Hey orris i am a third year obgyn resident preparing for my ms final exams. Teach me HIV in pregnancy in accordance with the standard textbooks and all recent guidelines
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"HIV" AND "pregnancy" AND "antiretroviral"
Reading File
Finding Sources
Finding Sources
Reading File
Searching the Web
WHO DHHS 2024 2025 HIV in pregnancy antiretroviral guidelines recommendations
Reading File
Reading Web Page
https://clinicalinfo.hiv.gov/en/guidelines/perinatal/introdu…
Reading File
Loading Image
I now have comprehensive material. Let me compile the full teaching answer.
HIV in Pregnancy - A Complete Guide for MS Finals
Based on Creasy & Resnik's Maternal-Fetal Medicine (8th ed.), NIH/DHHS Perinatal Guidelines (updated June 2025), WHO Consolidated HIV Guidelines, and BHIVA 2025
1. Epidemiology and Background
- Without any intervention, HIV mother-to-child transmission (MTCT) occurs in ~25% of pregnancies, rising to ~40% if breastfeeding continues to 12 months.
- Since the landmark PACTG 076 trial (1994) - which showed ZDV monotherapy reduced MTCT from 25% to 8% - the world has seen a dramatic decline.
- With modern combination ART throughout pregnancy and no breastfeeding, MTCT is now <1% in high-income settings.
- Globally, ~2,000 HIV-exposed infants are born daily; 90% of cases are in sub-Saharan Africa.
- Nearly all pediatric HIV infection today is through perinatal transmission (not horizontal).
2. Pathophysiology of MTCT - Timing and Mechanisms
| Timing | Mechanism | Notes |
|---|---|---|
| In utero (early) | Transplacental virus passage | ~38% of infected infants test positive within 48 hrs of birth |
| In utero (late) | Ascending infection with prolonged ROM | More rapid disease course than intrapartum |
| Intrapartum | Contact with infected maternal blood/secretions | Majority of perinatal cases; 93% positive by Day 14 |
| Postnatal | Breastfeeding | ~16% risk per exposure; key global challenge |
Maternal predictors of enhanced MTCT:
- High maternal viral load (most important)
- Low CD4+ count / immunosuppression
- Viral characteristics: chemokine receptor tropism (R5 vs. X4), resistance patterns
- Obstetric variables: delivery mode, duration of ROM, chorioamnionitis
- Seroconversion during pregnancy or breastfeeding (high-risk window)
- Co-infections: syphilis, other STIs, CMV
- Drug abuse, heterosexual transmission from high-risk partner
3. Screening in Pregnancy
Universal, opt-out HIV testing with a 4th-generation HIV test is the standard of care at the first antenatal visit.
The 4th-generation test detects both HIV-1/HIV-2 antibodies AND the HIV-1 p24 antigen, enabling diagnosis as early as 2 weeks after exposure (vs. 3-4 weeks for older antibody-only tests).
CDC 3-Step Testing Algorithm:
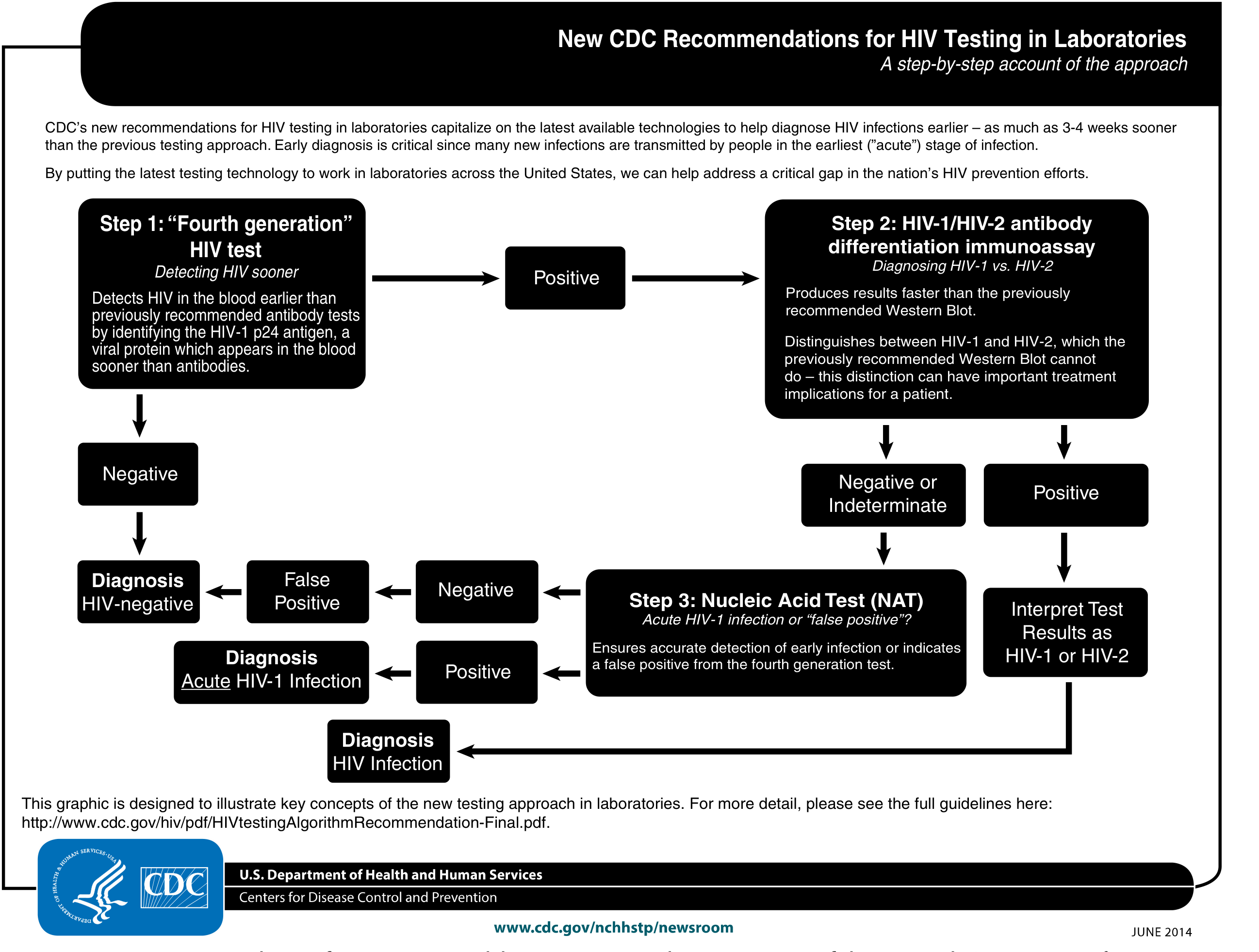
Step 1: 4th-generation HIV-1/2 Ag/Ab combination immunoassay
- If positive → Step 2
- If negative → HIV-negative (done)
Step 2: HIV-1/HIV-2 antibody differentiation immunoassay
- Distinguishes HIV-1 from HIV-2 (treatment implications differ)
- If negative/indeterminate → Step 3
Step 3: Nucleic Acid Test (NAT/RNA PCR)
- Detects acute HIV-1 infection or confirms false positive
When to Repeat Testing:
- High-risk women (seropositive partner, high-prevalence area): repeat in 3rd trimester
- STI diagnosed or symptoms of acute HIV: repeat immediately
- Expedited testing during labor for women at increased risk who were not retested in 3rd trimester
- In labor with unknown status: rapid HIV test (result within 1 hour)
4. PrEP in Pregnancy
Women at risk of HIV seroconversion during pregnancy should receive pre-exposure prophylaxis (PrEP):
- Regimen: Tenofovir disoproxil fumarate/emtricitabine (TDF/FTC) oral combination
- Indications: Condomless sex with a partner with detectable/unknown HIV RNA, recent STI, injection drug use
- Safe in pregnancy and postpartum/breastfeeding period
5. Baseline Workup After HIV Diagnosis in Pregnancy
- CD4+ T-cell count
- HIV RNA viral load (quantitative PCR)
- Resistance testing (genotype) - before ART initiation if viral load >500-1000 copies/mL
- Hepatitis B and C serology (affects ART choice)
- Full STI screen (syphilis, gonorrhea, chlamydia)
- TB screening (affects ART timing)
- CBC, LFTs, renal function
6. ART in Pregnancy - When to Start
ALL pregnant women with HIV should receive combination ART (cART) regardless of CD4 count, viral load, or clinical stage. This is the WHO Option B+ approach and the current DHHS/ACOG/BHIVA standard.
- ART-naive woman: Start as soon as possible after diagnosis (ideally by end of 1st trimester)
- Already on ART: Continue the same regimen (if virologically suppressed and no teratogenicity concerns)
- Do NOT interrupt ART postpartum - continue lifelong
7. ART Regimen Selection in Pregnancy
Preferred Backbone: 2 NRTIs
| NRTI Combination | Notes |
|---|---|
| TDF + FTC (tenofovir DF + emtricitabine) | Preferred; also covers HBV |
| TAF + FTC | Alternative (less bone/renal toxicity) |
| ABC + 3TC (abacavir + lamivudine) | Preferred if HBsAg positive; requires HLA-B*5701 testing |
| ZDV + 3TC (zidovudine + lamivudine) | Historical; still used in resource-limited settings |
Preferred 3rd Agent: INSTI (Integrase Strand Transfer Inhibitor)
This is the most high-yield point for exams:
| Drug | 2025 Status | Key Points |
|---|---|---|
| Dolutegravir (DTG) | Preferred (WHO 2021, BHIVA 2025, DHHS 2025) | Rapid viral suppression; concerns about NTD (neural tube defects) have been largely resolved by Tsepamo study - risk is very low (~0.1%) and outweighed by benefits; avoid in 1st trimester only if feasible |
| Bictegravir (BIC) | Newly preferred (DHHS 2025) | Rapid suppression; high genetic barrier to resistance; good tolerability |
| Raltegravir (RAL) | Preferred when rapid VL suppression needed (e.g., presenting in 3rd trimester with high VL) | Crosses placenta well; rapid suppression |
Drugs to AVOID in Pregnancy:
| Drug | Reason |
|---|---|
| Efavirenz (EFV) | Historically avoided in 1st trimester (NTD risk in primates); now classified as acceptable but not preferred |
| Lopinavir/ritonavir (LPV/r) | Increased risk of preterm birth; use DRV/r or ATV/r if PI needed |
| Didanosine + Stavudine | Severe lactic acidosis in pregnancy (black box) |
| Nevirapine | Risk of severe hepatotoxicity/skin rash in women with CD4 >250; avoid as new initiation |
Special Situation - High Viral Load Presenting Late:
If presenting >28 weeks with VL >100,000 copies/mL or unknown VL:
- Consider raltegravir as part of the regimen (proven more rapid VL suppression than other ARVs in this scenario) - per DHHS 2025
8. Monitoring During Pregnancy
| Timepoint | What to Check |
|---|---|
| Initiation of ART | Viral load, CD4, LFTs, renal function |
| Every visit (monthly) | Adherence, side effects |
| 4 weeks after ART start | Viral load (confirm suppression trajectory) |
| 32-36 weeks | Viral load (the critical decision point for mode of delivery) |
| At delivery | Viral load if not done recently |
9. Mode of Delivery
This is one of the most important clinical decisions in HIV management in pregnancy:
| Viral Load at ~36 Weeks | Recommended Delivery Mode |
|---|---|
| <1,000 copies/mL (undetectable or low) | Vaginal delivery - safe; no additional benefit from cesarean |
| ≥1,000 copies/mL | Elective cesarean delivery at 38 weeks (before labor/ROM) |
Why 38 weeks for cesarean? To minimize duration of rupture of membranes (ROM), which is independently associated with intrapartum MTCT. Duration of ROM significantly increases transmission risk.
Evidence base: In a meta-analysis of 15 North American and European cohorts (n=8,533 mother-infant pairs), scheduled cesarean delivery reduced MTCT from 7.3% to 2% compared to other delivery modes. However, this was from the ZDV monotherapy era - with modern cART and undetectable VL, vaginal delivery is equally safe.
Key point on IV ZDV during labor:
- Historically: IV ZDV (2 mg/kg loading then 1 mg/kg/hr) was given during labor to all HIV-positive women
- Current recommendation: If VL is consistently undetectable on cART, IV ZDV is NOT required - continue current oral ART regimen through labor and delivery
- IV ZDV is still recommended when VL is detectable/unknown near delivery or when ART was not received
Intrapartum precautions:
- Avoid fetal scalp electrodes (FSE) - breach skin barrier
- Avoid fetal scalp blood sampling
- Minimize instrumental delivery
- Avoid amniotomy unless necessary
- Minimize episiotomy
10. Postpartum Management
- Continue ART lifelong (WHO Option B+, DHHS recommendation) - do NOT stop after delivery
- Monitor viral load 6 weeks postpartum
- Emotional support, adherence counseling
- Contraception counseling (note: some ARVs interact with hormonal contraceptives - particularly boosted PIs and NNRTIs can reduce efficacy of combined oral contraceptives)
11. Infant Feeding
| Setting | Recommendation |
|---|---|
| High-resource (US, UK) | Formula feeding preferred - eliminates postnatal transmission risk entirely |
| Low-resource (sub-Saharan Africa) | Breastfeeding with maternal ART - WHO recommends exclusive breastfeeding + maternal cART until weaning; reduces MTCT to <2% |
Updated DHHS 2025 position: If a mother on cART has consistently undetectable VL throughout pregnancy and postnatally with appropriate neonatal prophylaxis, the risk of postnatal transmission via breastfeeding may be as low as ~1%. High-income country guidelines (US, Canada, UK, Switzerland) now recommend patient-centered, evidence-based counseling that includes breastfeeding as an option - a major shift from the blanket "do not breastfeed" recommendation.
Key note: Risk of breastfeeding transmission from an HIV-positive mother is approximately 16% overall in untreated/unsuppressed women. Seroconversion during breastfeeding carries highest risk.
12. Neonatal Management
Neonatal ARV Prophylaxis vs. Presumptive Therapy
All HIV-exposed infants receive some ARV regimen. The choice depends on maternal risk:
LOW-RISK infant (mother on ART with consistently undetectable VL):
- ZDV alone for 4-6 weeks
HIGH-RISK infant - defined as infant whose mother:
- Received no antepartum ART, OR
- Received only intrapartum ART, OR
- Had suboptimal viral suppression (VL ≥50 copies/mL) within 4 weeks of delivery, OR
- Had acute/primary HIV infection during pregnancy or breastfeeding
High-risk infants receive presumptive HIV therapy (3-drug ART at treatment doses):
- ZDV + 3TC + Nevirapine (3 doses NVP in first week of life + 6 weeks ZDV) - shown more efficacious than ZDV alone
- Or a full 3-drug regimen at treatment doses
Neonatal HIV Diagnosis (Serial NAAT):
- Birth (within 48 hours): Detects in utero infection
- 14-21 days: Detects intrapartum infection (may be negative at birth)
- 1-2 months
- 4-6 months
Remember: Maternal HIV antibodies (IgG) cross the placenta, so ALL HIV-exposed infants are antibody-positive until 15-18 months. Antibody tests (ELISA/Western blot) are useless for infant diagnosis before 18 months. Diagnosis in infants relies on PCR (DNA or RNA).
PCR sensitivity: Reaches 96% by 4 weeks of age (in absence of breastfeeding).
Two consecutive negative virologic tests (one at ≥1 month and one at ≥4 months) reliably excludes HIV infection in non-breastfed infants.
13. Effects of HIV/ART on Pregnancy Outcomes
Maternal HIV Effects:
- Generally asymptomatic during pregnancy in high-income countries
- Advanced disease: risk of reactivating CMV, toxoplasmosis, HSV
- Higher risk of STIs (syphilis, HTLV-1, Hep C co-infections in endemic areas)
ART Effects on Fetus/Neonate:
| Concern | Detail |
|---|---|
| Preterm birth | Increased risk with LPV/r-containing regimens; DTG/BIC-based regimens have better safety profile |
| Neural tube defects (DTG) | Early Tsepamo study (Botswana, 2018) reported 0.9% NTD risk with periconceptional DTG vs 0.1% with non-DTG. Larger follow-up reduced this concern significantly. WHO and DHHS now recommend DTG as preferred. |
| SGA/IUGR | Some PI-containing regimens; monitor fetal growth |
| Mitochondrial toxicity | NRTI class; theoretical concern in exposed-uninfected infants; ZDV and ddI most implicated |
| Hyperbilirubinemia | Atazanavir (UGT inhibitor); monitor neonatal jaundice |
14. Summary of Risk Reduction - A Framework
No treatment → MTCT risk 25-40%
ZDV monotherapy → MTCT risk ~8% (PACTG 076)
Elective C/S alone → MTCT risk ~2% (pre-HAART era)
cART + vaginal birth → MTCT risk <1%
cART + no breastfeed → MTCT risk <0.1% (approaching zero)
15. Recent Evidence to Know (2024-2025)
| Study/Guideline | Finding |
|---|---|
| Dugdale et al., Lancet, 2025 (PMID 40652949) | Systematic review and meta-analysis confirming maternal viral load is the single strongest predictor of both perinatal and postnatal HIV transmission |
| Walters et al., Lancet HIV, 2025 (PMID 40753992) | Meta-regression on probability of vertical transmission across different ARV regimens and settings |
| Gandhi et al., JAMA, 2025 (PMID 39616604) | IAS-USA 2024 guidelines - bictegravir + DTG are now the top-tier preferred INSTIs in pregnancy |
| DHHS Perinatal Guidelines, June 2025 | Added bictegravir as a preferred agent; updated breastfeeding counseling to include patient-centered discussion of breastfeeding option in virologically suppressed women |
| WHO, September 2025 | Updated integrated HIV service delivery guidelines, reaffirming DTG-based first-line in pregnancy |
16. Exam High-Yield Points - Quick Bullets
- The 4th-generation test (p24 Ag + Ab) diagnoses HIV 2 weeks earlier than older tests
- Opt-out testing has significantly improved uptake in pregnancy
- MTCT risk without treatment: 25% (pregnancy alone), 40% (including breastfeeding to 12 months)
- MTCT risk with optimal modern cART: <1%
- Preferred ART in pregnancy (2025): DTG or BIC + TDF/FTC (or TAF/FTC)
- Elective C/S at 38 weeks is indicated when VL ≥1,000 copies/mL near delivery
- IV ZDV intrapartum is NOT needed if VL is undetectable on cART
- Neonatal prophylaxis: ZDV x 4-6 weeks (low risk) OR 3-drug ART (high risk)
- Infant diagnosis: DNA/RNA PCR at 48 hrs, 14-21 days, 1-2 months, 4-6 months (NOT antibody test before 18 months)
- Breastfeeding in US/UK: Formula feeding preferred; with undetectable maternal VL, breastfeeding now an option per 2025 DHHS counseling guidelines
- LPV/r is associated with preterm birth - use DRV/r or ATV/r if PI needed
- Do not stop ART postpartum - continue lifelong
Sources: Creasy & Resnik's Maternal-Fetal Medicine 8th ed., Chapter 49 | NIH DHHS Perinatal Guidelines (June 2025) | WHO Consolidated HIV Guidelines 2021/2025 | BHIVA 2025 | Dugdale et al., Lancet 2025 | Gandhi et al., JAMA 2025
This is a shared conversation. Sign in to Orris to start your own chat.