Why is it necessary to get air out than take oxygen in
- Exhalation clears "dead space" - stale air sitting in your airways (trachea, bronchi) that never reached the alveoli. If you don't fully exhale, your next breath just recirculates that old air.
- A full exhale stretches the diaphragm back to its resting position, allowing a deeper, more efficient next inhale.
- In conditions like asthma or COPD, air gets trapped in the lungs - patients struggle most with getting air out, not in.
Why is intrapleural pressure always negative
- The lungs want to collapse inward - lung tissue is elastic and, because of its elasticity plus the surface tension of alveolar fluid, it constantly tries to recoil inward (toward the hilum).
- The chest wall wants to spring outward - the rib cage and thoracic muscles have their own elastic recoil that pulls outward, away from the lungs.
- The negative pressure is what keeps the lungs inflated against their own tendency to collapse
- It couples lung movement to chest wall movement - when the diaphragm contracts and the chest expands, the lungs are pulled open passively
- It also aids venous return to the heart (the great veins in the thorax are also subject to this negative pressure)
Classification of lung disease
classification of lung diseases obstructive restrictive vascular
Classification of Lung Diseases
I. Functional / Physiological Classification
1. Obstructive Lung Disease
- Definition: Reduced airflow due to airway narrowing or loss of elastic recoil
- PFT pattern: FEV₁/FVC ratio < 0.70 (reduced); TLC normal or increased; air trapping
- Key diseases:
- COPD (chronic bronchitis + emphysema)
- Bronchial asthma
- Bronchiectasis
- Cystic fibrosis
- Alpha-1 antitrypsin deficiency
- Bronchiolitis / bronchiolitis obliterans
- After lung or stem-cell transplantation
2. Restrictive Lung Disease
-
Definition: Reduced lung volumes due to stiff lungs or mechanical constraints on expansion
-
PFT pattern: FEV₁/FVC ratio normal or increased; TLC reduced
-
Two major subtypes:A. Parenchymal (intrinsic) restriction - the lung tissue itself is abnormal:
- Idiopathic pulmonary fibrosis (IPF)
- Nonspecific interstitial pneumonitis (NSIP)
- Sarcoidosis
- Asbestosis, silicosis, berylliosis (pneumoconioses)
- Eosinophilic pneumonia
- Congestive heart failure
- Drug-induced (amiodarone, methotrexate, nitrofurantoin)
B. Extra-parenchymal (extrinsic) restriction - the lung is normal but can't expand:- Chest wall/skeletal: Obesity, kyphoscoliosis, ankylosing spondylitis, pregnancy
- Neuromuscular: Guillain-Barre syndrome, myasthenia gravis, ALS, muscular dystrophy, diaphragmatic paralysis, botulism
- Pleural: Pleural fibrosis (fibrothorax), rheumatoid arthritis, asbestosis
- Surgical: Lung resection
3. Mixed (Obstructive + Restrictive) Pattern
- Bronchiectasis
- Cystic fibrosis
- Sarcoidosis
- Hypersensitivity pneumonitis
- Pulmonary Langerhans cell histiocytosis
- Lymphangioleiomyomatosis
- Congestive heart failure
II. Anatomical / Structural Classification
| Structure | Diseases |
|---|---|
| Airways (large) | Asthma, COPD, tracheal stenosis |
| Airways (small) | Bronchiolitis, bronchiectasis |
| Alveoli/parenchyma | Pneumonia, ARDS, IPF, emphysema |
| Interstitium | ILD, sarcoidosis, fibrosis |
| Pleura | Pleuritis, pneumothorax, effusion, mesothelioma |
| Pulmonary vasculature | Pulmonary hypertension, PE, vasculitis |
| Chest wall/diaphragm | Kyphoscoliosis, diaphragmatic palsy |
| Mediastinum | Mediastinitis, thymoma, lymphoma |
III. Aetiological Classification
| Category | Examples |
|---|---|
| Infectious | Pneumonia (bacterial, viral, fungal, TB) |
| Neoplastic | Lung cancer (NSCLC, SCLC), mesothelioma, carcinoid |
| Inflammatory/Autoimmune | Sarcoidosis, vasculitis, RA-ILD, SLE-ILD |
| Occupational/Environmental | Pneumoconioses (silicosis, asbestosis, CWP) |
| Genetic | Cystic fibrosis, alpha-1 antitrypsin deficiency |
| Drug-induced | Amiodarone, bleomycin, methotrexate lung |
| Vascular | Pulmonary embolism, pulmonary hypertension |
| Idiopathic | IPF, cryptogenic organizing pneumonia (COP) |
IV. Acuity Classification
- Acute: Pneumonia, ARDS, pulmonary embolism, acute severe asthma
- Subacute: Hypersensitivity pneumonitis, organizing pneumonia
- Chronic: COPD, IPF, sarcoidosis, bronchiectasis
PFT Summary Table
| Parameter | Obstructive | Restrictive | Mixed |
|---|---|---|---|
| FEV₁ | Decreased | Decreased | Decreased |
| FVC | Normal/decreased | Decreased | Decreased |
| FEV₁/FVC | Decreased (<0.70) | Normal/increased | Decreased |
| TLC | Normal/increased | Decreased | Decreased |
| DLCO | Decreased (emphysema) | Decreased (ILD) | Variable |
- Murray & Nadel's Textbook of Respiratory Medicine, Table 32.1
- The Washington Manual of Medical Therapeutics
Classify restrictive and obstructive lung disease
Obstructive Lung Disease
Classification by Level of Airway Affected
Large Airway Obstruction
| Disease | Key Mechanism |
|---|---|
| Bronchial asthma | Reversible bronchospasm + inflammation |
| Chronic bronchitis | Mucus hypersecretion, airway inflammation |
| Tracheal stenosis | Fixed upper airway narrowing |
Small Airway / Parenchymal Obstruction
| Disease | Key Mechanism |
|---|---|
| Emphysema | Destruction of alveolar walls, loss of elastic recoil |
| Bronchiectasis | Irreversible bronchial dilation, chronic infection |
| Cystic fibrosis | Thick mucus plugging + chronic infection |
| Bronchiolitis | Inflammation of terminal bronchioles |
| Bronchiolitis obliterans | Fibrotic obliteration of small airways |
| Alpha-1 antitrypsin deficiency | Genetic - premature emphysema |
COPD is the umbrella term for chronic bronchitis + emphysema combined.
Restrictive Lung Disease
Classification by Location of the Defect
A. Intrinsic (Parenchymal) - Disease within the lung tissue itself
| Disease | Pattern |
|---|---|
| Idiopathic Pulmonary Fibrosis (IPF) | UIP pattern - worst prognosis |
| Nonspecific Interstitial Pneumonia (NSIP) | Better prognosis than IPF |
| Cryptogenic Organizing Pneumonia (COP) | Steroid-responsive |
| Acute Interstitial Pneumonia (AIP) | Rapidly fatal (>70% mortality at 3 months) |
| Respiratory Bronchiolitis-ILD | Smoking-related |
| Desquamative Interstitial Pneumonia (DIP) | Smoking-related |
- Rheumatoid arthritis (RA-ILD)
- Systemic sclerosis (most common CTD-ILD)
- SLE, polymyositis/dermatomyositis, Sjogren's
- Sarcoidosis
- Hypersensitivity pneumonitis (extrinsic allergic alveolitis)
- Berylliosis
- Silicosis (silica dust)
- Asbestosis (asbestos fibers)
- Coal worker's pneumoconiosis
- Amiodarone, methotrexate, bleomycin, nitrofurantoin
- Radiation pneumonitis/fibrosis
B. Extrinsic (Extra-parenchymal) - Lungs are normal but cannot expand
| Cause | Example |
|---|---|
| Obesity | Reduced diaphragm excursion |
| Kyphoscoliosis | Thoracic cage deformity |
| Ankylosing spondylitis | Fused rigid chest wall |
| Pectus excavatum | Chest wall deformity |
| Cause | Example |
|---|---|
| Upper motor neuron | ALS, spinal cord injury |
| Lower motor neuron | Guillain-Barre syndrome, polio |
| Neuromuscular junction | Myasthenia gravis, botulism |
| Muscle itself | Muscular dystrophy, polymyositis |
| Diaphragm | Diaphragmatic paralysis |
- Pleural effusion (large)
- Fibrothorax / pleural fibrosis
- Pneumothorax (tension)
Side-by-Side Comparison
| Feature | Obstructive | Restrictive |
|---|---|---|
| Problem | Airflow out | Lung expansion |
| FEV₁/FVC | Decreased | Normal/increased |
| FVC | Normal or decreased | Decreased |
| TLC | Normal or increased | Decreased |
| RV | Increased (air trapping) | Decreased |
| DLCO | Decreased (emphysema) | Decreased (ILD) |
| Breath sounds | Wheeze, prolonged expiration | Fine crackles (ILD) |
| CXR | Hyperinflation, flat diaphragm | Small lungs, infiltrates |
| Reversibility | Partial (asthma fully reversible) | Generally progressive |
Difference in rheumatic fever and rhd
difference between acute rheumatic fever and rheumatic heart disease pathogenesis
Rheumatic Fever vs. Rheumatic Heart Disease
Core Distinction
| Acute Rheumatic Fever (ARF) | Rheumatic Heart Disease (RHD) | |
|---|---|---|
| Nature | Acute, self-limiting inflammatory illness | Chronic, progressive structural heart disease |
| Timing | Occurs 2-3 weeks after strep pharyngitis | Develops months to years after ARF |
| Reversibility | Mostly reversible (except cardiac damage) | Irreversible - fibrotic valve deformity |
| Active infection? | Triggered by GAS but no bacteria in lesions | No active infection - immunological scarring |
Aetiology & Pathogenesis
ARF
- Trigger: Group A Streptococcus (GAS) pharyngitis (S. pyogenes)
- Mechanism: Molecular mimicry - antibodies and CD4+ T cells against streptococcal M protein cross-react with cardiac antigens (myocardium, valves, pericardium)
- The 2-3 week delay after infection = time needed to mount this immune response
- Only 0.3-3% of GAS pharyngitis cases develop ARF - genetic susceptibility plays a role
- Tissue injury via: complement activation, neutrophil/macrophage recruitment, T-cell cytokine release
RHD
- Mechanism: Repeated episodes of ARF cause cumulative valve inflammation and healing by fibrosis
- Each attack adds more scarring - even a single severe episode can cause RHD
- Streptococci are completely absent from RHD lesions - it is purely immunological scarring
- Chronic fibrosis is the predictable consequence of repeated healing of acute inflammation
Clinical Features
ARF - Acute, Multisystem Inflammation (lasts 2-4 weeks)
| Feature | Frequency | Details |
|---|---|---|
| Fever | >90% | High grade |
| Polyarthritis | ~75% | Large joints (knees, ankles, wrists), migratory, exquisitely painful, sterile fluid |
| Carditis | >50% | Pancarditis - valvulitis (most important), myocarditis, pericarditis |
| Sydenham's Chorea | ~30% | Involuntary, non-rhythmic movements; "St. Vitus dance"; stops during sleep; unilateral or bilateral |
| Erythema marginatum | <10% | Pink, non-pruritic, blanching, serpiginous rash on trunk and proximal limbs |
| Subcutaneous nodules | <10% | Painless, 0.5-2 cm, over bony prominences/extensor tendons |
RHD - Chronic Valvular Disease (develops years later)
| Feature | Details |
|---|---|
| Mitral stenosis | Most characteristic - virtually the ONLY cause of MS |
| Mitral regurgitation | Most common valve lesion in acute carditis |
| Aortic regurgitation | Second most commonly affected valve |
| Tricuspid disease | Less common; usually with mitral disease |
| Valve morphology | Leaflet thickening, fusion of commissures, chordae shortening/fusion, calcification |
| Symptoms | Dyspnoea, orthopnoea, haemoptysis, AF, systemic emboli, heart failure |
Diagnosis
ARF - Revised Jones Criteria (2015 AHA)
- Carditis (clinical and/or subclinical echocardiographic valvulitis)
- Arthritis (polyarticular in low-risk; mono or polyarticular in high-risk populations)
- Chorea
- Erythema marginatum
- Subcutaneous nodules
- Polyarthralgia (low-risk) / monoarthralgia (high-risk)
- Fever ≥38.5°C
- ESR ≥60 mm/hr and/or CRP ≥3.0 mg/dL (low-risk); ESR ≥30 mm/hr (high-risk)
- Prolonged PR interval on ECG
RHD - Echocardiography
- Valve thickening, restricted mobility, commissural fusion
- Doppler evidence of stenosis/regurgitation
- No specific blood test - diagnosed by imaging and clinical history
Investigations
| Test | ARF | RHD |
|---|---|---|
| Throat culture / ASO titre | Positive (evidence of GAS) | Usually negative (old infection) |
| ESR / CRP | Elevated | Normal (unless in failure) |
| ECG | Prolonged PR interval | AF, LVH, RVH |
| Echocardiogram | Valvulitis (regurgitation) | Stenosis, thickening, calcification |
| CXR | Cardiomegaly (if carditis) | Enlarged chambers, pulmonary congestion |
Treatment
ARF
- Eradicate GAS: Benzathine penicillin G 1.2 million units IM single dose
- Arthritis: Aspirin 80-100 mg/kg/day OR NSAIDs (rapid symptomatic relief)
- Carditis: Corticosteroids for moderate-severe carditis (no proven long-term benefit on valve outcome)
- Chorea: Haloperidol or carbamazepine if severe
- Hospitalization required
RHD
- Secondary prophylaxis (most important - prevents further ARF attacks): Benzathine penicillin G 1.2 million units IM every 4 weeks for minimum 10 years (often lifelong if carditis occurred)
- Symptomatic heart failure: Diuretics, ACE inhibitors, beta-blockers
- AF: Anticoagulation
- Definitive: Balloon mitral valvuloplasty or valve replacement surgery for significant stenosis
Age Profile & Epidemiology
| ARF | RHD | |
|---|---|---|
| Peak age | 5-15 years | 3rd-4th decade |
| Sex | Equal M:F | More common in women |
| Geography | Common in low/middle-income countries | Same distribution; cumulative |
| Global burden | ~33 million cases, ~300,000 deaths/year | Predominantly same populations |
Key Conceptual Summary
ARF is the fire. RHD is the scar left by the fire.
-
ARF = acute, reversible (mostly), multisystem autoimmune response to GAS
-
RHD = chronic, irreversible, cardiac-specific fibrotic sequela of recurrent ARF
-
The mitral valve bears the brunt in both - acute regurgitation in ARF, chronic stenosis in RHD
-
Secondary prophylaxis with penicillin is the single most important intervention to prevent ARF recurrence and thereby halt progression to RHD
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 525-526
-
Goldman-Cecil Medicine, Chapter 269
I remember studiying specific protein affected in valved and joints
rheumatic fever molecular mimicry specific proteins valves joints myosin laminin M protein cross-reactivity
Specific Proteins Targeted in Rheumatic Fever (Molecular Mimicry)
The Core Concept
Streptococcal Antigens That Trigger Cross-Reactivity
| Streptococcal Antigen | Structural Feature |
|---|---|
| M protein | Alpha-helical coiled-coil structure |
| Group A carbohydrate (GlcNAc) | N-acetyl-beta-d-glucosamine dominant epitope |
Tissue-Specific Target Proteins
1. Heart Valves (Valvulitis)
- Anti-GlcNAc antibodies cross-react with laminin (a basement membrane/extracellular matrix protein in valve endothelium)
- This initial antibody-mediated damage to the endocardium causes expression of VCAM-1 (vascular cell adhesion molecule-1) on the valve surface
- VCAM-1 upregulation allows T cells to infiltrate the valve substance
- These T cells cross-react with cardiac myosin (the intracellular biomarker antigen)
- Result: granulomatous inflammation, scarring, neovascularization
| Strep Antigen | Cross-reacts with | Location | Result |
|---|---|---|---|
| GlcNAc / M protein | Laminin | Valve endothelium surface | Endothelial damage, VCAM-1 upregulation |
| M protein | Cardiac myosin | Cardiomyocyte contractile protein | T cell-mediated valve/myocardial inflammation |
| M protein | Tropomyosin | Cardiac muscle (alpha-helical protein) | Further cross-reactive damage |
Autoantibodies against collagen also form secondarily - released from damaged valves, perpetuating the cycle.
2. Joints (Arthritis)
- Mechanism: Immune complex deposition in synovial tissue
- Synovial fluid is sterile with lymphocyte predominance
- The arthritis is transient and non-destructive - unlike valvular disease, joints heal completely
- The specific joint proteins targeted are less well defined compared to cardiac antigens; the damage is primarily from immune complex-mediated inflammation rather than direct molecular mimicry of a single joint protein
3. Brain / Basal Ganglia (Sydenham's Chorea)
| Strep Antigen | Cross-reacts with | Effect |
|---|---|---|
| GlcNAc / M protein | Tubulin | Intracellular biomarker antigen in neurons |
| GlcNAc / M protein | Gangliosides | Neuronal surface antigens |
| GlcNAc / M protein | Dopamine receptors (D1, D2) | Surface target on neuronal cells |
- These antibodies activate calcium/calmodulin-dependent kinase II (CaMKII) in neuronal cells
- CaMKII activation leads to dopamine release - explaining the involuntary movements
- Same antibodies seen in PANDAS (Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal infections)
4. Myocardium (Myocarditis) - Aschoff Bodies
- Anti-M protein antibodies and T cells attack cardiac myosin
- T cells from peripheral blood and heart valves of RHD patients cross-react with both M protein and cardiac myosin
- This forms the Aschoff body - the pathognomonic lesion of rheumatic carditis
- Central fibrinoid necrosis
- Surrounded by Anitschkow cells (plump activated histiocytes with "caterpillar" nuclei)
- Occasional multinucleate giant cells
Summary Table
| Tissue | Strep Antigen | Host Target Protein | Mechanism |
|---|---|---|---|
| Valve endothelium | GlcNAc | Laminin | Antibody-mediated endothelial damage |
| Valve/myocardium | M protein | Cardiac myosin, Tropomyosin | T cell infiltration, Aschoff bodies |
| Myocardium | M protein | Myosin | T cell cytotoxicity |
| Joints | Immune complexes | Synovial tissue (non-specific) | Immune complex deposition |
| Brain (basal ganglia) | GlcNAc / M protein | Tubulin, Gangliosides, Dopamine receptors | CaMKII activation, dopamine release |
-
Valves: Laminin (surface target) + Myosin (intracellular biomarker)
-
Brain: Tubulin (intracellular) + Dopamine receptors (surface target)
-
Structural link: M protein's alpha-helical coil mimics the alpha-helical structure of myosin and tropomyosin - this is why cardiac muscle proteins are preferentially targeted
-
Fuster & Hurst's The Heart, 15th Ed., p. 861
-
Braunwald's Heart Disease, 2 Vol Set
Difference between incidence and prevalence
Incidence vs. Prevalence
Core Distinction
| Incidence | Prevalence | |
|---|---|---|
| What it measures | New cases occurring in a time period | All existing cases at a point in time |
| Question it answers | "How fast is disease developing?" | "How much disease exists right now?" |
| Time element | Always over a period (rate) | Point in time OR period |
| Includes | New cases only | New + old ongoing cases |
Definitions
Incidence
The number of new cases of a disease developing in a population at risk over a specified time period
- Example: 50 new TB cases per 100,000 population per year
Prevalence
The number of all existing cases (new + old) in a population at a given point in time
- Example: 500 diabetics per 100,000 population today
Types
Incidence
| Type | Definition | Example |
|---|---|---|
| Cumulative incidence | Proportion of a fixed group who develop disease over a period | "20% of smokers develop COPD over 10 years" |
| Incidence rate (density) | Cases per person-time (used when follow-up varies) | "5 cases per 1000 person-years" |
Prevalence
| Type | Definition | Example |
|---|---|---|
| Point prevalence | Cases at a single moment in time | "On Jan 1st, 10% of adults had hypertension" |
| Period prevalence | Cases existing at any time during a period | "During 2024, 15% had depression at some point" |
The Relationship Between Them
New cases flowing IN
↓↓↓
┌─────────────────────────┐
│ PREVALENCE POOL │
│ (all existing cases) │
└─────────────────────────┘
↓↓↓
Cases flowing OUT
(cured, died, emigrated)
- Prevalence increases when: incidence rises, disease duration increases (e.g. better treatment keeps patients alive longer)
- Prevalence decreases when: incidence falls, patients recover/die faster
Practical Examples
| Disease | Incidence (new cases/yr) | Prevalence (existing burden) | Why they differ |
|---|---|---|---|
| Flu | High | Low | Short duration - resolves quickly |
| Diabetes | Moderate | Very high | Lifelong condition - accumulates |
| Rabies | Low | Very low | Almost always fatal quickly |
| HIV (pre-ART era) | Moderate | Low | Short survival |
| HIV (post-ART era) | Same/lower | Much higher | ART extends survival dramatically |
HIV/AIDS is the classic exam example: Antiretroviral therapy didn't reduce incidence much, but massively increased prevalence because patients live longer.
Which Measure to Use?
| Use Incidence when | Use Prevalence when |
|---|---|
| Studying causes/risk factors (aetiology) | Planning healthcare resources |
| Evaluating preventive interventions | Estimating disease burden |
| Acute diseases | Chronic diseases |
| Screening programme evaluation | Policy and funding decisions |
Memory Aid
- Incidence = Incoming new cases (the inflow)
- Prevalence = Pool of all cases present (the pond)
Programme management indicators of tb
WHO TB programme management indicators treatment success notification cure rate 2023
RNTCP NTEP TB programme indicators case detection rate treatment success defaulter lost to follow up definitions
https://www.tbdiah.org/wp-content/uploads/2021/10/Navigating…
TB Programme Management Indicators
Framework Overview
INPUT → PROCESS → OUTPUT → OUTCOME → IMPACT
(Resources) (Activities) (Coverage) (Results) (TB burden)
I. Input Indicators
| Indicator | What it measures |
|---|---|
| TB funding | Domestic + international funding availability and gaps |
| Human resources | Number of trained health workers per population |
| Laboratory network | Number of diagnostic labs, GeneXpert machines |
| Drug availability | Uninterrupted supply of first and second-line drugs |
| Guidelines/SOPs | Availability of national TB plans and algorithms |
II. Process Indicators
| Indicator | What it measures |
|---|---|
| GeneXpert utilization rate | % pulmonary TB suspects tested with rapid molecular diagnostics |
| DST coverage | % confirmed TB cases tested for drug resistance |
| HIV testing rate among TB patients | % TB patients with known HIV status |
| Contact tracing coverage | % household contacts of index cases screened |
| TPT (TB preventive therapy) coverage | % eligible contacts/PLHIV started on preventive therapy |
| Private sector engagement | % cases notified from private sector |
| DOTS implementation | % patients on directly observed therapy |
III. Output / Diagnostic Indicators
1. Case Notification Rate (CNR)
- Expressed per 100,000 population per year
- Reflects both disease burden AND programme detection capacity
2. TB Treatment Coverage
- WHO End TB target: ≥90% by 2025
- Reflects the gap between estimated and detected cases
3. Case Detection Rate (CDR) - now called TB Treatment Coverage
- Old terminology still used in many exams
- Formula same as treatment coverage above
- Target: ≥70% under original DOTS targets
4. Bacteriological Confirmation Rate
- Measures quality of diagnosis
- Higher rate = more accurate case-finding
5. Drug-Resistant TB Notification Rate
- Number of confirmed RR-TB/MDR-TB cases notified and started on treatment
- % of confirmed RR-TB patients started on appropriate regimens
IV. Treatment Outcome Indicators
Standard WHO Treatment Outcome Definitions
| Outcome | Definition |
|---|---|
| Cured | Bacteriologically confirmed TB case who was smear/culture negative in the last month of treatment AND on at least one previous occasion |
| Treatment completed | TB case who completed treatment without evidence of failure but no record of smear/culture result in last month (clinically well) |
| Treatment failed | TB case whose sputum smear/culture is positive at month 5 or later during treatment |
| Died | TB case who died for any reason during treatment |
| Lost to follow-up (LTFU) | TB case whose treatment was interrupted for ≥2 consecutive months (previously called "defaulter") |
| Not evaluated | TB case for whom no treatment outcome has been assigned |
Composite Indicators
| Indicator | Formula | WHO Target |
|---|---|---|
| Treatment Success Rate (TSR) | (Cured + Treatment completed) / Total enrolled × 100 | ≥90% by 2025 |
| Lost to follow-up rate | LTFU cases / Total enrolled × 100 | Minimize |
| Case fatality rate | Deaths during treatment / Total enrolled × 100 | Minimize |
| Treatment failure rate | Failed cases / Total enrolled × 100 | <5% |
Current global TSR: ~85% for drug-susceptible TB; ~76% for HIV-associated TB (WHO 2024) India (NTEP) TSR: ~85.5% (2022)
V. Outcome Indicators (Programme-Level)
| Indicator | Definition | Target |
|---|---|---|
| TB incidence rate | New TB cases per 100,000 population/year | Reduce 80% by 2030 vs 2015 baseline |
| TB mortality rate | TB deaths per 100,000 population/year | Reduce 90% by 2030 vs 2015 baseline |
| TB prevalence rate | Existing TB cases per 100,000 population | Reduce 90% by 2030 |
| % TB patients with catastrophic costs | Households facing >20% income loss from TB | Reduce to 0% by 2030 |
VI. Special Population Indicators
| Indicator | Population |
|---|---|
| TB/HIV co-infection rate | % TB patients who are HIV positive |
| ART coverage in TB/HIV | % TB/HIV co-infected patients on ART |
| Childhood TB notification rate | TB cases in 0-14 yr age group |
| MDR-TB treatment success rate | Typically ~60% globally |
VII. RNTCP/NTEP Specific Indicators (India)
| Indicator | Standard |
|---|---|
| Sputum conversion rate (at 2 months) | ≥80% smear positives convert to negative |
| Cure rate | ≥85% for new smear-positive cases |
| Treatment success rate | ≥90% (End TB target) |
| Default/LTFU rate | <5% |
| Annualised Risk of TB Infection (ARTI) | Indicator of transmission in community; target <1% |
| Proportion of TB patients tested for HIV | ≥90% |
Summary: The "3 Key" Programme Indicators for Exams
| Indicator | Formula | Target |
|---|---|---|
| Case Detection Rate | Notified cases / Estimated incident cases × 100 | ≥70% (DOTS) / ≥90% (End TB) |
| Treatment Success Rate | (Cured + Completed) / Registered × 100 | ≥90% |
| Lost to Follow-up Rate | LTFU cases / Registered × 100 | <5% |
A programme is considered successful when CDR ≥70% AND TSR ≥85% are achieved simultaneously - this is because you need both high detection AND high treatment success to actually reduce TB burden in the community.
- WHO Global TB Report 2024
- TB DIAH/USAID Navigating TB Indicators Framework
- NTEP (National TB Elimination Programme), India
Mode of transmission of dengue with incubation period
dengue fever mode of transmission incubation period Aedes aegypti extrinsic intrinsic
Mode of Transmission of Dengue + Incubation Period
The Agent
- Virus: Dengue virus (DENV) - a Flavivirus
- 4 serotypes: DENV-1, DENV-2, DENV-3, DENV-4 (all can cause DHF)
- Each serotype gives lifelong immunity to that serotype only - cross-immunity to other serotypes is temporary (weeks to months)
Mode of Transmission
Primary Mode - Vector-Borne (Biological Transmission)
| Vector | Details |
|---|---|
| Aedes aegypti | Primary vector; domestic, day-biting mosquito; breeds in clean stagnant water (flower pots, tyres, coolers, tanks) |
| Aedes albopictus | Secondary vector ("tiger mosquito"); more widely distributed, harder to control |
How Transmission Occurs - Step by Step
Viraemic human → Mosquito feeds → Virus in mosquito gut
↓
Extrinsic Incubation Period (EIP) in mosquito: 8-12 days
(virus replicates and migrates to salivary glands)
↓
Infective mosquito → Bites susceptible human → Injects virus in saliva
↓
Intrinsic Incubation Period (IIP) in human: 3-14 days
↓
Symptomatic dengue fever
Incubation Periods - The Two Types
| Type | In Whom | Duration | Definition |
|---|---|---|---|
| Intrinsic Incubation Period (IIP) | In the human host | 3-14 days (commonly 5-6 days for classical DF; 4-6 days for DHF) | Time from infective mosquito bite to onset of symptoms in the human |
| Extrinsic Incubation Period (EIP) | In the mosquito vector | 8-12 days | Time from mosquito ingesting viraemic blood to becoming infective (virus must replicate and reach salivary glands) |
Once a mosquito becomes infective after the EIP, it remains infective for life - it can transmit virus with every subsequent bite.
Period of Communicability (Viraemia Window)
| In whom | Duration of infectiousness |
|---|---|
| Infected human | Blood is infective to mosquitoes from 1 day before to 5 days after onset of fever (viraemic period) |
| Infected mosquito | Lifelong, after completion of the EIP |
This is why mosquito control during the first 5 days of illness is critical - the patient is still viraemic and can infect biting mosquitoes.
Other (Non-Vector) Routes
| Route | Details |
|---|---|
| Vertical (transplacental/perinatal) | Mother-to-fetus transmission documented; risk of DHF in neonate |
| Transovarian transmission | Virus passes from infected female mosquito to her eggs - allows virus to persist during dry seasons when no human hosts are available |
| Blood transfusion / organ transplant | Rare, during viraemic phase of donor |
| Needlestick | Rare occupational exposure |
Why Aedes aegypti is Such an Efficient Vector
| Feature | Significance |
|---|---|
| Day-biting (peak dawn and dusk) | Bed nets (used at night) offer little protection |
| Multiple feeds per gonotrophic cycle | Feeds on multiple hosts in one breeding cycle - amplifies transmission |
| Domestic habitat | Lives inside homes, close to humans |
| Breeds in clean water | Hard to control - uses flower pots, overhead tanks, tyres, discarded containers |
| Short flight range (~100 m) | Transmission is highly localized - explains cluster pattern in households |
Summary Box
| Parameter | Value |
|---|---|
| Causative agent | DENV 1-4 (Flavivirus) |
| Primary vector | Aedes aegypti |
| Secondary vector | Aedes albopictus |
| Transmission | Bite of infected female Aedes mosquito |
| Intrinsic IP (human) | 3-14 days (commonly 5-6 days) |
| Extrinsic IP (mosquito) | 8-12 days |
| Human viraemia | 1 day before to 5 days after fever onset |
| Mosquito infectivity | Lifelong after EIP |
| Special routes | Vertical, transovarian, transfusion (rare) |
- Park's Textbook of Preventive and Social Medicine, pp. 289-293
- PLOS ONE: The Incubation Periods of Dengue Viruses (mean IIP 5.9 days, EIP 8-12 days at 25°C)
Which type of fever is dengue
dengue fever type biphasic saddleback fever pattern temperature curve
Type of Fever in Dengue
The Pattern: Biphasic (Saddleback / Camelback) Fever
The Fever Curve - Illustrated
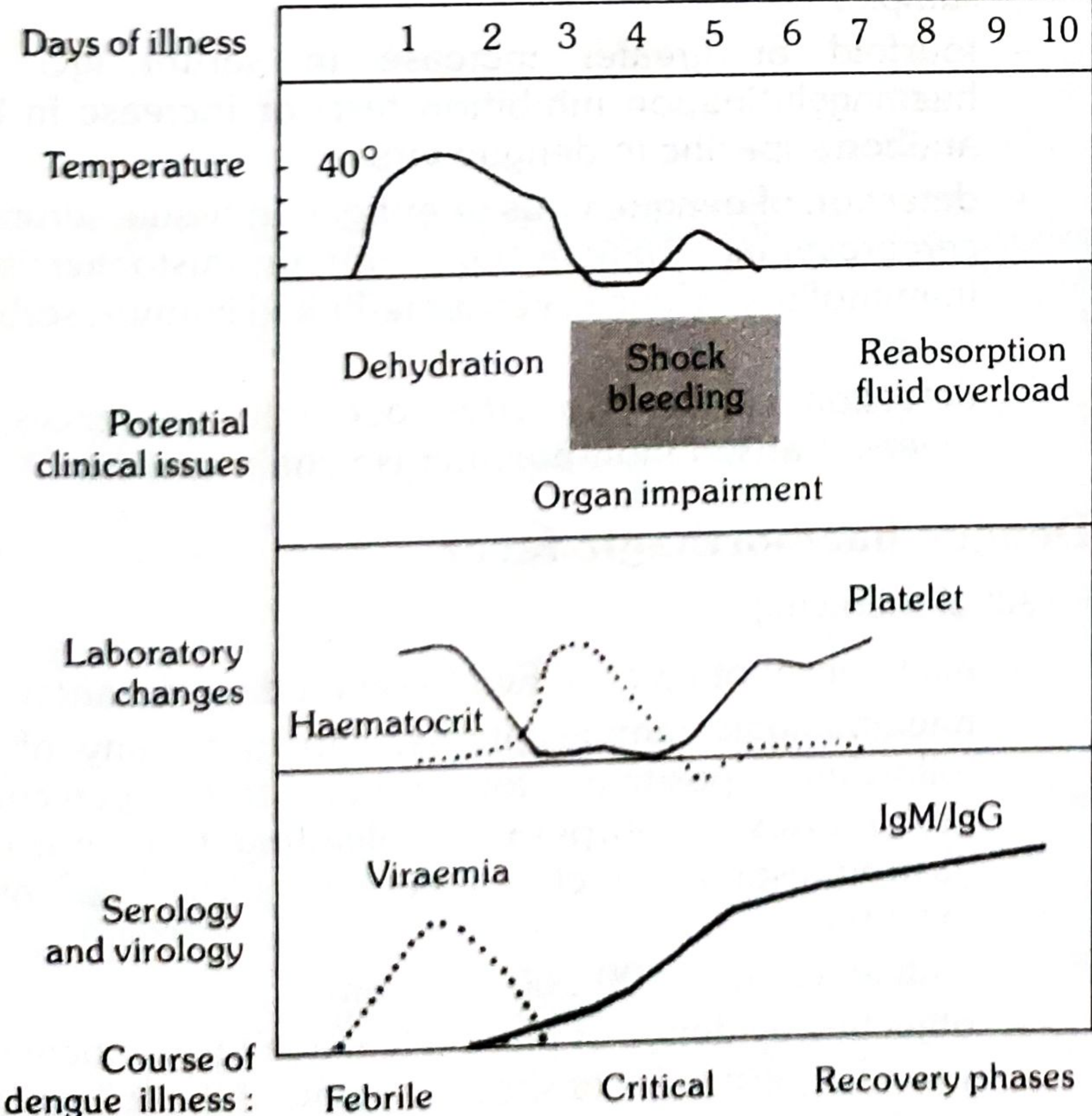
How the Fever Progresses
Phase 1 - First Febrile Spike (Days 1-3)
- Sudden onset of high fever: 39°C-40°C
- Accompanied by chills, severe headache, retro-orbital pain, myalgia, arthralgia ("breakbone fever")
- Flushing of face, neck and chest
- Early rash - diffuse flushing or fleeting pin-point eruptions
Defervescence - Brief Remission (Day 3-4)
- Temperature drops for a few hours to 2 days
- Patient feels temporarily better
- Rash appears in 80% of cases during this remission - characteristic maculopapular/scarlatiniform rash starting on chest and trunk
- In DHF - this is the critical phase - plasma leakage, shock, and bleeding risk peaks here
Phase 2 - Second Febrile Spike (Days 4-5)
- Fever returns but is lower and milder than the first peak
- Lasts 1-2 days
- Accompanied by milder versions of the initial symptoms
- Rash may continue with itching and hyperaesthesia
Recovery Phase (Day 6 onwards)
- Fever resolves, usually within 5-7 days total (rarely >7 days)
- Bradycardia common during recovery
- Platelet count rises, haematocrit normalises
- IgM/IgG antibodies become detectable from ~Day 5 onwards
Fever Classification Summary
| Classification Axis | Dengue Fever Type |
|---|---|
| By pattern | Biphasic (saddleback/camelback) |
| By duration | Acute (5-7 days) |
| By height | High grade (39-41°C) |
| By onset | Sudden/abrupt |
| By cause | Viral (arboviral) |
Why "Breakbone Fever"?
Important Clinical Correlation
-
The defervescence (dip) coincides with plasma leakage beginning in DHF
-
The patient feels better but is actually entering the most dangerous phase
-
Clinicians must not be reassured by the temperature drop - platelet count and haematocrit must be monitored closely between Days 3-6
-
Park's Textbook of Preventive and Social Medicine, pp. 291-293
Which type of fever is dengue fever
Dengue Fever Type = Biphasic (Saddleback/Camelback) Fever
| Classification | Type |
|---|---|
| Pattern | Biphasic / Saddleback / Camelback |
| Height | High grade (39°C - 41°C) |
| Onset | Sudden/abrupt |
| Duration | 5-7 days total |
| Cause | Viral (arboviral - Flavivirus) |
The Two Peaks
Temperature
|
40° | ***
| * * **
|* * * *
| * * *
| ** **
| ** **
| ******
|_________________________ Days
1 2 3 4 5 6 7
[Phase 1] [Dip] [Phase 2]
- Phase 1 (Days 1-3): High fever, headache, myalgia, retro-orbital pain, facial flushing
- Dip (Day 3-4): Brief remission - rash appears in 80% of cases; most dangerous period in DHF (plasma leakage begins)
- Phase 2 (Days 4-5): Milder second fever spike for 1-2 days, then recovery
Also Known As
- "Breakbone fever" - due to the intense bone/joint/muscle pain
- "Three-day fever + two-day fever" - reflecting the biphasic nature
Give me exam oriented classification of hemorrhage
classification of hemorrhage exam surgery pathology types primary reactionary secondary
Classification of Haemorrhage - Exam Oriented
1. By Timing (Surgical Classification) ⭐ Most Asked
| Type | When | Cause | Management |
|---|---|---|---|
| Primary | At the time of injury/surgery | Direct vessel injury, cutting a vessel | Control on the table - suture, ligate, cauterise |
| Reactionary | Within 24-48 hours post-op | Slipped ligature; vessel goes into spasm + hypotension intraop, then BP recovers and bleeding restarts | Return to OT, re-explore, ligate |
| Secondary | 7-14 days post-op (days to weeks) | Deep-seated infection eroding into a vessel wall | Treat infection + haemostasis; often needs re-operation |
Memory: P-R-S = Primary (now), Reactionary (24-48 hrs), Secondary (1-2 weeks/infection)
2. By Source of Vessel
| Type | Character | Clinical Clue |
|---|---|---|
| Arterial | Bright red, spurting, pulsatile | Matches pulse rhythm; high pressure |
| Venous | Dark red, steady ooze/flow | Constant, non-pulsatile; low pressure |
| Capillary | Slow ooze from cut surface | Entire wound surface bleeds; usually self-limiting |
3. By Site / Direction of Bleeding
| Type | Definition | Examples |
|---|---|---|
| External | Blood escapes outside the body | Wound, epistaxis, haematemesis, melaena, haematuria |
| Internal | Blood collects inside body cavities | Haemothorax, haemoperitoneum, haemopericardium |
| Concealed (Revealed vs Concealed) | ||
| - Revealed | Visible externally | Antepartum haemorrhage - placenta praevia |
| - Concealed | Hidden inside (not visible) | Abruptio placentae, ruptured spleen |
4. By Volume / ATLS Classification of Haemorrhagic Shock ⭐ Very High Yield
| Class I | Class II | Class III | Class IV | |
|---|---|---|---|---|
| Blood loss (%) | 0-15% | 15-30% | 30-40% | >40% |
| Blood loss (mL) | Up to 750 mL | 750-1500 mL | 1500-2000 mL | >2000 mL |
| Pulse (bpm) | <100 | >100 | >120 | >140 |
| BP | Normal | Normal | Decreased | Decreased |
| Pulse pressure | Normal | Decreased | Decreased | Decreased |
| RR (breaths/min) | 14-20 | 20-30 | 30-40 | >35 |
| Urine output (mL/hr) | >30 | 20-30 | 5-15 | Negligible |
| CNS/mental status | Slightly anxious | Mildly anxious | Anxious/confused | Confused/lethargic |
| Fluid resuscitation | Crystalloid | Crystalloid | Crystalloid + blood | Crystalloid + blood |
Key: BP does not fall until Class III (>30% blood loss). Pulse pressure falls first (Class II). Urine output is the most sensitive indicator of perfusion.
5. By Pathology / Morphological Types (Robbins/Pathology)
| Type | Size | Definition | Example |
|---|---|---|---|
| Petechiae | 1-2 mm | Pin-point haemorrhages into skin/mucosae | Thrombocytopenia, vasculitis, dengue |
| Purpura | 3-5 mm | Slightly larger than petechiae | ITP, meningococcaemia |
| Ecchymosis | >1 cm | Bruise - subcutaneous haemorrhage | Trauma, coagulopathy |
| Haematoma | Variable | Collection of blood in tissue | Epidural haematoma, retroperitoneal |
| Haemothorax | - | Blood in pleural cavity | Trauma, aortic dissection |
| Haemopericardium | - | Blood in pericardial sac | Cardiac tamponade |
| Haemoperitoneum | - | Blood in peritoneal cavity | Ruptured ectopic, splenic rupture |
| Haemarthrosis | - | Blood in joint space | Haemophilia, trauma |
6. By Cause (Aetiology)
| Category | Examples |
|---|---|
| Traumatic | Wounds, fractures, surgery |
| Spontaneous | Hypertension, aneurysm rupture, AVM |
| Coagulopathic | Haemophilia, DIC, anticoagulant overdose, liver disease |
| Vascular | Vasculitis, scurvy (capillary fragility), HHT |
| Platelet disorders | ITP, thrombocytopenia, aspirin use |
| Neoplastic | Tumour erosion into vessel |
| Infective | Secondary haemorrhage, mycotic aneurysm |
| Obstetric | PPH, abruptio placentae, placenta praevia |
7. Obstetric Classification (PPH) - Special Category
| Type | Timing | Common Cause |
|---|---|---|
| Primary PPH | Within 24 hours of delivery | Atony (4 T's: Tone, Tissue, Trauma, Thrombin) |
| Secondary PPH | 24 hours to 6 weeks after delivery | Retained products of conception, infection |
PPH defined as blood loss >500 mL (vaginal delivery) or >1000 mL (caesarean section)
8. By Intracranial Location (Neurosurgery)
| Type | Location | Classic Feature |
|---|---|---|
| Extradural (EDH) | Between skull and dura | Middle meningeal artery; lucid interval |
| Subdural (SDH) | Between dura and arachnoid | Bridging veins; elderly/alcoholics |
| Subarachnoid (SAH) | In subarachnoid space | "Thunderclap headache"; Berry aneurysm |
| Intracerebral | Within brain parenchyma | Hypertension; basal ganglia |
| Intraventricular | In ventricles | Neonates; severe trauma |
Quick Exam Memory Table
| Classification Axis | Key Points to Remember |
|---|---|
| Timing | Primary / Reactionary (24-48h) / Secondary (7-14d, infection) |
| Vessel | Arterial (bright, pulsatile) / Venous (dark, steady) / Capillary (ooze) |
| Direction | External / Internal; Revealed / Concealed |
| Volume (ATLS) | Class I-IV; BP falls at Class III; urine falls early |
| Morphology | Petechiae < Purpura < Ecchymosis < Haematoma |
| Obstetric | Primary PPH (<24h) / Secondary PPH (24h-6 weeks) |
| Intracranial | EDH / SDH / SAH / ICH |
- Bailey & Love's Short Practice of Surgery, 28th Ed., p. 131
- Sabiston Textbook of Surgery - ATLS Classes of Hemorrhagic Shock, Table 33.1
Pathophysiology of shock in chart form
Pathophysiology of Shock - Chart Form
Core Definition
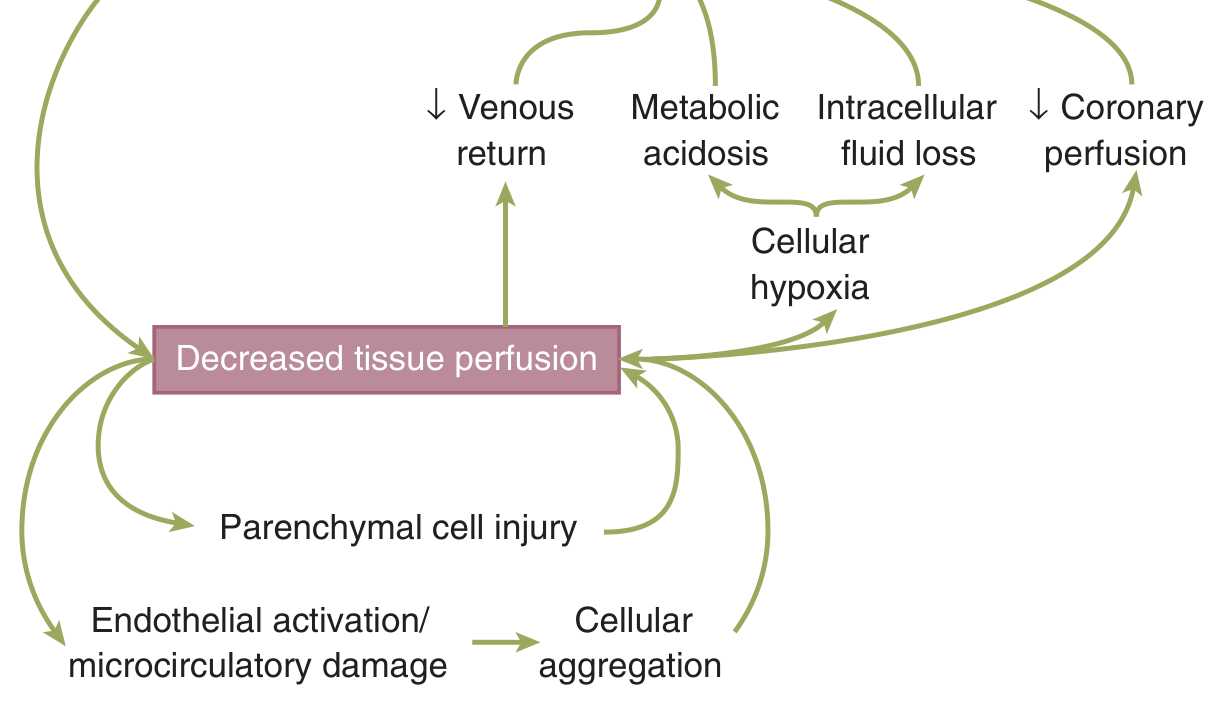
Shock = failure to meet the metabolic needs of the cell Regardless of cause, the final common pathway is decreased tissue perfusion → cellular hypoxia
1. The Vicious Cycle of Shock (from Schwartz's Surgery)
2. Phases of Shock
INCITING EVENT (haemorrhage / sepsis / cardiac failure / neurologic injury)
│
▼
┌─────────────────────────┐
│ DECREASED CO / BP │
│ Tissue hypoperfusion │
└──────────┬──────────────┘
│
┌───────────▼────────────┐
│ COMPENSATED PHASE │ ← Body adapts; BP maintained
│ (Neuroendocrine kick) │ Tachycardia, vasoconstriction,
│ │ oliguria - but BP still normal
└───────────┬────────────┘
│ (if untreated / prolonged)
┌───────────▼────────────┐
│ DECOMPENSATED PHASE │ ← BP falls, acidosis, cell death
│ (Cellular injury) │ Organ dysfunction begins
└───────────┬────────────┘
│ (if further untreated)
┌───────────▼────────────┐
│ IRREVERSIBLE PHASE │ ← Massive parenchymal + microvascular
│ │ damage; resuscitation fails → DEATH
└────────────────────────┘
3. Neuroendocrine Response to Shock (Compensatory Mechanisms)
↓ Blood Volume / ↓ BP
│
├──────────────────────────────────────────┐
▼ ▼
BARORECEPTORS CHEMORECEPTORS
(aortic arch, carotid sinus, (aorta, carotid bodies)
atrial volume receptors) sense ↓O₂, ↑CO₂, ↑H⁺
│ │
└────────────────┬─────────────────────────┘
▼
HYPOTHALAMUS / CNS ACTIVATION
│
┌──────────────┼──────────────┐
▼ ▼ ▼
SYMPATHETIC HPA AXIS ADH (AVP)
ACTIVATION ACTIVATION RELEASE
│ │ │
▼ ▼ ▼
↑Catecholamines ↑Cortisol ↑Water retention
(Epi, Norepi) ↑ACTH by kidneys
│
┌─────┼──────┐
▼ ▼ ▼
↑HR ↑Contractility Vasoconstriction
(skin, gut, kidneys)
│
▼
BLOOD REDISTRIBUTED to
Brain + Heart (vital organs)
- RAAS: ↓Renal perfusion → ↑Renin → ↑Angiotensin II → ↑Aldosterone → Na⁺ + H₂O retention
- ADH/AVP: Released from posterior pituitary → ↑water reabsorption in collecting duct
4. Cellular Pathophysiology
↓ Tissue O₂ Delivery
│
▼
AEROBIC METABOLISM FAILS
│
▼
ANAEROBIC GLYCOLYSIS begins
│
▼
↑ Lactic acid → METABOLIC ACIDOSIS (↓pH)
│
▼
Na⁺-K⁺-ATPase PUMP FAILS (needs ATP)
│
├─────────────────────────────────┐
▼ ▼
Na⁺ + H₂O enter cell K⁺ leaks OUT of cell
CELLULAR OEDEMA HYPERKALAEMIA
│
▼
↑ Intracellular Ca²⁺
(activates proteases, phospholipases)
│
▼
LYSOSOMAL MEMBRANE RUPTURE
│
▼
CELL DEATH (necrosis)
│
▼
INFLAMMATORY MEDIATOR RELEASE
(DAMPs, cytokines, ROS)
│
▼
SYSTEMIC INFLAMMATORY RESPONSE (SIRS)
→ MODS (Multi-Organ Dysfunction Syndrome)
5. Microcirculatory Changes
Initial shock
│
▼
Arteriolar VASOCONSTRICTION (catecholamines)
│
▼
↑ Pre-capillary resistance
│
▼
↓ Capillary hydrostatic pressure
│
▼
Fluid shifts FROM interstitium INTO vasculature
(auto-transfusion / transcapillary refill)
│
▼
Prolonged shock:
│
▼
Endothelial activation + damage
│
├──────────────────────────┐
▼ ▼
↑ Capillary permeability Cellular aggregation
(fluid leaks OUT of vessels) (WBCs, platelets plug
→ oedema, hypovolaemia worsens microcirculation)
│
▼
"No-reflow phenomenon"
(microvascular occlusion persists
even after resuscitation)
6. Organ-Specific Consequences
| Organ | Effect of Shock | Clinical Manifestation |
|---|---|---|
| Kidney | Renal cortex vasoconstriction | Oliguria → ATN → Renal failure |
| Gut | Splanchnic vasoconstriction; mucosal ischaemia | Bacterial translocation → Sepsis |
| Lung | Neutrophil sequestration, capillary leak | ARDS (wet, stiff lungs) |
| Liver | Zone 3 (centrilobular) ischaemia | ↑LFTs, coagulopathy |
| Heart | Subendocardial ischaemia | ↓Contractility → worsens shock |
| Brain | Last to suffer (autoregulated) | Confusion → coma (late sign) |
| Adrenal | ↑Cortisol, catecholamine surge | Compensatory initially |
7. Shock by Type - Haemodynamic Fingerprint
| Parameter | Hypovolaemic | Cardiogenic | Distributive (Septic) | Obstructive | Neurogenic |
|---|---|---|---|---|---|
| CO | ↓ | ↓↓ | ↑ (early) / ↓ (late) | ↓ | ↓ |
| SVR | ↑↑ | ↑↑ | ↓↓ | ↑ | ↓↓ |
| CVP/PCWP | ↓ | ↑↑ | ↓ | ↑ | ↓ |
| Skin | Cold, clammy | Cold, clammy | Warm, flushed (early) | Cold | Warm, dry |
| Cause | Haemorrhage, dehydration | MI, tamponade | Sepsis, anaphylaxis | PE, tension pneumothorax | Spinal cord injury |
Summary Flowchart - One Page
CAUSE
│
▼
↓ Effective Circulating Volume OR ↓ Cardiac Output OR ↓ SVR
│
▼
↓ MEAN ARTERIAL PRESSURE
│
▼
↓ TISSUE PERFUSION (all organs)
│
├── COMPENSATED → ↑HR, ↑SVR, RAAS, ADH → BP maintained
│
├── DECOMPENSATED → ↓BP, Lactic acidosis, Oliguria, Confusion
│
└── IRREVERSIBLE → Cell death, MODS, Death
The gut is the "motor" of MOF - splanchnic ischaemia allows bacterial translocation which drives the systemic inflammatory response that culminates in multi-organ failure.
- Schwartz's Principles of Surgery, 11th Ed., Chapter 5 (pp. 133-152)
Mechanism of labour according to williams
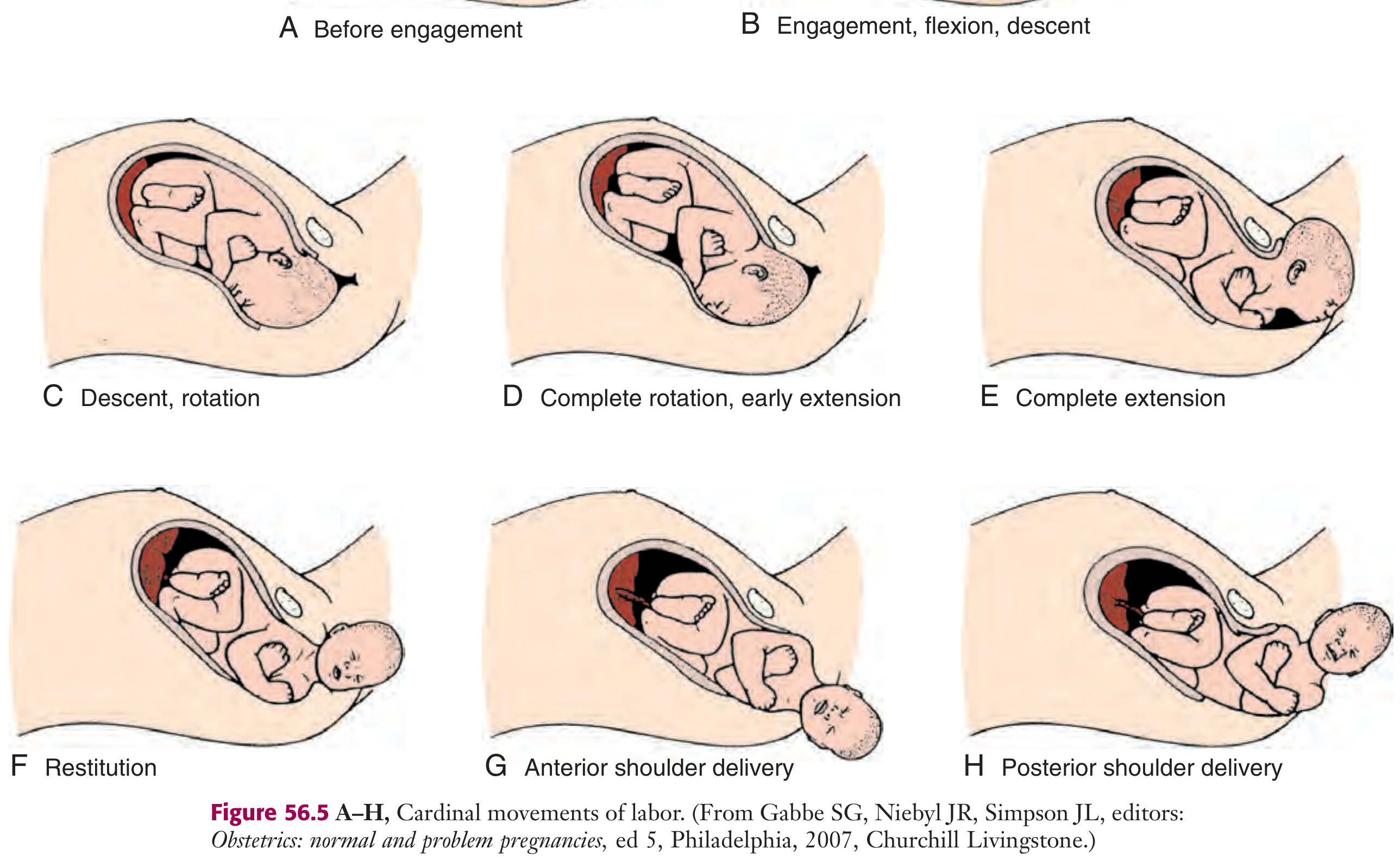
Mechanism of Labour (Cardinal Movements) - According to Williams Obstetrics
Preliminary Concepts
| Term | Definition |
|---|---|
| Lie | Relationship of fetal long axis to maternal long axis (longitudinal / transverse / oblique) |
| Presentation | Part of fetus overlying pelvic inlet (cephalic / breech) |
| Position | Relationship of presenting part to maternal pelvis (e.g. LOA, ROA, OP) |
| Station | Level of presenting part relative to ischial spines (0 = at spines; -ve = above; +ve = below) |
| Engagement | Biparietal diameter (BPD) has passed through pelvic inlet = station 0 |
Most common presentation: Vertex (occiput anterior) in 97% of term pregnancies
The 7 Cardinal Movements of Labour
1. ENGAGEMENT
BPD passes through pelvic inlet
│
▼
Presenting part reaches Station 0
│
Primiparae: 2 weeks before labour (lightening)
Multiparae: at onset of labour
│
Head usually enters in TRANSVERSE diameter of inlet
(Left Occiput Transverse - LOT is most common)
- What engages: Biparietal diameter (BPD) = 9.5 cm
- Denominator: Occiput
- Clinical sign: Fundal height decreases, patient says "baby dropped"
2. FLEXION
Head meets resistance of pelvic floor/walls
│
▼
Chin brought to chest (passive movement)
│
▼
Presenting diameter changes:
Occipito-frontal (11.5 cm) → Sub-occipito-bregmatic (9.5 cm)
- Why it matters: Reduces the presenting diameter by ~2 cm, allowing easier descent
- Mechanism: Lever action - longer occiput arm + shorter face arm → flexion
- Passive movement - driven by uterine contractions and pelvic resistance
3. DESCENT
Downward passage of fetal presenting part through birth canal
│
Forces driving descent:
├── Uterine contractions
├── Abdominal muscle contractions (bearing down)
└── Straightening/extension of fetal body
│
▼
Gradual and progressive (not always continuous)
- Occurs throughout labour but most rapid in 2nd stage
- Assessed by station (-5 to +5 relative to ischial spines)
- Descent occurs simultaneously with all other movements
4. INTERNAL ROTATION
Head in transverse position (LOT/ROT)
│
▼
Occiput rotates ANTERIORLY (45°)
to face symphysis pubis
│
▼
Head now in ANTERO-POSTERIOR diameter of outlet
(Occiput Anterior position)
- Why it occurs: Pelvic floor muscles (levator ani) act like a gutter - sloping anteriorly - and guide the occiput forward
- Normal rotation: 45° from LOT → OA (occiput anterior)
- Abnormal: Rotation to OP (occiput posterior) = "persistent OP" → longer, more painful labour
- Occurs at level of ischial spines as head traverses mid-pelvis
5. EXTENSION
Flexed head reaches pelvic outlet / vaginal introitus
│
▼
Occiput reaches inferior margin of pubic symphysis
│
▼
Head EXTENDS around pubic symphysis (pivot point)
│
▼
Parts delivered in sequence:
Occiput → Bregma → Forehead → Nose → Mouth → Chin
│
▼
Head is born; immediately drops - chin over anus
- Mechanism: Two forces act on the head: uterine contractions push downward; pelvic floor resistance directs anteriorly → resultant force = extension
- Suboccipital region acts as the hypomochlion (fulcrum) against the pubic arch
6. RESTITUTION (External Rotation)
Head delivered; untwists to correct anatomical alignment
│
▼
Occiput rotates back to TRANSVERSE position
(same side it came from - e.g. LOT if was LOA)
│
▼
Now aligns with fetal shoulders
(shoulders are still in oblique diameter of pelvis)
- Passive movement - simple recoil of the neck twist
- Restitution = first 45° rotation back to transverse
- External rotation = further rotation as shoulders undergo internal rotation inside
7. EXPULSION
After external rotation:
Shoulders internally rotate → A-P diameter of outlet
│
▼
ANTERIOR SHOULDER delivered first
(slips under pubic symphysis)
│
▼
POSTERIOR SHOULDER delivered
(passes over perineum)
│
▼
REST OF BODY delivered by lateral flexion
(follows path of least resistance)
Summary Flow Chart
HEAD IN TRANSVERSE (LOT)
↓
ENGAGEMENT
(BPD through inlet, Station 0)
↓
FLEXION
(chin to chest, SOM → SOB diameter)
↓
DESCENT
(downward through birth canal)
↓
INTERNAL ROTATION
(OT → OA, 45° anterior rotation)
↓
EXTENSION
(head pivots under symphysis pubis)
HEAD BORN (occiput → bregma → face → chin)
↓
RESTITUTION / EXTERNAL ROTATION
(head realigns with shoulders)
↓
EXPULSION
(anterior shoulder → posterior shoulder → body)
Diameters Involved - Key Numbers
| Diameter | Measurement | When Relevant |
|---|---|---|
| Sub-occipito-bregmatic (SOB) | 9.5 cm | After full flexion - smallest presenting diameter |
| Sub-occipito-frontal | 10 cm | Partial flexion |
| Occipito-frontal | 11.5 cm | Deflexed head |
| Mento-vertical | 13.5 cm | Brow presentation - cannot deliver vaginally |
| Biparietal (BPD) | 9.5 cm | Engages through pelvic inlet |
| Bi-ischial (outlet) | 11 cm | Transverse diameter of outlet |
Memory Aid
"Every Fetus Deserves Internal Rotation; External Rotation Expels"Engagement → Flexion → Descent → Internal Rotation → (Extension) → External Rotation → Expulsion
- Roberts & Hedges' Clinical Procedures in Emergency Medicine, p. 1351
- Cardinal movements illustrated from Gabbe's Obstetrics: Normal and Problem Pregnancies
Define pem and its complications
protein energy malnutrition PEM definition classification complications kwashiorkor marasmus
Protein-Energy Malnutrition (PEM)
Definition
PEM is a spectrum of clinical conditions resulting from inadequate intake of both protein and calories (macronutrients), leading to impaired growth, wasting of body tissues, impaired immunity, and organ dysfunction.
- Also called Protein-Energy Undernutrition (PEU) by WHO
- Represents a spectrum from mild (subclinical) to extreme forms
- The two extreme poles are Kwashiorkor and Marasmus
Classification of PEM
A. By Aetiology
| Type | Cause |
|---|---|
| Primary PEM | Inadequate dietary intake of protein and/or calories (poverty, food insecurity, famine) |
| Secondary PEM | Underlying disease - malabsorption, malignancy, chronic infection, increased metabolic demand, protein-losing states |
B. By Clinical Syndrome (Most Important for Exams)
| Kwashiorkor | Marasmus | Marasmic-Kwashiorkor | |
|---|---|---|---|
| Deficit | Protein >> Calories | Calories + Protein (both) | Both protein and calories severely |
| Age | After weaning (~1-3 yrs) | Infancy (<1 year) | Any |
| Cause | Carbohydrate-based diet after weaning | Inadequate breast milk/overall starvation | Mixed |
| Weight for age | 60-80% expected | <60% expected | <60% |
| Oedema | Present (cardinal feature) | Absent | Present |
| Muscle wasting | Mild (masked by oedema) | Severe | Severe |
| Subcutaneous fat | Relatively spared | Markedly depleted | Depleted |
| Serum albumin | Low (hypoalbuminaemia) | Near normal or low | Very low |
| Fatty liver | Present | Absent | Present |
| Skin changes | "Flaky paint" (hyper + hypopigmentation, desquamation) | Loose, wrinkled skin | Variable |
| Hair changes | Depigmentation, "flag sign" (alternating bands), easily plucked | Thin, sparse | Variable |
| Appetite | Poor, apathetic | Hungry, alert | Variable |
| Adaptation | Non-adapted (insulin suppresses lipolysis) | Adapted (cortisol, glucagon mobilize fat/protein) | Partial |
C. By Severity (Wellcome Classification)
| Grade | Weight (% of expected) | Oedema |
|---|---|---|
| Underweight | 60-80% | Absent |
| Kwashiorkor | 60-80% | Present |
| Marasmus | <60% | Absent |
| Marasmic-Kwashiorkor | <60% | Present |
D. By WHO/MUAC (Mid-Upper Arm Circumference)
| MUAC | Nutritional Status |
|---|---|
| >13.5 cm | Normal |
| 12.5 - 13.5 cm | Mild-moderate malnutrition |
| <12.5 cm | Severe malnutrition |
Clinical Photographs

Pathophysiology (Why the Two Forms Differ)
KWASHIORKOR MARASMUS
(Protein deficiency > Calories) (All macronutrients deficient)
Carbohydrate intake adequate Severe caloric restriction
↓ ↓
Insulin secreted Cortisol + Glucagon rise
↓ ↓
Lipolysis suppressed Fat + Protein mobilized
Proteolysis suppressed (body adapts)
↓ ↓
Visceral protein ↓↓ Wasting of all compartments
Albumin ↓↓ Albumin relatively spared
↓ ↓
Oedema (↓ oncotic pressure) NO oedema
Fatty liver (↓ lipoprotein carrier) NO fatty liver
Complications of PEM
1. Immune System
- Depressed cell-mediated immunity (T-lymphocyte dysfunction)
- Thymic atrophy and lymphoid depletion
- Impaired complement function
- Increased susceptibility to infections - measles, TB, pneumonia, gastroenteritis
- Secondary infections can be fatal and perpetuate the catabolic state
2. Gastrointestinal
- Villous atrophy of small intestinal mucosa
- Malabsorption - fat, carbohydrate, protein all affected
- Reduced digestive enzyme secretion (lactase deficiency common)
- Bacterial overgrowth
- Impaired gut barrier → bacterial translocation
3. Cardiovascular
- Reduced cardiac muscle mass → reduced cardiac output
- Bradycardia and hypotension
- Susceptibility to cardiac failure during refeeding
4. Liver
- Fatty liver (steatosis) in kwashiorkor - due to reduced VLDL/lipoprotein synthesis
- Impaired drug metabolism
- Reduced coagulation factor synthesis → bleeding tendency
5. Endocrine
- Growth hormone resistance (↑GH but ↓IGF-1)
- Stunted growth - if chronic (height-for-age below -2 SD)
- Hypothyroidism features
- Adrenal and gonadal dysfunction
6. Haematological
- Anaemia - iron, folate, B12 deficiency; also from protein deficiency itself
- Leukopenia
- Thrombocytopenia
7. Neurological / Developmental
- Apathy, listlessness, irritability
- Impaired cognitive development and intellectual capacity
- Permanent neurodevelopmental delay if severe PEM occurs in first 2 years of life ("critical window")
- Peripheral neuropathy
8. Renal
- Reduced GFR and concentrating ability
- Electrolyte imbalances - hypokalaemia, hyponatraemia, hypophosphataemia
9. Refeeding Syndrome (a complication of treatment)
- Rapid refeeding causes sudden shift of phosphate into cells
- Hypophosphataemia → cardiac arrhythmias, respiratory failure, seizures
- Prevention: start feeding slowly, supplement electrolytes
10. Long-term Consequences
- Stunting (chronic malnutrition)
- Obesity and metabolic syndrome in adulthood (Barker hypothesis - fetal programming)
- Reduced adult height and work capacity
- Cognitive deficits and poor school performance
Summary Table - Key Points for Exam
| Feature | Kwashiorkor | Marasmus |
|---|---|---|
| Deficit | Protein > Calories | All macronutrients |
| Age | Post-weaning (1-3 yr) | Infancy (<1 yr) |
| Oedema | YES | No |
| Fatty liver | YES | No |
| Albumin | Low | Near normal |
| Skin | Flaky paint dermatosis | Loose, wrinkled |
| Hair | Flag sign, depigmented | Sparse, thin |
| Behaviour | Apathetic, anorexic | Hungry, alert |
| Adaptation | Non-adapted | Adapted |
| Key complication | Infections, oedema, fatty liver | Infections, cardiac failure |
- Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 412-413
- Lippincott's Illustrated Reviews: Biochemistry, 8th Ed., Table 27.1
- Park's Textbook of Preventive and Social Medicine, p. 737
I have a condition of skin my skin has black patches in my body specially in my legs and hands
black patches skin hands legs causes hyperpigmentation differential diagnosis
Black/Dark Patches on Skin - Possible Causes
⚠️ Important First
- Are the patches flat or raised/rough?
- Are they itchy, painful, or completely symptomless?
- Did they appear suddenly or gradually over months/years?
- Are there any other symptoms - fatigue, weight loss, joint pain?
- Do you have diabetes, thyroid issues, or take any medications?
Common Causes of Black/Dark Patches on Legs and Hands
1. Post-Inflammatory Hyperpigmentation (PIH) - Most Common
- What: Darkening left behind after skin inflammation heals (old insect bites, scratches, eczema, acne)
- Looks like: Flat, dark brown-black patches at sites of old injury
- Common in: Darker skin tones (South Asian, African skin)
- Treatment: Sunscreen, vitamin C, niacinamide, hydroquinone creams
2. Acanthosis Nigricans
- What: Velvety, dark, thickened patches in body folds
- Location: Typically neck, armpits, groin - but also backs of hands and knuckles
- Cause: Insulin resistance, diabetes, obesity, hormonal disorders (PCOS, thyroid)
- Key sign: Texture is rough/velvety, not just a colour change
- Why important: It is a marker of underlying metabolic disease - needs blood sugar testing
3. Venous Stasis / Haemosiderin Deposition (Legs specifically)
- What: Iron deposits from leaking blood vessels stain the skin dark
- Location: Lower legs, ankles especially
- Associated with: Chronic venous insufficiency, varicose veins, leg swelling, standing for long periods
- Other signs: Leg swelling, varicose veins, skin hardening (lipodermatosclerosis)
4. Addison's Disease (Adrenal Insufficiency)
- What: Generalised hyperpigmentation, particularly on pressure areas, skin folds, knuckles, lips, scars
- Cause: Low cortisol → high ACTH → stimulates melanocytes
- Other symptoms: Extreme fatigue, weight loss, low blood pressure, nausea, salt craving
- Important: This needs urgent medical attention if suspected
5. Lichen Planus Pigmentosus
- What: Dark grey-brown patches, especially on sun-exposed areas (face, neck, arms) and flexures
- Common in: South Asians and Middle Easterners
- Associated with: Hepatitis C infection sometimes
6. Diabetic Dermopathy
- What: Round or oval brownish, slightly depressed patches
- Location: Specifically on the shins (lower legs)
- Cause: Small vessel disease in diabetes
- Key: Very common in diabetics, often ignored
7. Sun/UV Damage (Solar Lentigines)
- What: Flat, well-defined dark spots ("age spots", "liver spots")
- Location: Sun-exposed areas - backs of hands, face, forearms
- Cause: Chronic sun exposure → melanocyte proliferation
8. Drug-Induced Pigmentation
- Some medications cause skin darkening: minocycline (antibiotic), amiodarone, hydroxychloroquine, chemotherapy agents, oral contraceptives
9. Tinea Nigra (Fungal)
- What: Black/brown macular patch, usually on palm (rarely sole)
- Cause: Fungal infection (Hortaea werneckii)
- Treatment: Simple antifungal cream
Red Flags - See a Doctor Urgently If:
| Warning Sign | Why Urgent |
|---|---|
| Patch is growing rapidly | Could be melanoma |
| Patch has irregular borders | Melanoma concern |
| Itching, bleeding, or crusting | Active skin disease |
| Associated with fatigue, weight loss | Addison's or systemic disease |
| Leg swelling + dark patches | Venous disease needs treatment |
| Patch feels like thick/rough velvet | Acanthosis nigricans - check blood sugar |
What to Do
- See a dermatologist - they can often diagnose by examination alone
- Take a photo of the patches in good lighting to show progression over time
- Get basic blood tests: fasting blood sugar, HbA1c, thyroid function, cortisol (if fatigue present)
- Avoid self-treating with strong bleaching creams without diagnosis - some contain steroids or mercury which can worsen the skin
I have a condition on my skin it has these dry dark patches on skin all over my body especially on my leg and arms
I have a condition on my skin it has these dry dark patches on skin all over my body especially on my leg and arms Doctor say that it is a genetic condition but i cannot remember the name of disease
ichthyosis genetic dry dark skin patches legs arms types vulgaris X-linked
Ichthyosis - Your Likely Condition
What Does It Look Like?
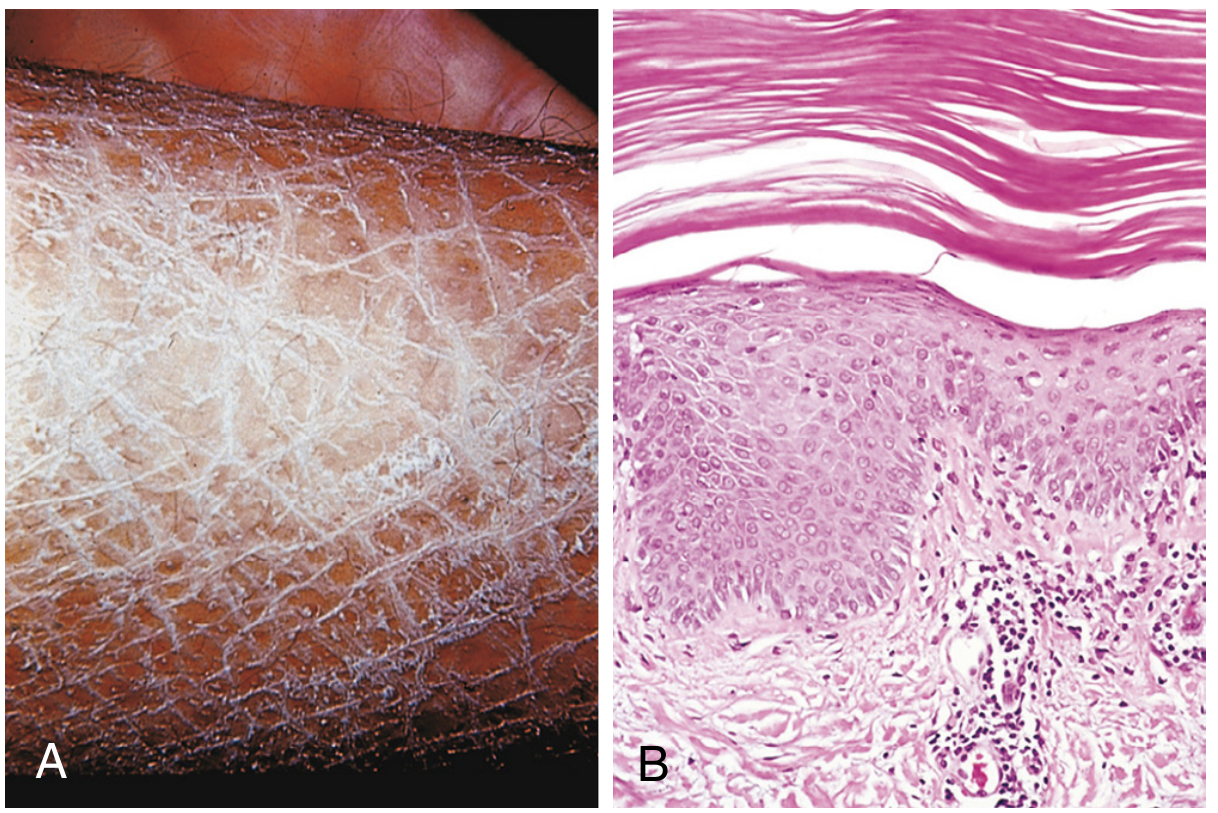
What is Ichthyosis?
Types - Which One Might You Have?
| Type | Inheritance | How Common | Main Features |
|---|---|---|---|
| Ichthyosis Vulgaris | Autosomal dominant (FLG gene) | 1 in 250-1 in 80 - most common | Mild-moderate dry scales; mainly legs, arms, back; flexures (elbows, knees) spared |
| X-linked Ichthyosis | X-linked recessive (STS gene) | Males only | Dark brown scales; trunk, neck, outer arms/legs |
| Lamellar Ichthyosis | Autosomal recessive | Rare | Large, dark, plate-like scales all over body; severe |
| Congenital Ichthyosiform Erythroderma | Autosomal recessive | Rare | Red skin with fine scales from birth |
| Epidermolytic Ichthyosis | Autosomal dominant | Very rare | Blistering + thick scales |
Why Does It Happen? (Simple Explanation)
Gene mutation (FLG / STS gene)
↓
Skin protein (filaggrin / steroid sulfatase) abnormal
↓
Dead skin cells cannot shed properly
↓
They pile up on the surface
↓
Dry, thick, dark, scaly patches
- In Ichthyosis Vulgaris: The filaggrin protein that holds the skin barrier together is defective → skin loses moisture + can't shed dead cells
- In X-linked Ichthyosis: Enzyme steroid sulfatase is missing → dead cells stick together instead of shedding
Key Features That Help Confirm It
- Worst on lower legs (shins) - classic location
- Also outer arms, back, abdomen
- Usually spares armpits, groin (flexures) in vulgaris
- Palms may have extra skin lines (hyperlinear palms)
- Dry, rough, dark or grey-brown scales
- Skin feels like sandpaper or fish scales
- Worse in cold/dry weather, better in summer/humid weather
- No redness or oozing (unless infected)
Management - What You Can Do
Daily Routine
| Step | What to Do |
|---|---|
| Soak | Bath/shower in lukewarm water for 10-15 min to soften scales |
| Exfoliate gently | Use a soft loofah or pumice stone while wet to remove loose scales |
| Moisturise immediately | Apply thick emollient/moisturiser within 3 minutes of getting out - this locks water in |
| Best moisturisers | Urea creams (10-25%), lactic acid lotion, petroleum jelly (Vaseline), ammonium lactate |
| Avoid harsh soaps | Use gentle, fragrance-free soap or soap substitutes |
| Humid environment | Use a humidifier in dry weather/winter |
Medications (prescribed by doctor)
- Retinoids (vitamin A derivatives) - acitretin or isotretinoin for severe cases
- Keratolytics - salicylic acid, alpha-hydroxy acids to help shed scales
- Topical steroid sulfatase replacements being studied for X-linked type
Things That Worsen It
- Cold, dry weather
- Hot showers
- Harsh soaps/detergents
- Not moisturising after bathing
Reassurance
- It is not contagious - no one can catch it from you
- It is not dangerous to your overall health in most forms
- It does not spread to other people
- The skin condition is lifelong but very manageable with consistent skincare
- Associated with atopic eczema and asthma in some cases (ichthyosis vulgaris)
What to Ask Your Doctor
- "Which type of ichthyosis do I have?"
- "Should I have a genetic test?"
- "What moisturiser do you recommend for my skin type?"
- "Are there any triggers I should avoid?"
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 1063
- Fitzpatrick's Dermatology (Ichthyosis Vulgaris section)
Difference between obstructive and restrictive diseases
Obstructive vs. Restrictive Lung Disease
Core Difference in One Line
| Problem | |
|---|---|
| Obstructive | Air cannot get OUT - airways are narrowed |
| Restrictive | Lungs cannot EXPAND - volumes are reduced |
PFT (Spirometry) - The Key Distinguishing Tool
| Parameter | Obstructive | Restrictive |
|---|---|---|
| FEV₁ | ↓↓ | ↓ |
| FVC | Normal or ↓ | ↓↓ |
| FEV₁/FVC ratio | ↓ (<0.70) ← KEY | Normal or ↑ (>0.70) ← KEY |
| TLC | Normal or ↑ (air trapping) | ↓ |
| RV | ↑ (air trapped) | ↓ |
| DLCO | ↓ (emphysema) | ↓ (ILD) |
The FEV₁/FVC ratio is the single most important distinguishing test.
- Low = obstructive
- Normal/high = restrictive
Pathophysiology
| Obstructive | Restrictive | |
|---|---|---|
| Mechanism | Airway narrowing, collapse, or loss of elastic recoil → air traps | Lung stiffness OR chest wall/neuromuscular constraint → cannot expand |
| Where the problem is | Airways (bronchi, bronchioles, alveoli) | Lung parenchyma OR pleura/chest wall/muscles |
| Gas trapping | Yes - TLC increases | No - TLC decreases |
| Breathing effort | Hard to exhale | Hard to inhale |
| Breath sounds | Wheeze, prolonged expiration | Fine end-inspiratory crackles (ILD) |
Examples
Obstructive
| Disease | Key Feature |
|---|---|
| COPD (chronic bronchitis + emphysema) | Smoking; irreversible obstruction |
| Bronchial asthma | Reversible bronchospasm |
| Bronchiectasis | Dilated, infected airways |
| Cystic fibrosis | Thick mucus plugging |
| Alpha-1 antitrypsin deficiency | Genetic; early emphysema |
Restrictive - Intrinsic (parenchymal)
| Disease | Key Feature |
|---|---|
| Idiopathic Pulmonary Fibrosis (IPF) | UIP pattern; worst prognosis |
| Sarcoidosis | Granulomatous; bilateral hilar lymphadenopathy |
| Asbestosis / Silicosis | Occupational exposure |
| Drug-induced (amiodarone, bleomycin) | Medication history |
Restrictive - Extrinsic (extra-parenchymal)
| Disease | Key Feature |
|---|---|
| Obesity, kyphoscoliosis | Chest wall restriction |
| Myasthenia gravis, Guillain-Barré | Neuromuscular; respiratory failure |
| Pleural effusion / fibrothorax | Pleural space disease |
| Diaphragmatic paralysis | Paradoxical breathing |
Clinical Features Compared
| Feature | Obstructive | Restrictive |
|---|---|---|
| Dyspnoea | On exertion; worse on expiration | On exertion; worse on inspiration |
| Cough | Productive (COPD) or dry (asthma) | Dry, non-productive |
| Chest shape | Barrel chest (hyperinflated) | Normal or small chest |
| Percussion | Hyper-resonant | Dull (ILD/effusion) |
| Auscultation | Wheeze, reduced air entry | Fine crackles (Velcro crackles in IPF) |
| CXR | Hyperinflation, flat diaphragm | Small lungs, reticular shadowing |
| Reversibility | Partial (asthma = full; COPD = partial) | Generally irreversible/progressive |
| Cor pulmonale | Late complication | Late complication |
Flow-Volume Loop (Exam Favourite)
Obstructive: Restrictive:
Flow Flow
| *** | ***
| * * | * *
|* *____ | * *
|____________ Volume |_________ Volume
(scooped out expiratory (normal shape but
curve; low peak flow) smaller loop overall)
- Obstructive = scooped/concave expiratory limb, reduced peak expiratory flow
- Restrictive = normal shape but proportionally smaller loop
One-Line Memory Aid
"Obstructive = Out problem (can't breathe out); Restrictive = Room problem (no room to breathe in)"
| FEV₁/FVC | TLC | |
|---|---|---|
| Obstructive | ↓ | ↑ or normal |
| Restrictive | Normal/↑ | ↓ |
| Mixed | ↓ | ↓ |
Difference between obstructive and restrictive diseases
Difference between restrictive and obstructive disease

Solve