lobe (>80%) |
| Aspirate | Purulent/foul | "Anchovy paste" |
| Serology | Negative | Positive E. histolytica |
| Eosinophilia | No | No |
| Response to metronidazole | No | Yes (dramatic, 90% within 72h) |
| Organisms on culture | Bacteria | Sterile (usually) |
Treatment
1. Antiparasitic (intestinal + liver)
- Metronidazole 500-750 mg TDS x 7-10 days - drug of choice; >90% respond within 72h with decrease in pain and fever
- Longer-acting nitroimidazoles (tinidazole, ornidazole) - effective as single/shorter-dose therapy
- MUST follow with a luminal agent to eradicate intestinal cysts and prevent recurrence:
- Paromomycin 10 mg/kg TDS x 7 days (preferred), OR
- Diiodohydroxyquin 650 mg TDS x 20 days
- No evidence that combined dual antiparasitic therapy is superior to single-agent
2. Drainage
ALA does NOT routinely require drainage - a major distinction from PLA.
Indications for aspiration/drainage in ALA (Harrison's):
- Need to rule out a pyogenic abscess (especially with multiple lesions)
- No clinical response to metronidazole in 3-5 days
- Threat of imminent rupture (very large abscess)
- Prevention of left-lobe abscess rupture into the pericardium (life-threatening complication)
Surgical intervention is reserved for:
- Bowel perforation
- Rupture into the pericardium
- Failure of all other measures
Abscess resolution may take several months on imaging - this does not indicate treatment failure and should not drive antibiotic cessation decisions.
Prognosis: Mortality <1% with early diagnosis and treatment. Recurrence is rare.
PART IV: COMPLICATIONS OF PARASITIC LIVER DISEASES
Amoebic Liver Abscess - Complications
| Complication | Details |
|---|---|
| Rupture into pleural cavity | Most common extraperitoneal complication; right-sided pleuropulmonary amoebiasis |
| Rupture into peritoneum | Amoebic peritonitis - surgical emergency |
| Rupture into pericardium | Life-threatening; occurs with left lobe abscesses; requires emergency drainage |
| Rupture into adjacent viscera (bowel, stomach) | Rare fistula formation |
| Secondary bacterial infection | Converts ALA to pyogenic abscess |
| Hepatobronchial fistula | "Chocolate sauce" sputum - expectoration of abscess contents |
| IVC obstruction | Rare, from large abscesses |
| Pleuritis, right-sided effusion | From reactive inflammation |
Hydatid Disease (Echinococcosis) - Complications
Caused by larval stages of Echinococcus granulosus (cystic) or E. multilocularis (alveolar). Liver is affected in ~70% of cases.
| Complication | Details |
|---|---|
| Secondary infection / pyogenic abscess | Cyst becomes infected |
| Biliary communication/leak | Intrabiliary rupture - jaundice, cholangitis |
| Rupture into peritoneum | Anaphylaxis, peritoneal seeding, daughter cysts |
| Rupture into thorax | Bronchial fistula, lung cysts |
| Obstructive jaundice | From compression of bile ducts |
| Cholangiocarcinoma | Long-term complication of biliary involvement |
| Anaphylaxis | On rupture (spontaneous or surgical) |
Surgical Treatment of Hydatid Disease
When medical management (albendazole) fails:
- Liver resection or local excision
- Deroofing with evacuation of cyst contents
- Pre/peri-operative albendazole + praziquantel to prevent seeding
- Peritoneal cavity packed with 20% hypertonic saline-soaked packs; 20% hypertonic saline instilled into cyst before opening (to kill scolices)
- Biliary communication actively sought and sutured
- Omentoplasty (pedicled omentum) to fill the space - reduces bile leak and infection risk
- Calcified cysts may be dead; if doubt, follow by ultrasound (active cysts gradually enlarge)
Other Parasitic Complications Affecting the Liver
| Parasite | Complication |
|---|---|
| Clonorchis sinensis / Opisthorchis (liver flukes) | Biliary obstruction, recurrent cholangitis, predisposes to cholangiocarcinoma |
| Ascaris lumbricoides | Biliary obstruction (worms in bile duct), cholangitis, liver abscess |
| Schistosoma spp. | Periportal fibrosis, portal hypertension, splenomegaly |
| Amoebiasis | See above |
| Echinococcus | See above |
Key principle (Bailey & Love summary): Parasitic infections of the liver cause abscess AND biliary tract damage; biliary involvement predisposes to cholangiocarcinoma; parasitic infections mimic pyogenic abscesses; and obstructive jaundice can result from calcified flukes or biliary tract involvement.
PART V: COMPARISON TABLE - PLA vs ALA
| Feature | Pyogenic (PLA) | Amoebic (ALA) |
|---|---|---|
| Cause | Bacteria (polymicrobial) | E. histolytica |
| Geography | Worldwide | Tropics/endemic areas |
| Age/Sex | Older, any sex | Younger, male (8:1) |
| Number | Multiple or single | Usually solitary |
| Location | Any lobe | Right lobe (>80%) |
| Aspirate | Pus, foul smelling | "Anchovy paste" (brown) |
| Organisms in aspirate | Bacteria on culture | Sterile (trophozoites at wall) |
| Serology | Negative | E. histolytica positive |
| Eosinophilia | No | No |
| Treatment | Antibiotics + drainage (PCD) | Metronidazole + luminal agent |
| Drainage required? | Yes (standard) | Only if no response or rupture risk |
| Mortality | 4-10% | <1% |
| Recurrence | 12-38% | Rare |
Sources: Bailey and Love's Short Practice of Surgery 28th Edition - Current Surgical Therapy 14e - Schwartz's Principles of Surgery 11th Edition - Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.