Dacryocystitis
Reading File
Finding Sources
Searching PubMed
dacryocystitis
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative sources. Here is the full clinical summary:
Dacryocystitis
Dacryocystitis is infection/inflammation of the lacrimal sac, nearly always caused by obstruction of the nasolacrimal duct (NLD), leading to stasis and bacterial overgrowth.
Anatomy Recap
The lacrimal sac (10-12 mm long) sits in the lacrimal fossa between the anterior and posterior lacrimal crests. Tears drain from the puncta → canaliculi → lacrimal sac → NLD → inferior nasal meatus (past the valve of Hasner). Obstruction at any point below the sac leads to stasis and infection.
Etiology
- Primary cause: Nasolacrimal duct obstruction (NLDO) - the vast majority of cases
- Less common: Lacrimal sac diverticula, dacryoliths, nasal/sinus surgery, trauma, lacrimal sac tumors
- Pathogens (acute): Staphylococci, Streptococcus pneumoniae, Haemophilus influenzae (especially in children)
- Special populations: Gram-negative organisms and atypical bacteria are more common in diabetics, immunocompromised patients, and nursing home residents
- MRSA should be considered in appropriate epidemiological contexts
Classification
Acute Dacryocystitis
- Symptoms: Subacute onset of pain at the medial canthal area, epiphora, fever/chills
- Signs:
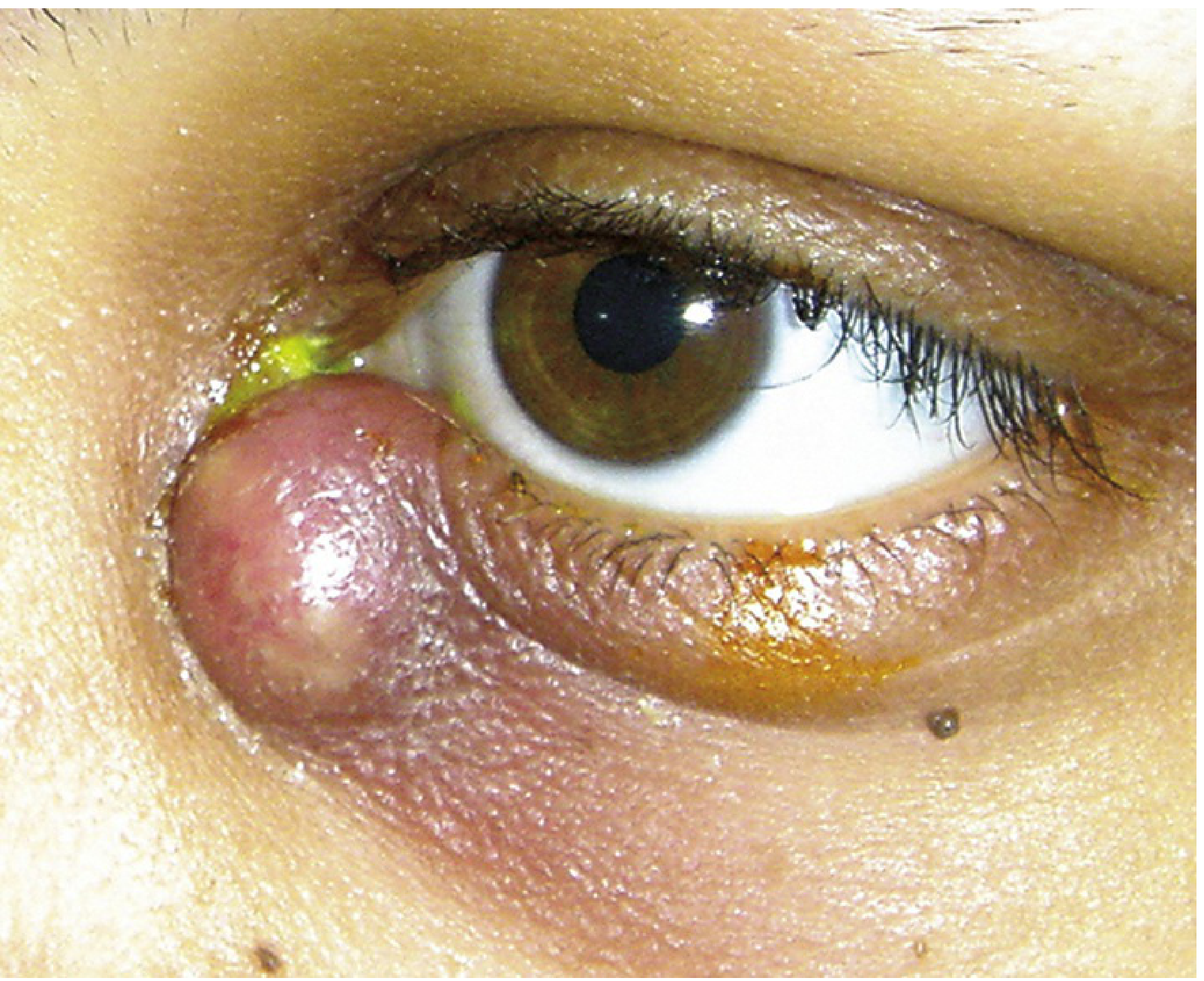
- Erythematous, tender, tense swelling below the medial canthal tendon (this is the key anatomical landmark)
- Mucoid or purulent discharge expressible from the punctum on pressure over the sac
- May progress to abscess formation and preseptal cellulitis
- Fistula formation from skin (below medial canthal tendon) is a known complication
Key sign: Swelling in dacryocystitis is always below the medial canthal tendon. A mass above the tendon suggests a lacrimal sac tumor (rare) - Wills Eye Manual
Chronic Dacryocystitis
- Symptoms: Chronic epiphora, recurrent unilateral conjunctivitis
- Signs: Painless swelling at the inner canthus (mucocele), or pressure over sac elicits mucopurulent canalicular reflux even without obvious swelling
- Can progress to lacrimal sac abscess; rarely orbital or facial cellulitis
Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| Preseptal/facial cellulitis | No punctal discharge on pressure; patent lacrimal system on irrigation |
| Dacryocystocele | Non-inflamed, present at birth; in infants |
| Acute ethmoid sinusitis | Tenderness over nasal bone medial to inner canthus; imaging diagnostic |
| Frontal sinus mucocele | Swelling above medial canthal tendon; proptosis; downward globe displacement |
| Lacrimal sac tumor | Mass above medial canthal tendon; no discharge |
Workup
- History: Prior episodes, ENT infections, sinus disease, trauma, surgery
- External exam: Gentle pressure over the lacrimal sac with cotton-tipped swab to express discharge from punctum - do bilaterally
- Orbital assessment: Pupillary response, extraocular motility, globe position (rule out concurrent orbital cellulitis)
- Microbiology: Gram stain and blood agar culture of expressed discharge; use chocolate agar in children (for H. influenzae)
- Imaging (CT orbits + paranasal sinuses): In atypical, severe, or antibiotic-unresponsive cases
Do NOT attempt to probe or irrigate the lacrimal system during acute infection - Kanski's & Wills Eye Manual
Treatment
Acute Dacryocystitis
Conservative (first line):
- Warm compresses + gentle massage q.i.d.
- Topical antibiotics (e.g., trimethoprim/polymyxin B q.i.d.) as adjunct - topical alone is NOT adequate
Systemic antibiotics:
Adults:
| Severity | Regimen |
|---|---|
| Mild, afebrile, systemically well | Cephalexin 500 mg PO q6h or Amoxicillin/clavulanate 875/125 mg PO b.i.d. |
| Suspected MRSA | TMP-SMX DS (160/800 mg) PO q12h or Clindamycin 300 mg PO t.i.d. |
| Febrile, acutely ill | Hospitalize; Cefazolin 1 g IV q8h |
Children:
| Severity | Regimen |
|---|---|
| Mild, afebrile | Amoxicillin/clavulanate 25-45 mg/kg/d PO in 2 divided doses (max 90 mg/kg/d) |
| Moderate-severe / febrile | Hospitalize; Cefuroxime 50-100 mg/kg/d IV in 3 divided doses |
| Suspected MRSA | Vancomycin 10-13 mg/kg IV q6-8h |
- Adjust based on culture/sensitivity
- Total course: 10-14 days
Surgical:
- Incision and drainage (I&D): Reserved for a pointing, fluctuant abscess about to spontaneously drain - carries risk of persistent sac-skin fistula
- Dacryocystorhinostomy (DCR): Definitive surgery after acute infection resolves; creates anastomosis between lacrimal sac and nasal mucosa, bypassing NLD obstruction; indicated for recurrent or chronic dacryocystitis
Chronic Dacryocystitis
- Definitive treatment: Dacryocystorhinostomy (DCR)
- A 2025 meta-analysis (PMID 39762863) comparing transcanalicular laser-assisted vs. external DCR for primary acquired NLDO confirms external DCR remains the gold standard for anatomical and functional success
Follow-Up
- Acute: Daily until improvement confirmed; hospitalize and start IV antibiotics if outpatient condition worsens
- Post-resolution: Probing and irrigation to assess NLD patency; refer for DCR if obstruction confirmed or recurrence occurs
Important Clinical Pearls
- Postpone intraocular surgery if any signs of lacrimal drainage system infection - risk of endophthalmitis (Kanski's Clinical Ophthalmology)
- In children, dacryocystitis is usually a secondary bacterial infection following viral upper respiratory infection
- Improperly treated dacryocystitis can lead to periorbital/orbital cellulitis - children often require hospitalization
Sources: Kanski's Clinical Ophthalmology 10th ed.; The Wills Eye Manual; Tintinalli's Emergency Medicine; Textbook of Family Medicine 9th ed.
Indications and complications of endonasal dcr
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching PubMed
endonasal endoscopic dacryocystorhinostomy indications complications
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
I now have comprehensive information. Here is the full answer:
Endonasal (Endoscopic) DCR - Indications & Complications
Endonasal/endoscopic DCR creates a direct anastomosis between the lacrimal sac and the nasal cavity entirely through the nose, avoiding any external skin incision. The key technical principle is the widest possible marsupialization of the medial wall of the lacrimal sac - this is the single most critical determinant of success.
Indications
Primary Indications
| Indication | Notes |
|---|---|
| Primary acquired nasolacrimal duct obstruction (PANDO) | Most common indication; anatomic obstruction at the sac-duct junction |
| Chronic dacryocystitis | Recurrent or persistent lacrimal sac infection with NLD obstruction |
| Mucocele / pyocele of the lacrimal sac | Chronic obstruction causing sac distension with mucus or pus |
| Dacryolithiasis | Middle-aged patients with lacrimal duct stones |
| Functional NLD obstruction | Critical narrowings causing delayed lacrimal flow; good patency rates but symptom relief less predictable (~81%) |
| Failed prior external DCR | Endoscopic revision avoids scarred external tissue; revision outcomes: 91.3% anatomic patency, 87% functional success |
| Congenital NLD obstruction | When probing has failed or bony atresia/complex anomalies of upper NLD are present |
| Cosmetically sensitive patients | Avoids the external skin scar of open DCR |
| Bleeding diathesis / anticoagulation | Endonasal approach gives better intraoperative visualization and hemostasis than external; preferred by some surgeons in anticoagulated patients |
| Simultaneous nasal pathology requiring surgery | Additional nasal procedures (septoplasty, turbinoplasty) can be done at the same time (needed in ~50% of endonasal DCRs) |
What Endonasal DCR Cannot Treat
- Obstruction proximal to the common canaliculus (canalicular disease) - DCR alone is insufficient; Lester Jones tube may be required
- Lesions at the punctum or canalicular level require separate management
Contraindications / When Endonasal Is Less Preferred
- Lacrimal sac tumor - requires combined external + endonasal extirpation, not DCR alone
- Extensive medial canthal scarring or trauma distorting anatomy (external approach may be easier)
- Active acute dacryocystitis - surgery deferred until infection resolves
- Surgeon without established rhinologic/endoscopic proficiency - inexperience causes most severe complications; ideally performed as a team with an oculoplastic surgeon and endoscopic otolaryngologist
Complications
Perioperative Complications (Overall ~5% complication rate)
Listed in descending order of frequency (Cummings Otolaryngology):
- Hemorrhage - Most common; usually managed with topical 1:1000 epinephrine and spot bipolar cautery; rarely requires abandoning the procedure
- Orbital fat exposure - Occurs if dissection goes posterior to the uncinate process; the exposed fat re-mucosalizes spontaneously - do not attempt repair; patient must avoid nose-blowing until healed
- Orbital hematoma - Rare but serious; can cause compartment syndrome and vision loss
- Synechiae / granulation tissue obstruction of the ostium - Leading cause of late failure
Surgical Failure
-
Primary causes of endoscopic DCR failure:
- Inadequate bony removal (most common) - any remaining unopened lacrimal sac creates a fluid meniscus and increases lacrimal resistance, causing pump failure
- Insufficient sac marsupialization
- Cicatricial closure of the ostium
-
Silicone stent ("cheese-wiring") - stents placed under too much tension can tear through the lacrimal puncta, causing iatrogenic functional epiphora; reported in ~0.1% of cases
-
Ostial granulomas - 47% form at the ostium edge; most respond to topical steroids; surgical excision or intralesional triamcinolone for obstructing ones; recurrence <5%
-
Lacrimal sac tumor (missed diagnosis) - approximately 1/3 of lacrimal sac tumors present with persistent or recurrent epiphora after DCR; suspect when bloody nasal discharge, medial canthal swelling, or proptosis develop post-operatively
Rare but Serious Complications
| Complication | Comment |
|---|---|
| CSF leak | Due to inadvertent skull base penetration; requires immediate recognition and repair |
| Orbital penetration / EOM injury | Erroneous dissection into the orbit |
| Postoperative frontal/maxillary sinusitis | Damage to sinus drainage pathways; almost exclusively reported in series not involving otolaryngologists |
| CPAP-related air regurgitation | 80% of post-DCR patients on CPAP experience ophthalmic symptoms; half subsequently stop using CPAP |
Success Rates (Comparison)
| Technique | Immediate Success | ~5-Year Success |
|---|---|---|
| Endoscopic DCR | 84-94% | 92% |
| External DCR | 65-100% | 94% |
| Laser-assisted DCR | 47-100% | 38% (poor long-term) |
- For anatomic obstruction: 95-97% success expected
- For functional obstruction: ~81% complete symptom relief (technical patency similar, but underlying pump failure persists in some)
- Laser-assisted DCR has poor long-term results and should generally be avoided as definitive treatment
Key Principles
"Failures in endoscopic DCR are primarily due to inadequate marsupialization of the lacrimal sac mucosa." - Cummings Otolaryngology
"Endonasal DCR has the advantage of creating no external incision, having similar outcomes to external DCR, and being an ideal option for revision cases." - Cummings Otolaryngology
Sources: Cummings Otolaryngology Head and Neck Surgery; Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2
This is a shared conversation. Sign in to Orris to start your own chat.