Important subtopics in the special senses chapter of indukhurana textbook of physiology
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
Indu Khurana textbook physiology special senses chapter important topics subtopics
Finding Sources
Searching the Web
Indu Khurana Essentials Medical Physiology special senses chapter topics eye ear olfaction gustation table of contents
Reading File
Reading Web Page
https://www.scribd.com/document/689040903/70791658786
Now I have enough information to provide a thorough and well-organized answer. The Indu Khurana "Essentials of Medical Physiology" is not in the library database, but based on my knowledge of the book's content, the web search results, and cross-referencing with the available physiology textbooks, I can now give a comprehensive answer about the important subtopics in the Special Senses chapter.
Here are the important subtopics in the Special Senses chapter of Indu Khurana's Essentials of Medical Physiology (Section XI, pages 637-668):
Special Senses - Indu Khurana: Important Subtopics
Chapter 1: Eye and Vision
Anatomy & Optics
- Structure of the eyeball (coats, chambers, lens, aqueous humor)
- Refractive media and refraction of light
- Accommodation - mechanism and components (lens, ciliary muscle, pupil)
- Errors of refraction: myopia, hypermetropia, astigmatism, presbyopia - and their correction
Intraocular Pressure (IOP)
- Formation and drainage of aqueous humor
- Role of trabecular meshwork and canal of Schlemm
- Glaucoma (applied)
Retina and Photoreception
- Structure of the retina: rods and cones, their distribution (fovea vs periphery)
- Photochemistry of vision:
- Rhodopsin (visual purple) and the phototransduction cascade in rods
- Iodopsin in cones
- Vitamin A and visual cycle
- Light and dark adaptation
- Duplicity theory of vision
Color Vision
- Trichromatic theory (Young-Helmholtz)
- Three types of cones (R, G, B pigments)
- Color blindness: types (deuteranopia, protanopia, tritanopia), inheritance
Visual Pathway
- Retina → optic nerve → optic chiasma → lateral geniculate body → visual cortex (area 17)
- Visual field defects according to level of lesion (hemianopia, quadrantanopia, scotoma)
Pupillary Reflexes
- Light reflex: direct and consensual - pathway in detail
- Accommodation reflex (near reflex triad)
- Argyll Robertson pupil (pathognomonic of neurosyphilis)
- Horner's syndrome
Eye Movements
- Types: saccadic, smooth pursuit, vergence
- Conjugate gaze - controlling nuclei
- Nystagmus: types and significance
Chapter 2: Ear - Hearing and Equilibrium
Anatomy Review
- Outer, middle, and inner ear - brief structural overview
Physiology of Hearing
- Sound - frequency, intensity, decibel scale
- Transmission of sound: outer ear → tympanic membrane → ossicles (malleus, incus, stapes) → oval window
- Impedance matching by the middle ear (transformer action, lever ratio, area ratio)
- Attenuation reflex (stapedius and tensor tympani muscles)
- Eustachian tube: role in pressure equalization
Inner Ear - Cochlea
- Structure of cochlea: scala vestibuli, scala tympani, scala media (cochlear duct), organ of Corti
- Basilar membrane and traveling wave theory (Bekesy's place principle)
- Hair cells as mechanoreceptors - transduction mechanism (stereocilia deflection, K+ influx)
- Frequency coding: tonotopic organization of basilar membrane
Auditory Pathway
- Organ of Corti → cochlear nerve (CN VIII) → cochlear nuclei → superior olivary complex → inferior colliculus → medial geniculate body → auditory cortex (area 41, 42)
- Bilateral representation - clinical importance
Applied Audiology
- Conductive vs sensorineural deafness - distinction
- Rinne's test, Weber's test
- Audiogram interpretation (basics)
Vestibular System (Equilibrium)
- Otolith organs (utricle and saccule): detect linear acceleration and gravity (static equilibrium)
- Semicircular canals: detect angular/rotational acceleration (dynamic equilibrium)
- Cupula and endolymph movement
- Vestibular pathway: vestibular nuclei → cerebellum, thalamus, spinal cord
- Vestibulo-ocular reflex (VOR)
- Motion sickness: mechanism
- Caloric test
Chapter 3: Chemical Senses - Taste (Gustation)
- Taste buds: location (fungiform, circumvallate, foliate papillae), structure (taste receptor cells, microvilli/taste pores)
- Five primary tastes: sour, salty, sweet, bitter, umami; mechanism of each
- Taste transduction mechanisms (ion channel-based for salty/sour; G-protein/GPCR-based for sweet/bitter/umami)
- Taste pathway: CN VII (anterior 2/3 tongue), CN IX (posterior 1/3), CN X (epiglottis) → nucleus tractus solitarius → thalamus → gustatory cortex
- Applied: ageusia, hypogeusia
Chapter 4: Chemical Senses - Smell (Olfaction)
- Olfactory epithelium: location (superior nasal conchae), cell types (olfactory receptor neurons, supporting cells, basal cells)
- Olfactory receptor neurons - bipolar cells; ~400 types of olfactory receptors (G-protein coupled)
- Olfactory transduction: odorant → receptor protein → Gs → adenylyl cyclase → cAMP → cation channel opening
- Olfactory pathway (unique - only sense that bypasses the thalamus):
- Olfactory nerve (CN I) → olfactory bulb → olfactory tract → primary olfactory cortex (prepyriform area, amygdala)
- Connections to limbic system - basis of emotional/memory responses to smell
- Olfactory adaptation
- Applied: anosmia (causes - head injury, COVID-19 relevance), parosmia
High-Yield Exam Topics (Most Frequently Asked from This Chapter)
| Topic | Why Important |
|---|---|
| Rhodopsin-visual cycle | Common long question |
| Visual field defects | High-yield, map-based |
| Accommodation reflex vs Light reflex | Frequent MCQ and SAQ |
| Argyll Robertson pupil | Classic applied/clinical |
| Impedance matching in middle ear | Frequently asked mechanism |
| Place principle (Bekesy) | Core hearing theory |
| Conductive vs sensorineural deafness | Clinical application |
| Semicircular canals vs otolith organs | Vestibular physiology comparison |
| Taste pathway cranial nerves | MCQ favorite |
| Olfactory pathway bypassing thalamus | Unique feature, often MCQ |
Note: The Indu Khurana textbook is not currently in the digital library, so this outline is drawn from the known structure of Essentials of Medical Physiology (Elsevier India), cross-referenced with standard physiology textbook coverage (Guyton & Hall, Ganong). The chapter spans approximately pages 637-668 in the 2008 edition. Later editions (3rd/4th) follow the same major chapter divisions but include expanded clinical correlations and added recent concepts in phototransduction and olfactory receptor biology.
Explain the visual pathway with a neat labelled diagram. Add lesions at different levels and visual field defects in detail for university paper
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have all the content needed. Let me compile the comprehensive university-level answer.
Visual Pathway - Complete University Answer
Overview
The visual pathway is the neural route through which visual information travels from the retina to the primary visual cortex in the occipital lobe.
DIAGRAM 1: Visual Pathway with Lesion Sites and Field Defects
(From Ganong's Review of Medical Physiology, 26th Edition)
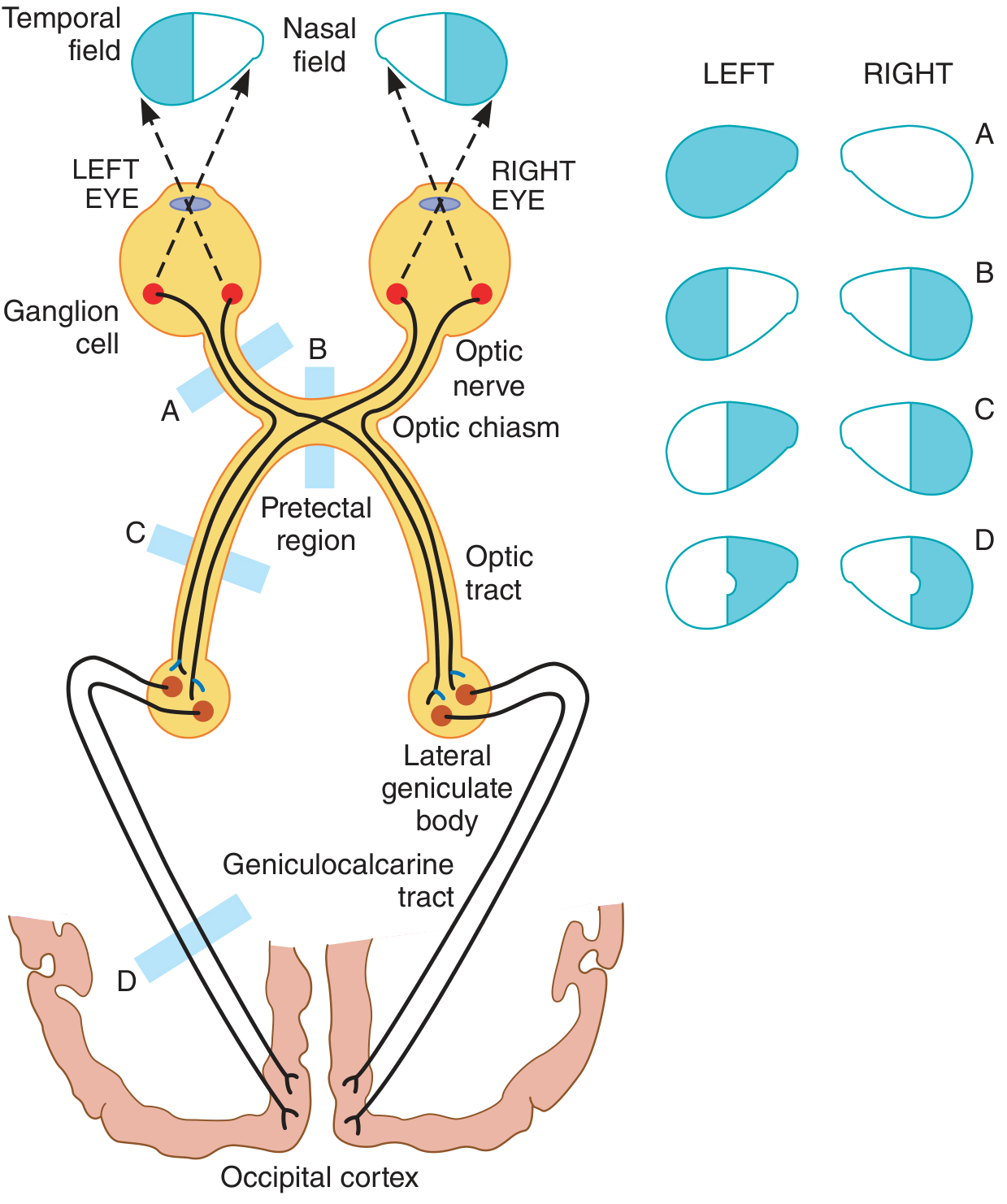
Key: A = optic nerve lesion; B = optic chiasm lesion; C = optic tract lesion; D = occipital cortex lesion
DIAGRAM 2: Detailed Lesion Map - 8 Sites with Field Defects
(From Goldman-Cecil Medicine, International Edition)
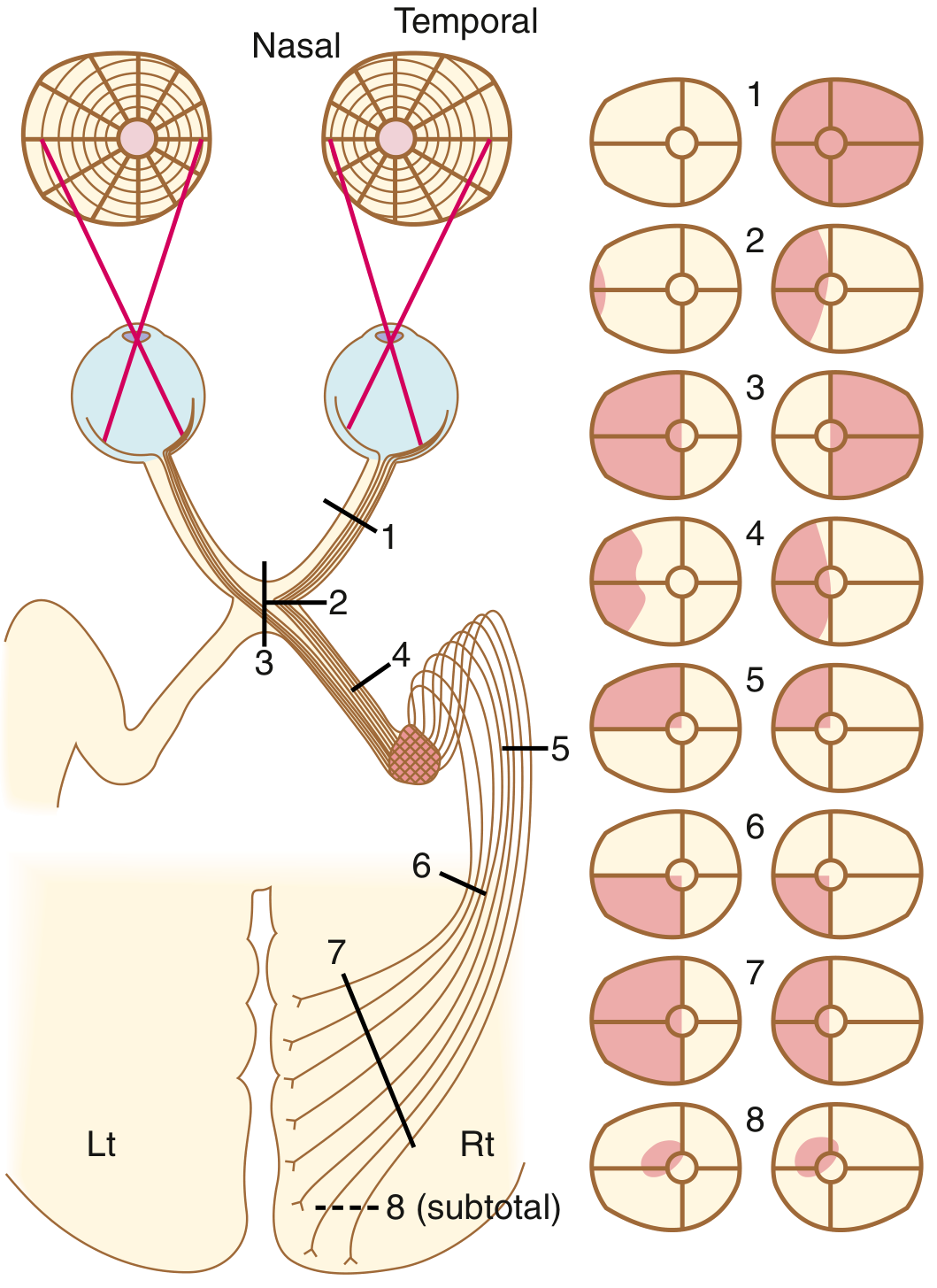
DIAGRAM 3: Visual Field Representation Along the Pathway
(From Gray's Anatomy for Students)
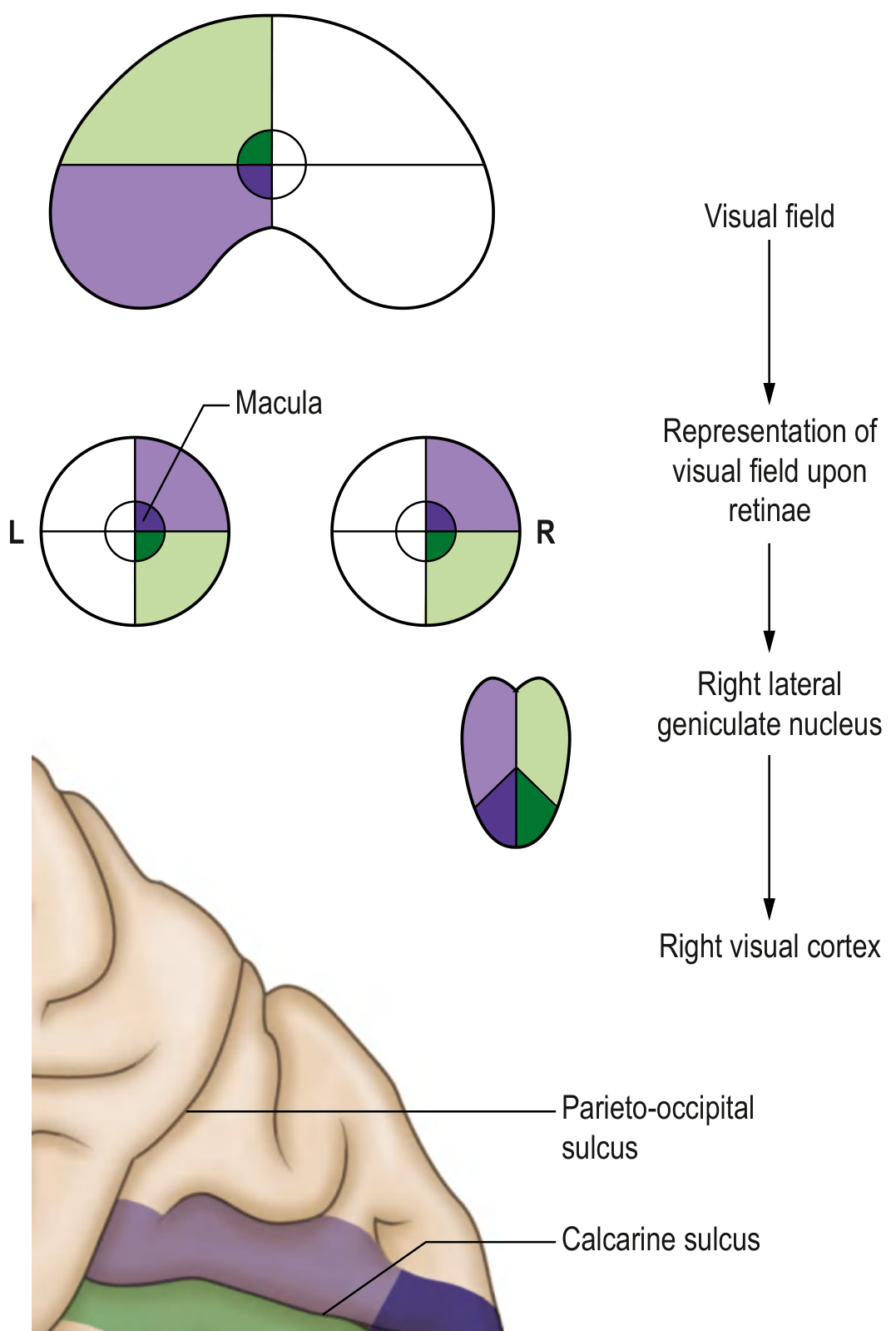
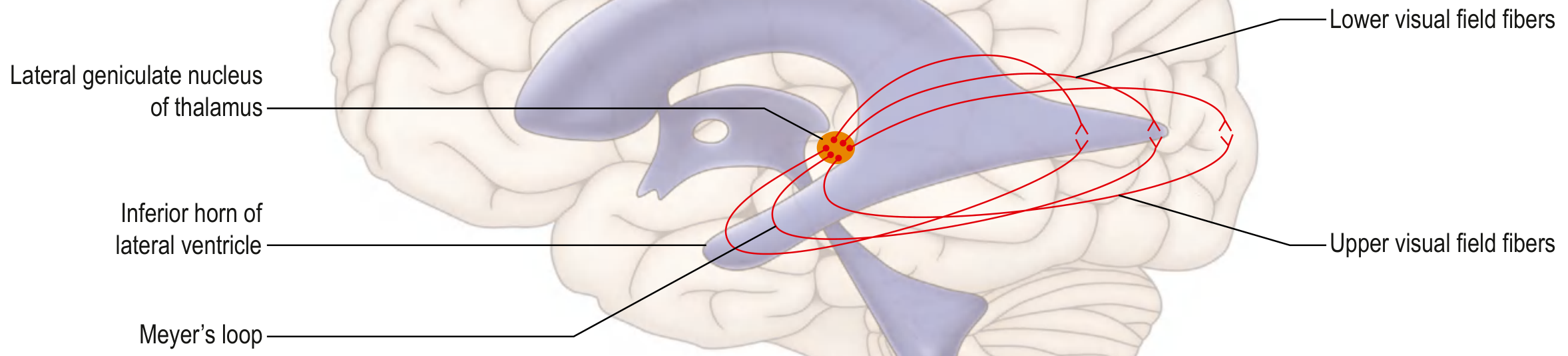
DIAGRAM 4: Optic Radiations (Meyer's Loop)
(From Gray's Anatomy for Students)
I. COMPONENTS OF THE VISUAL PATHWAY
The visual pathway consists of the following sequential relay stations:
Retinal photoreceptors (rods & cones)
↓
Bipolar cells
↓
Retinal ganglion cells
↓ (axons form optic nerve)
Optic nerve (CN II)
↓
Optic chiasm
↓
Optic tract
↓
Lateral Geniculate Nucleus (LGN) of thalamus
↓ (optic radiation / geniculocalcarine tract)
Primary Visual Cortex (Area 17, calcarine fissure, occipital lobe)
II. DETAILED RELAY-BY-RELAY DESCRIPTION
1. Retina
- Contains rods (peripheral; dim light; black/white) and cones (fovea/macula; daylight; color)
- The image on the retina is inverted and reversed: the left visual field falls on the right (nasal) half of the left retina and the right (temporal) half of the right retina
- Ganglion cell axons converge at the optic disc (blind spot - no photoreceptors)
2. Optic Nerve (CN II)
- Formed by ~1.2 million axons of retinal ganglion cells
- Covered by cranial meninges; myelinated by oligodendrocytes (component of CNS, not PNS)
- Runs from the eyeball through the optic canal into the cranial cavity
- Carries all fibers from one eye - both nasal and temporal retinal halves
3. Optic Chiasm
- Located anterior to the infundibular stalk (pituitary stalk), above the pituitary gland
- Key crossing point - partial decussation occurs here:
- Fibers from the nasal (medial) hemiretina of each eye cross to the contralateral optic tract
- Fibers from the temporal (lateral) hemiretina of each eye remain ipsilateral
- Result: each optic tract beyond the chiasm carries fibers representing the contralateral visual field (from both eyes)
- The macular fibers are located posteriorly in the chiasm
4. Optic Tract
- Runs around the midbrain from the chiasm to the lateral geniculate nucleus
- Each optic tract contains:
- Temporal fibers from the ipsilateral eye (representing ipsilateral visual field)
- Nasal fibers from the contralateral eye (representing the same - ipsilateral - visual field)
- A small proportion (~10%) of fibers leave the optic tract before the LGN to reach:
- Pretectal area (superior colliculus) - mediates the pupillary light reflex
- Superior colliculus - controls eye movements and reflexes
5. Lateral Geniculate Nucleus (LGN) of Thalamus
- Located in the posterior thalamus
- Has 6 well-defined layers:
- Layers 1 & 2 = Magnocellular (large cells; M-pathway; movement, depth, coarse form)
- Layers 3-6 = Parvocellular (small cells; P-pathway; color, fine detail, texture)
- Layers 1, 4, 6 = input from contralateral eye
- Layers 2, 3, 5 = input from ipsilateral eye
- Point-for-point (retinotopic) representation of the retina
- Only ~10-20% of LGN input comes from the retina; rest comes from feedback from visual cortex and brainstem
6. Optic Radiation (Geniculocalcarine Tract)
Axons from LGN fan out as the optic radiation (also called geniculocalcarine tract):
| Division | Course | Visual field represented |
|---|---|---|
| Superior fibers (parietal lobe - straight back) | Directly to superior lip of calcarine fissure | Lower contralateral visual field |
| Inferior fibers - Meyer's loop | Loop forward into temporal lobe around inferior horn of lateral ventricle, then back | Upper contralateral visual field |
- Meyer's loop is clinically very important - temporal lobe lesions affect it selectively
7. Primary Visual Cortex (V1, Area 17, Striate Cortex)
- Located on both lips of the calcarine (calcarine) fissure in the medial occipital lobe
- Macular (central) vision is represented posteriorly (large area - macular sparing)
- Peripheral vision is represented anteriorly (small area)
- Upper visual field → inferior lip of calcarine fissure
- Lower visual field → superior lip of calcarine fissure
- From V1, signals go to V2 (area 18), V3, V4 (color), V5/MT (motion), and higher association areas
III. LESIONS AND VISUAL FIELD DEFECTS
Understanding the Terminology First
| Term | Definition |
|---|---|
| Scotoma | Localized area of lost or depressed vision within the visual field |
| Hemianopia | Loss of half the visual field |
| Quadrantanopia | Loss of a quarter of the visual field |
| Homonymous | Same side of visual field in both eyes (right field of both eyes, or left field of both eyes) |
| Heteronymous / Bitemporal | Opposite sides of the visual field in each eye |
| Congruous | Identical (mirror image) defect in both eyes - suggests posterior (postgeniculate) lesion |
| Incongruous | Defect differs in shape/extent between the two eyes - suggests anterior (pregeniculate) lesion |
| Macular sparing | Central (macular) vision preserved despite hemianopia - typical of occipital lobe lesions |
Lesion 1 - Optic Nerve (one eye only)
Site: Anywhere along one optic nerve (CN II), before the chiasm
Defect: Complete monocular blindness (amaurosis) in the ipsilateral eye
Visual field: Total loss of vision in the affected eye; other eye completely normal
Clinical causes: Optic neuritis (MS), central retinal artery occlusion, trauma, optic nerve glioma
Special feature: Afferent pupillary defect (APD / Marcus Gunn pupil) on the affected side - direct light reflex absent, but consensual reflex present
Lesion 2 - Lateral Optic Chiasm
Site: Lateral edge of the chiasm (compressing temporal fibers that do NOT cross)
Defect: Ipsilateral monocular nasal hemianopia (loss of nasal field of one eye)
Clinical causes: Internal carotid artery aneurysm, trauma
Note: Rare, often asymmetric and incongruous
Lesion 3 - Central Optic Chiasm (MOST CLASSIC)
Site: Central chiasm - destroys decussating nasal fibers from both eyes
Defect: Bitemporal hemianopia (loss of both temporal visual fields) - heteronymous
Visual field: Both temporal (outer) halves of the visual field are lost; central and nasal fields are spared
Clinical causes:
- Pituitary adenoma (most common) - expands superiorly from sella turcica
- Craniopharyngioma
- Meningioma of tuberculum sellae
- Suprasellar aneurysm
Special note: Macular fibers are in the posterior chiasm, so early tumors produce superior bitemporal defects first (superior quadrant loss before full hemianopia)
Lesion 4 - Optic Tract
Site: One optic tract (between chiasm and LGN)
Defect: Contralateral incongruous homonymous hemianopia
Visual field: Right optic tract lesion → loss of left visual field in both eyes
Why incongruous? Because corresponding retinal fibers from both eyes have not yet completely interdigitated; they occupy separate positions in the tract
Clinical causes: Pituitary tumor extending laterally, temporal lobe herniation, MS
Special note: Pupillary light reflex may be impaired (Wernicke's hemianopic pupil) because pupillary fibers run in the optic tract
Lesion 5 - Meyer's Loop (Temporal Lobe Optic Radiation)
Site: Inferior fibers of the optic radiation looping through the temporal lobe
Defect: Contralateral congruous homonymous superior quadrantanopia ("pie in the sky")
Visual field: Contralateral upper quadrant lost in both eyes
Clinical causes:
- Temporal lobectomy (surgery for epilepsy)
- Temporal lobe tumors
- MCA infarct (inferior division)
Memory aid: "Temporal lesion = Top field lost" (Meyer's loop = upper field fibers)
Lesion 6 - Parietal Lobe Optic Radiation (Superior fibers)
Site: Superior fibers of the optic radiation in the parietal lobe
Defect: Contralateral congruous homonymous inferior quadrantanopia ("pie on the floor")
Visual field: Contralateral lower quadrant lost in both eyes
Clinical causes: Parietal lobe tumors, MCA infarct (superior division)
Associated features: Hemisensory loss, parietal lobe signs (dressing apraxia, neglect)
Lesion 7 - Complete Optic Radiation / Parieto-Occipital Interruption
Site: Complete interruption of all optic radiation fibers
Defect: Complete contralateral congruous homonymous hemianopia, often with macular sparing
Visual field: Complete loss of contralateral half-field in both eyes, but central (macular) 5-10° is preserved
Why macular sparing? Multiple reasons:
- Large cortical representation of the macula in the occipital pole (more likely to partially survive)
- Bilateral macular representation - some ipsilateral cortex also represents the macula
- The occipital pole has dual blood supply (PCA + MCA collaterals)
Clinical causes: PCA (posterior cerebral artery) infarct
Lesion 8 - Incomplete / Partial Visual Cortex Lesion
Site: Incomplete damage to the visual cortex (striate cortex, Area 17)
Defect: Congruous homonymous scotomas, often with macular involvement
Visual field: Small, well-defined congruous scotomas - can be central if macular cortex affected
Clinical causes: Small PCA branch occlusion, cortical contusion
IV. SUMMARY TABLE - ALL LESIONS AT A GLANCE
| Lesion Site | Visual Field Defect | Congruity | Macular | Cause |
|---|---|---|---|---|
| Optic nerve | Monocular blindness (ipsilateral) | N/A | Affected | Optic neuritis, trauma |
| Lateral chiasm | Ipsilateral nasal hemianopia | Incongruous | Spared | ICA aneurysm |
| Central chiasm | Bitemporal hemianopia | Heteronymous | Spared initially | Pituitary adenoma |
| Optic tract | Contralateral homonymous hemianopia | Incongruous | Affected | Pituitary extension |
| Meyer's loop (temporal) | Contralateral superior quadrantanopia | Congruous | Spared | Temporal lobectomy, TL tumor |
| Parietal radiation | Contralateral inferior quadrantanopia | Congruous | Spared | Parietal tumor, MCA infarct |
| Complete radiation / PCA | Contralateral homonymous hemianopia | Congruous | Spared | PCA infarct |
| Visual cortex (partial) | Congruous homonymous scotoma | Congruous | Affected | Small PCA branch |
V. IMPORTANT CLINICAL RULES (General Rules of Visual Fields)
The Bradley and Daroff's Neurology textbook states these key rules:
- A lesion anterior to the chiasm affects only one eye
- Only a chiasmal lesion causes true bitemporal hemianopia
- Retrochiasmal lesions produce homonymous visual field defects (same side lost in both eyes)
- Anterior retrochiasmal lesions (optic tract) produce incongruent homonymous defects
- Posterior retrochiasmal lesions (optic radiation, cortex) produce congruent defects
- Postgeniculate lesions (radiation, cortex): normal fundus, intact pupillary reflexes - because pupillary fibers leave the pathway at the optic tract level, before the LGN
VI. KEY POINTS FOR EXAM
- Bitemporal hemianopia = pituitary adenoma - most tested clinical correlation
- Meyer's loop = temporal lobe = superior field loss ("pie in the sky")
- Parietal radiation = inferior field loss ("pie on the floor")
- Macular sparing = PCA infarct - the macula is spared because it has a large occipital representation and dual blood supply
- Congruous = posterior lesion; Incongruous = anterior/tract lesion
- Pupillary reflex intact with cortical blindness - because pupillary fibers leave at the optic tract (pretectal area), not the cortex
- The right optic tract / radiation / cortex represents the left visual field of both eyes
- The calcarine fissure: upper lip = lower visual field; lower lip = upper visual field
Sources: Ganong's Review of Medical Physiology (26th ed.), Goldman-Cecil Medicine (International Edition), Gray's Anatomy for Students, Bradley and Daroff's Neurology in Clinical Practice
Answer According to exam pov
The previous answer already had all the textbook content. Let me now reformat it into a clean, exam-ready answer with the ideal structure university examiners expect.
VISUAL PATHWAY
(Long Answer / 10-15 marks | University Exam Format)
INTRODUCTION
The visual pathway is the neural pathway that transmits visual impulses from the retina to the primary visual cortex in the occipital lobe.
COMPONENTS (write this as a flow chart in your answer)
Retina (Rods & Cones)
↓
Bipolar cells → Ganglion cells
↓
Optic Nerve (CN II)
↓
Optic Chiasma
↓
Optic Tract
↓
Lateral Geniculate Body (LGB) of Thalamus
↓
Optic Radiation (Geniculocalcarine tract)
↓
Primary Visual Cortex (Area 17, Calcarine fissure, Occipital lobe)
DIAGRAM
(Draw this in your paper - simple and clear)
DESCRIPTION OF EACH COMPONENT
1. Retina
- Innermost layer of the eye
- Contains rods (peripheral; scotopic/dim light vision) and cones (fovea; photopic/color vision)
- Image on retina is inverted and laterally reversed
- Ganglion cell axons converge at the optic disc → this creates the physiological blind spot (no photoreceptors here)
2. Optic Nerve (CN II)
- Formed by axons of ~1.2 million retinal ganglion cells
- Passes through the optic canal to enter the cranial cavity
- Covered by all 3 meningeal sheaths (pia, arachnoid, dura) → it is a CNS structure, not a peripheral nerve
- Contains fibers from both nasal and temporal halves of the ipsilateral retina
3. Optic Chiasma
- Lies anterior to the pituitary stalk, above the pituitary gland
- Site of partial decussation - the most important point to remember:
| Fiber type | Origin | Action at chiasma |
|---|---|---|
| Nasal (medial) retinal fibers | Inner half of retina | Cross to opposite optic tract |
| Temporal (lateral) retinal fibers | Outer half of retina | Stay ipsilateral |
- Result: Each optic tract now carries fibers representing the contralateral visual field from both eyes
- Macular fibers occupy the posterior part of the chiasma
4. Optic Tract
- Runs around the midbrain from the chiasma to the LGB
- Each tract carries:
- Temporal fibers from the ipsilateral eye
- Nasal fibers from the contralateral eye
- (Both representing the same - contralateral - visual field)
- Before reaching LGB, a small bundle branches off to the pretectal nucleus (pupillary light reflex pathway) and superior colliculus (visual reflexes)
5. Lateral Geniculate Body (LGB)
- Located in the posterior thalamus
- Has 6 layers (numbered 1-6 from ventral to dorsal):
- Layers 1 & 2 → Magnocellular (large cells) → M pathway → motion, depth, coarse form
- Layers 3-6 → Parvocellular (small cells) → P pathway → color, fine detail
- Layers 1, 4, 6 → input from contralateral eye
- Layers 2, 3, 5 → input from ipsilateral eye
- Retinotopic (point-for-point) map of the retina is maintained
6. Optic Radiation (Geniculocalcarine Tract)
- Axons from LGB fan out as the optic radiation
- Divided into two important bundles:
| Bundle | Course | Field represented |
|---|---|---|
| Superior fibers | Directly through parietal lobe → superior lip of calcarine fissure | Lower visual field |
| Inferior fibers (Meyer's loop) | Loop forward into temporal lobe around inferior horn of lateral ventricle, then back | Upper visual field |
Exam tip: Meyer's loop is tested frequently. Damage here → contralateral superior quadrantanopia ("pie in the sky")
7. Primary Visual Cortex (Area 17 / Striate Cortex)
- Located on both lips of the calcarine fissure in the medial occipital lobe
- Retinotopic organization:
- Upper lip of calcarine → lower visual field
- Lower lip of calcarine → upper visual field
- Posterior pole (occipital tip) → macular (central) vision - large area
- Anterior part → peripheral vision
- Sends signals to visual association areas (V2, V3, V4-color, V5-motion)
VISUAL FIELD DEFECTS DUE TO LESIONS
Terminology to know:
| Term | Meaning |
|---|---|
| Hemianopia | Loss of half the visual field |
| Quadrantanopia | Loss of one quarter of visual field |
| Homonymous | Same side lost in both eyes |
| Heteronymous | Opposite sides lost in each eye |
| Congruous | Identical defect in both eyes (posterior lesion) |
| Incongruous | Defect differs between eyes (anterior/tract lesion) |
| Macular sparing | Central vision preserved despite hemianopia |
| Scotoma | Localized area of visual loss |
LESION 1 - Optic Nerve
| Feature | Details |
|---|---|
| Defect | Complete monocular blindness (ipsilateral eye) |
| Type | Amaurosis of one eye |
| Other eye | Normal |
| Pupil | APD (Marcus Gunn pupil) on affected side |
| Causes | Optic neuritis (MS), retinal artery occlusion, trauma |
LESION 2 - Lateral Optic Chiasma
| Feature | Details |
|---|---|
| Defect | Ipsilateral nasal hemianopia |
| Cause | ICA aneurysm pressing on lateral chiasma |
| Note | Rare; usually incongruous |
LESION 3 - Central Optic Chiasma ⭐ (Most Important)
| Feature | Details |
|---|---|
| Defect | Bitemporal hemianopia (both outer fields lost) |
| Type | Heteronymous hemianopia |
| Mechanism | Decussating nasal fibers from both eyes destroyed → both temporal fields lost |
| Causes | Pituitary adenoma (most common), craniopharyngioma, meningioma |
| Note | Superior fields affected first (inferior chiasma compressed first by pituitary tumor expanding upward) |
LESION 4 - Optic Tract
| Feature | Details |
|---|---|
| Defect | Contralateral incongruous homonymous hemianopia |
| Example | Right optic tract lesion → left field lost in both eyes |
| Congruity | Incongruous (fibers not yet fully interdigitated) |
| Pupil | Wernicke's hemianopic pupil (no pupillary response when light shone in the blind half-field) |
| Causes | Lateral extension of pituitary tumor, temporal lobe herniation |
LESION 5 - Meyer's Loop (Temporal Lobe) ⭐
| Feature | Details |
|---|---|
| Defect | Contralateral congruous homonymous superior quadrantanopia |
| Memory aid | "Pie in the sky" |
| Mechanism | Inferior optic radiation fibers (carrying upper field information) damaged |
| Causes | Temporal lobectomy (surgery for epilepsy), MCA infarct, temporal lobe tumor |
LESION 6 - Parietal Lobe (Superior Radiation)
| Feature | Details |
|---|---|
| Defect | Contralateral congruous homonymous inferior quadrantanopia |
| Memory aid | "Pie on the floor" |
| Associated signs | Hemisensory loss, neglect, dressing apraxia (parietal signs) |
| Causes | Parietal lobe tumor, MCA superior division infarct |
LESION 7 - Complete Optic Radiation / PCA Infarct ⭐
| Feature | Details |
|---|---|
| Defect | Complete contralateral congruous homonymous hemianopia with macular sparing |
| Macular sparing | Yes - central 5-10° of vision preserved |
| Why macular sparing? | 1. Large cortical representation of macula (more likely to survive partial infarct) 2. Dual blood supply of occipital pole (PCA + MCA collaterals) 3. Some bilateral macular representation |
| Causes | PCA (posterior cerebral artery) infarct - most classic |
| Pupil | Normal (pupillary fibers leave before LGB) |
| Fundus | Normal (postgeniculate lesion) |
LESION 8 - Partial Visual Cortex Lesion
| Feature | Details |
|---|---|
| Defect | Congruous homonymous scotomas (can be central) |
| Causes | Small PCA branch occlusion, cortical contusion |
MASTER SUMMARY TABLE (Draw this in exam - gives full marks)
| # | Lesion Site | Visual Field Defect | Congruity | Causes |
|---|---|---|---|---|
| 1 | Optic nerve | Monocular blindness (ipsilateral) | - | Optic neuritis, trauma |
| 2 | Lateral chiasm | Ipsilateral nasal hemianopia | Incongruous | ICA aneurysm |
| 3 | Central chiasm | Bitemporal hemianopia | Heteronymous | Pituitary adenoma |
| 4 | Optic tract | Contralateral homonymous hemianopia | Incongruous | Pituitary extension |
| 5 | Meyer's loop | Contralateral superior quadrantanopia | Congruous | Temporal lobectomy |
| 6 | Parietal radiation | Contralateral inferior quadrantanopia | Congruous | Parietal tumor |
| 7 | Complete radiation | Contralateral homonymous hemianopia + macular sparing | Congruous | PCA infarct |
| 8 | Visual cortex (partial) | Congruous homonymous scotoma | Congruous | Small PCA branch |
IMPORTANT RULES TO WRITE IN EXAM
- Lesions anterior to the chiasm → affect only one eye
- Lesions at the chiasm → bitemporal hemianopia (heteronymous)
- Lesions posterior to the chiasm → homonymous defects (same field lost in both eyes)
- More posterior the lesion → more congruous the defect
- Macular sparing = PCA infarct (occipital lobe)
- Pupillary reflexes are preserved in lesions posterior to the optic tract (LGB, radiation, cortex) because pupillary fibers leave at the pretectal level
- Normal fundus on ophthalmoscopy with postgeniculate lesions (no optic atrophy)
APPLIED / CLINICAL CORRELATIONS (Bonus marks)
| Clinical Condition | Visual Field Defect | Mechanism |
|---|---|---|
| Pituitary adenoma | Bitemporal hemianopia | Upward compression of central chiasm |
| Multiple sclerosis | Monocular visual loss (optic neuritis) | Demyelination of optic nerve |
| PCA stroke | Homonymous hemianopia with macular sparing | Occipital lobe infarct |
| Temporal lobe surgery | Superior quadrantanopia ("pie in sky") | Meyer's loop damage |
| Occipital lobe tumor | Congruous homonymous hemianopia | Visual cortex compression |
| MCA parietal infarct | Inferior quadrantanopia | Superior radiation damage |
Exam strategy: This question is typically asked as a 10-mark long answer. Always include: (1) a labeled diagram, (2) the relay station description, (3) the lesion table, and (4) at least 2-3 clinical applications. The three most-tested lesions are central chiasma (pituitary), Meyer's loop, and PCA infarct with macular sparing.
This is a shared conversation. Sign in to Orris to start your own chat.