Teach me monkey pox in dermatology
Reading File
Finding Sources
Finding Sources
Searching PubMed
monkeypox skin manifestations dermatology
Reading File
Reading File
Reading File
Reading File
Reading Article
PMID: 37106278
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have all the material needed for a thorough, well-illustrated teaching response. Let me compose the full answer.
Monkeypox (Mpox) in Dermatology
Based on Fitzpatrick's Dermatology (Vol. 1-2), Andrews' Diseases of the Skin, and Goldman-Cecil Medicine, supplemented by recent PubMed reviews.
1. Overview and Classification
Monkeypox virus (MPXV) is a member of the Orthopoxvirus genus - the same genus as variola (smallpox), vaccinia, and cowpox. On electron microscopy, it has the characteristic brick shape of all poxviruses. Its genome is 96% identical to variola virus in the central region (which encodes essential enzymes and structural proteins), but the end regions that determine virulence and host range differ substantially - giving monkeypox a much wider host range than variola.
Since the global eradication of smallpox, monkeypox is now the primary Orthopoxvirus causing disease in humans.
Two clades exist:
- Clade I (Central African / Congo Basin clade): More virulent, higher mortality (1-10%), greater human-to-human transmission potential
- Clade II (West African clade): Less virulent, lower mortality, responsible for the 2022 global outbreak (specifically Clade IIb)
2. Epidemiology
- Endemic to the Congo Basin of Central Africa, particularly the Democratic Republic of Congo, Central African Republic, Republic of Congo, and Sudan
- In Africa, the majority of cases are in children under 15, with a fatality rate of ~11% in that group
- Reservoir: Wild African rodents (squirrels of genus Funisciurus and Heliosciurus, giant Gambian rats Cricetomys) and secondarily primates
- Secondary household attack rate: 10-12%
- 2003 US outbreak: 72 cases (37 lab-confirmed) linked to pet prairie dogs co-housed with African rodents imported from Ghana - this demonstrated the first Western Hemisphere cases
- 2022 global outbreak: ~90,000 cases worldwide, >30,000 in the United States; initially concentrated in men who have sex with men (MSM), then spreading to heterosexual contacts and children; caused by Clade IIb
Why is incidence rising? The discontinuation of routine smallpox vaccination programs after 1980 has progressively removed cross-protective immunity in the global population. Prior smallpox vaccination is ~85% protective against monkeypox.
- Fitzpatrick's Dermatology, Vol. 1-2, pp. 3108-3110
3. Transmission
| Route | Details |
|---|---|
| Zoonotic (primary) | Bite/scratch from infected animal, contact with body fluids or carcasses |
| Human-to-human (droplet) | Close contact via respiratory droplets during first week of rash |
| Direct lesion contact | Contact with skin lesions or body fluids |
| Fomites | Rare - contaminated bedding, clothing |
| Sexual transmission | Prominent in 2022 outbreak (anogenital lesions as predominant feature) |
The virus enters through abraded skin, multiplies locally at the entry site, then travels to regional lymph nodes (causing the characteristic lymphadenopathy), then invades the bloodstream - producing viremia and dissemination to distant skin sites.
The longest documented chain of human-to-human transmission is 6 individuals, indicating far lower epidemic potential than smallpox.
4. Clinical Features
Incubation Period
7-17 days (Andrews' Diseases of the Skin cites 10-14 days)
Phase 1: Prodrome (1-4 days)
- Fever, chills, malaise, headache, myalgias, backache (nearly universal - 82-100%)
- Sore throat, cough, shortness of breath
- Diarrhea, abdominal pain (less common)
- Lymphadenopathy - This appears 1-2 days BEFORE the rash and is the single most distinguishing feature from smallpox
Phase 2: Rash (14-21 days to full evolution)
The rash evolves through characteristic stages in a monomorphic pattern (all lesions at same stage simultaneously - key difference from varicella):
Macules → Papules → Vesicles → Pustules → Umbilication → Crusting → Desquamation → Scarring
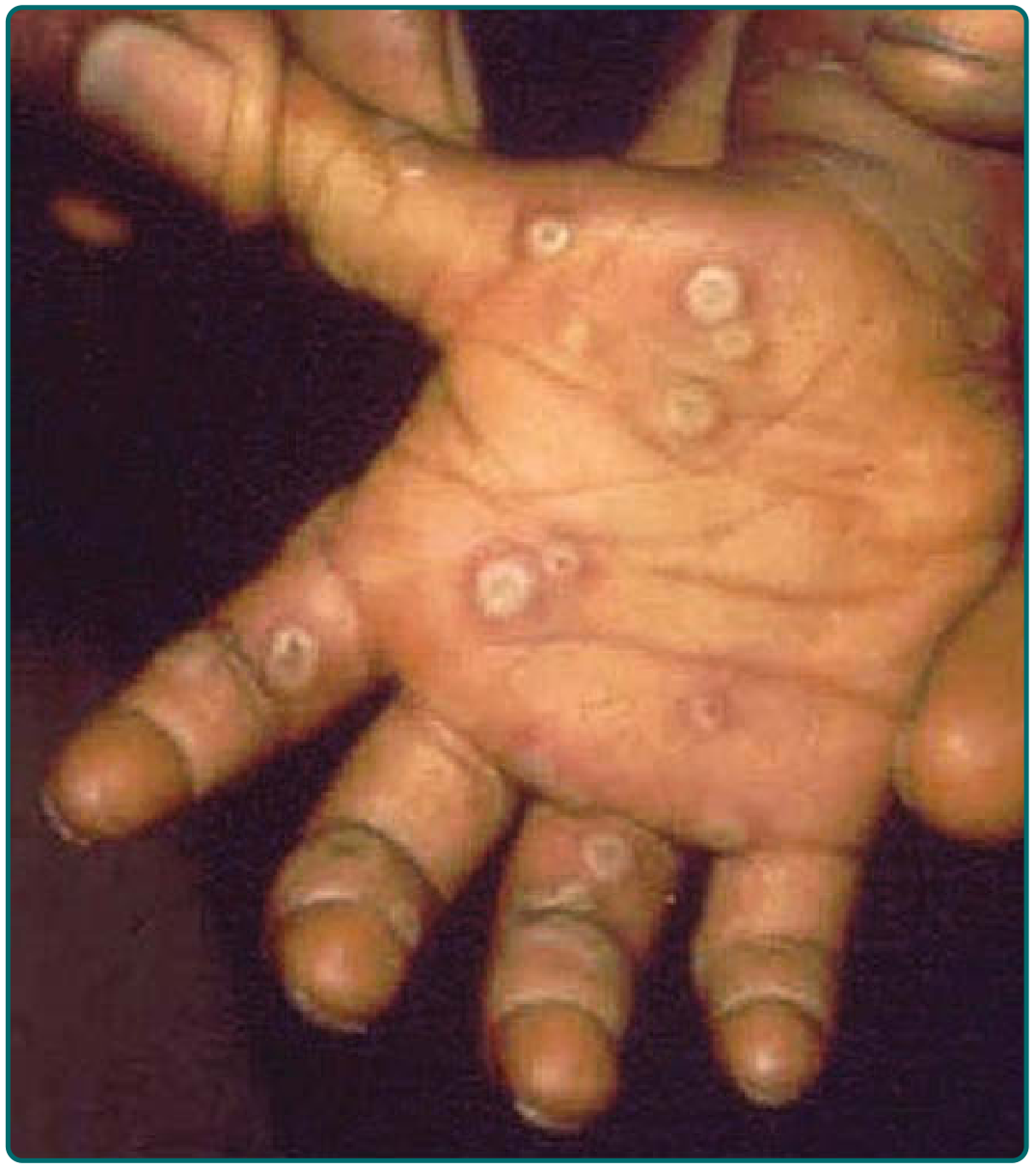
Fig. 166-15 - Umbilicated pustular lesions on the palm. Note the characteristic deep-seated, well-demarcated, umbilicated lesions. (Fitzpatrick's Dermatology)
Distribution:
- Begins on face and/or trunk
- Spreads centrifugally (outward) to become generalized - including palms and soles (also differs from varicella)
- Can involve oral and genital mucous membranes
- In the 2022 outbreak, anogenital lesions were the predominant and sometimes only manifestation
Number of lesions:
- African cases: Generalized (hundreds of lesions), 2-5 mm papules
- US 2003 cases: More localized, mostly on hands at inoculation sites with 1-50 satellite lesions
- 80% of patients have largely monomorphic lesions

Fig. 166-16 - Late desquamative monkeypox lesions on the back of a 5-year-old from the DRC. Note widespread, densely distributed lesions with desquamation. (Fitzpatrick's Dermatology)
Lesion characteristics:
- Deep-seated
- Well-circumscribed
- Umbilicated when pustular
- Heal with dyspigmented and pitted scars
- Hemorrhagic crusts form at resolution
5. Lymphadenopathy - The Hallmark
Lymphadenopathy is the single most clinically important feature distinguishing monkeypox from smallpox and varicella.
- Present in 90% of unvaccinated and 53% of previously vaccinated individuals
- Precedes the rash by 1-2 days
- Typically submandibular, cervical, or inguinal nodes
- Andrews' states: "Lymphadenopathy is not a feature of smallpox"
6. Noncutaneous Findings and Complications
| Finding | Frequency |
|---|---|
| Lymphadenopathy | 90% (unvaccinated) |
| Conjunctivitis and keratitis | Variable |
| Secondary skin/soft-tissue infections | ~20% |
| Pneumonitis | ~12% |
| Encephalitis | <1% |
| Corneal scarring | Rare but important |
African mortality: 1-10%, mainly in children. Death usually occurs in the second week from bacterial superinfection, GI complications, or pulmonary complications - compounded by malnutrition and limited healthcare access.
7. Histopathology
Skin biopsy is NOT specific but shows characteristic poxvirus changes:
- Dermal papillary edema
- Acute inflammation
- Ballooning degeneration of keratinocytes
- Cytoplasmic eosinophilic inclusion bodies (Guarnieri bodies) - pathognomonic of poxvirus infection
- Focal necrosis
These findings are indistinguishable from smallpox histologically. Special confirmatory testing is required.
8. Diagnosis
Laboratory Testing (non-specific markers)
- Leukocytosis (common)
- Elevated transaminases
- Low blood urea nitrogen
- Lymphocytosis and thrombocytopenia (less common)
Confirmatory Testing
| Test | Details |
|---|---|
| PCR (preferred) | Swab of lesion, crust, or fluid - confirms MPXV; can speciate |
| Electron microscopy | Shows brick-shaped poxvirus; cannot distinguish monkeypox from variola or vaccinia |
| Serology | Confirms Orthopoxvirus infection; not species-specific |
| Skin biopsy | Guarnieri bodies; not species-specific |
PCR of lesion material is the gold standard for confirming monkeypox specifically.
9. Differential Diagnosis
| Condition | Key Distinguishing Features |
|---|---|
| Smallpox (variola) | No lymphadenopathy; more severe; centrifugal distribution identical to monkeypox |
| Varicella (chickenpox) | Milder/absent prodrome; centripetal distribution (trunk > extremities); pleomorphic (multiple stages simultaneously); no lymphadenopathy |
| Orf / Bovine stomatitis | Parapoxvirus; more localized lesions; occupational exposure |
| Drug eruptions | Drug history; no viral prodrome |
| Eczema herpeticum | Background atopic dermatitis; HSV positive |
| Rickettsialpox | Eschar at bite site; rickettsia serology |
| Molluscum contagiosum | Immunocompromised patients can develop extensive lesions; no systemic features |
| Syphilis (secondary) | Maculopapular rash on palms/soles; VDRL/RPR positive; no vesiculation |
The key clinical triad pointing to monkeypox: Prodrome + lymphadenopathy preceding rash + monomorphic centrifugal vesiculopustular rash progressing to umbilicated lesions.
10. Monkeypox vs. Smallpox vs. Varicella - Comparison Table
| Feature | Monkeypox | Smallpox | Varicella |
|---|---|---|---|
| Lymphadenopathy | Yes (90%) | No | No |
| Distribution | Centrifugal | Centrifugal | Centripetal |
| Lesion morphology | Monomorphic | Monomorphic | Pleomorphic |
| Palms/soles involved | Yes | Yes | Rarely |
| Oral mucosa | Yes | Yes | Yes |
| Prodrome severity | Moderate | Severe | Mild/none |
| Mortality (unvaccinated) | 1-10% | 30% | <0.01% |
| Contagiousness | Moderate | High | Very high |
11. Management
Infection Control
- Contact and droplet precautions
- Negative-pressure room isolation if possible
- Healthcare workers at higher risk from contaminated fomites (examination tables, gowns, gloves)
Antiviral Treatment
| Drug | Notes |
|---|---|
| Tecovirimat (TPOXX) | First-line for severe disease; VP37 envelope protein inhibitor; maintained in US Strategic National Stockpile; used under IND protocol; reduces severity even when given after symptom onset |
| Cidofovir | DNA polymerase inhibitor; nephrotoxic |
| Brincidofovir | Oral prodrug of cidofovir; less nephrotoxic |
All three are approved for smallpox and used off-label for monkeypox - efficacy in humans remains uncertain but animal models are promising.
Most cases are self-limiting and require only supportive care.
Post-Exposure Prophylaxis (PEP)
- Preferred: Vaccinia (smallpox) vaccine within 4 days of exposure (consider up to 14 days)
- PEP applies even to: infants <12 months, pregnant women, those with skin conditions
- Contraindicated in severe T-cell immunodeficiency (risk from vaccination may equal or exceed risk from monkeypox in this group)
12. Vaccination
| Vaccine | Details |
|---|---|
| JYNNEOS (Imvamune/Imvanex) | Live attenuated, non-replicating modified vaccinia Ankara (MVA); specifically approved for monkeypox; 2 doses; safer profile; can be used for both pre- and post-exposure prophylaxis |
| ACAM2000 | Live replicating vaccinia; effective but more adverse effects (myocarditis, eczema vaccinatum risk); second-line |
| Dryvax (historical) | 85% protective in African studies |
Pre-exposure indications: Laboratory workers, monkeypox investigators, healthcare workers caring for monkeypox patients.
Global eradication of monkeypox is more difficult than smallpox eradication because of the wide range of animal reservoir hosts.
13. 2022 Outbreak - Clinical Shift (Clade IIb)
The 2022 global outbreak introduced important clinical differences relevant to dermatologists:
-
Anogenital skin lesions as the predominant feature - often the only manifestation
-
Rash limited to 1-5 lesions in some cases (not the classic widespread eruption)
-
Painful lesions (rectal pain, dysuria prominent)
-
Transmitted primarily through close sexual contact in MSM initially
-
Less prominent systemic prodrome before rash in some cases
-
Same vaccine and treatment strategies apply
-
Gupta AK et al., Am J Clin Dermatol 2023 [PMID: 37106278]
Summary Mnemonic: MONKEYPOX
| Letter | Key point |
|---|---|
| M | Monomorphic lesions (all at same stage) |
| O | Orthopoxvirus (brick-shaped on EM) |
| N | No smallpox vaccine immunity in today's population |
| K | Key sign = Lymphadenopathy (before rash) |
| E | Endemic - Congo Basin |
| Y | JYNNEOS vaccine for prevention |
| P | Prodrome: fever, chills, myalgias, backache |
| O | Oropharyngeal and anogenital mucosa involved |
| X | X-clude variola: lymphadenopathy differentiates |
Sources: Fitzpatrick's Dermatology Vol. 1-2, pp. 3108-3112; Andrews' Diseases of the Skin, p. 369; Goldman-Cecil Medicine, p. 3587; Gupta et al. Am J Clin Dermatol 2023 [PMID: 37106278]
This is a shared conversation. Sign in to Orris to start your own chat.