Thyroid strom
Reading File
Finding Sources
Searching PubMed
"thyroid storm" management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information to write a detailed response. Let me compile everything.
Thyroid Storm (Thyrotoxic Crisis)
Definition
Thyroid storm is a rare, life-threatening form of severe thyrotoxicosis with multiorgan dysfunction. Untreated, mortality approaches 100%; with prompt treatment, it is still 10-30%. It most often occurs as an acute reaction to a precipitant in a patient with pre-existing, often unrecognized or undertreated hyperthyroidism.
Pathophysiology
The exact mechanism underlying the shift from simple thyrotoxicosis to thyroid storm is not fully understood, but it involves adrenergic hyperactivity - either by increased release of thyroid hormones or increased adrenergic receptor sensitivity. Patients in thyroid storm have relatively higher levels of free (unbound) thyroid hormones compared to uncomplicated hyperthyroidism.
- Excess T4/T3 enter cells, where T4 is converted to active T3
- T3 passes into the nucleus, binds thyroid hormone receptors, and drives gene transcription
- Precipitants (infection, trauma, MI) amplify this by freeing hormones from binding proteins or increasing receptor sensitivity
- TSH is suppressed via negative feedback on the pituitary
Precipitating Events
| Systemic | Cardiovascular | Obstetric | Drug/Hormone |
|---|---|---|---|
| Infection | Myocardial infarction | Labor and delivery | Withdrawal of antithyroid meds |
| Trauma | CVA/stroke | Eclampsia | Iodine load |
| Surgery | Pulmonary embolism | Hyperemesis gravidarum | Radioactive iodine therapy |
| DKA | Preeclampsia | Thyroid hormone ingestion | |
| Hyperosmolar coma | Thyroid gland palpation |
Unknown cause in up to 25% of cases.
Clinical Features
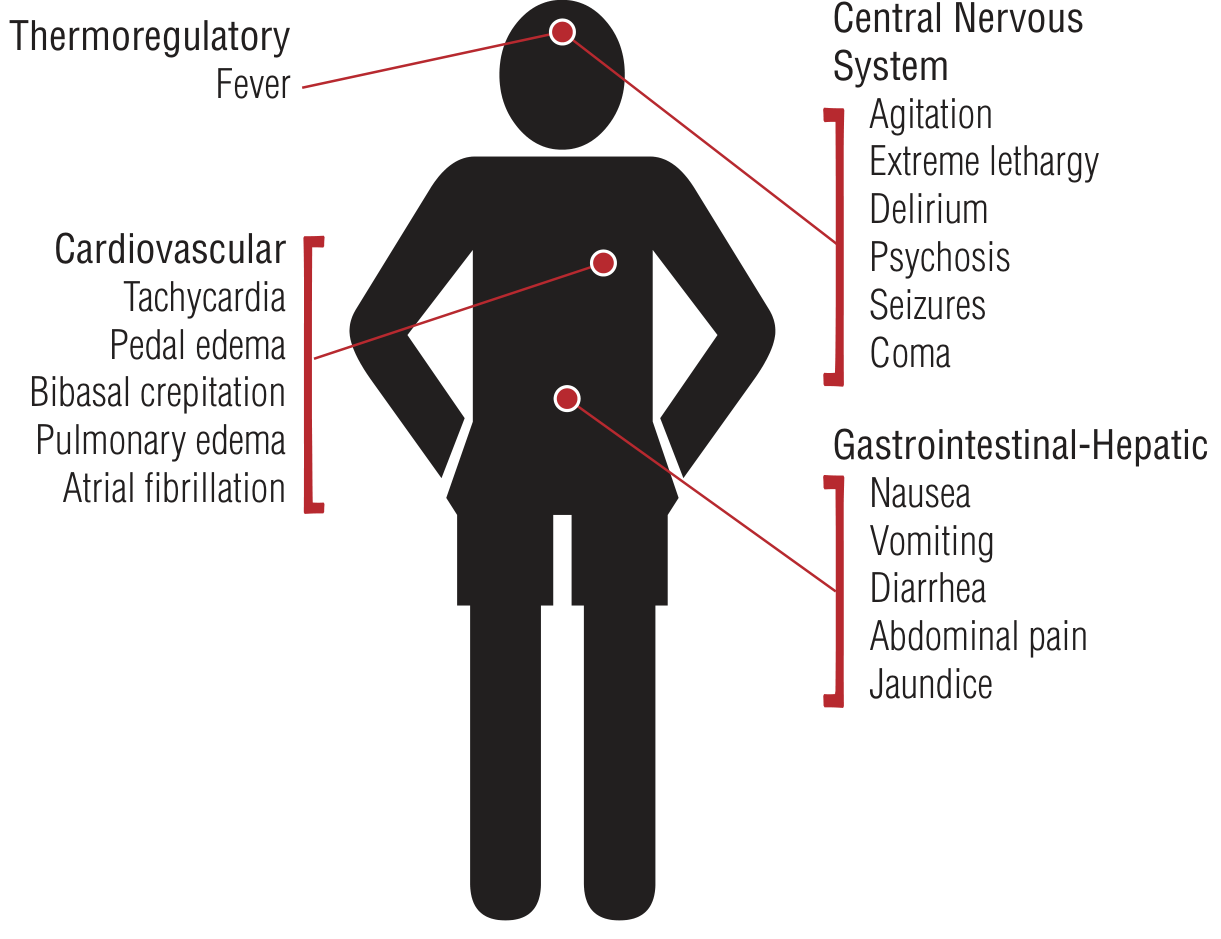
Figure: Clinical features of thyroid storm (Tintinalli's Emergency Medicine)
| System | Features |
|---|---|
| Thermoregulatory | Hyperpyrexia 104-106°F (40-41°C) |
| Cardiovascular | Extreme tachycardia (often disproportionate to fever), atrial fibrillation, heart failure, hypotension, cardiovascular collapse; Takotsubo cardiomyopathy can occur |
| CNS | Agitation, delirium, psychosis, extreme lethargy, seizures, coma |
| GI-Hepatic | Nausea, vomiting, diarrhea, abdominal pain; jaundice (hepatic failure - rare but poor prognosis) |
| Signs of hyperthyroidism | Goiter, exophthalmos, lid lag, tremor, warm/moist skin |
Diagnosis - Burch-Wartofsky Score
Thyroid storm is a clinical diagnosis - do not wait for labs. The Burch-Wartofsky scoring system (1993) helps distinguish thyrotoxicosis, impending storm, and frank storm:
| Category | Finding | Points |
|---|---|---|
| Fever (°F) | 99-99.9 | 5 |
| 100-100.9 | 10 | |
| 101-101.9 | 15 | |
| 102-102.9 | 20 | |
| 103-103.9 | 25 | |
| ≥104 | 30 | |
| Heart rate (bpm) | 90-109 | 5 |
| 110-119 | 10 | |
| 120-129 | 15 | |
| 130-139 | 20 | |
| ≥140 | 25 | |
| Mental status | Normal | 0 |
| Mild agitation | 10 | |
| Delirium/psychosis/extreme lethargy | 20 | |
| Coma/seizures | 30 | |
| CHF | Absent | 0 |
| Mild (edema) | 5 | |
| Moderate (rales) | 10 | |
| Pulmonary edema | 15 | |
| Atrial fibrillation | Present | 10 |
| GI-hepatic | None | 0 |
| N/V | 10 | |
| Diarrhea/abdominal pain | 20 | |
| Unexplained jaundice | 20 | |
| Precipitating event | Present | 10 |
- ≥45: Thyroid storm - treat immediately
- 25-44: Impending storm - treat aggressively
- <25: Unlikely to be thyroid storm
Labs
- TSH: depressed or undetectable (<0.01 μU/mL on 3rd-gen assay) - most sensitive test
- Free T4 and Free T3: elevated
- Note: Lab results should NOT delay treatment
Treatment
The order of medication is critical. Iodine given before thionamides can precipitate worsening storm - always give thionamides at least 1 hour before iodine.
Order of Treatment
Step 1 - Beta Blockade (immediate)
- Propranolol is first choice - it both blocks adrenergic effects AND inhibits peripheral conversion of T4 to T3
- Oral: 60-80 mg every 4-6 hours
- IV: 1-2 mg slowly every 5-10 min (max 10 mg), or infusion
- Esmolol (IV): 50-100 mcg/kg/min - preferred when rapid titration is needed, or in asthma/COPD
- Metoprolol can be used in asthma (beta-1 selective)
- If beta blockers are contraindicated (severe HF, asthma): use diltiazem 90-120 mg PO TID-QID, or IV 5-10 mg/h; or reserpine 2.5-5 mg IM q4h
- Avoid aspirin - it displaces T4/T3 from binding proteins, worsening thyrotoxicosis
Step 2 - Thionamides (block new hormone synthesis)
- PTU (Propylthiouracil) is preferred over methimazole in thyroid storm because it also blocks T4→T3 conversion
- Loading dose: 500-1000 mg PO, then 250 mg every 4-6 hours
- If unable to swallow: rectal preparation, 400 mg every 6 hours as retention enema
- Methimazole: 20-30 mg PO every 8 hours; rectal preparation 60-80 mg/day if needed
Step 3 - Iodine (>1 hour after thionamides - blocks hormone release via Wolff-Chaikoff effect)
- SSKI (Saturated Solution of Potassium Iodide): 5 drops PO every 6 hours
- Lugol's solution: 8-10 drops every 6 hours
- Lithium carbonate: alternative if iodine is contraindicated
Step 4 - Glucocorticoids (block T4→T3 conversion, prevent relative adrenal insufficiency)
- Hydrocortisone: 100-300 mg IV loading, then 100 mg IV every 8 hours
- Dexamethasone: 2-4 mg IV every 6 hours (also blocks peripheral conversion)
Step 5 - Supportive Care
- Cooling: blankets, fans, ice packs, gastric/bladder lavage
- Acetaminophen for fever (NOT aspirin - see above)
- IV fluids: D5/0.9%NS to replenish glycogen and volume losses
- Electrolyte replacement
- Benzodiazepines for agitation (also reduce central sympathetic outflow)
- Treat precipitating cause (empirical antibiotics if infection suspected)
- ICU monitoring
Refractory/Severe Cases
- Cholestyramine 1-4 g PO BID - blocks enterohepatic recirculation of thyroid hormones
- Plasmapheresis/plasma exchange - rapidly lowers circulating hormone levels
- Peritoneal dialysis (rarely used)
Causes of Death
- Congestive heart failure
- Cardiac arrhythmias
- Respiratory failure
- Multiorgan dysfunction
- DIC (disseminated intravascular coagulation)
- Hypoxic brain injury
- Sepsis
Differential Diagnoses
- Sympathomimetic intoxication
- Anticholinergic crisis
- Alcohol/sedative withdrawal
- Neuroleptic malignant syndrome
- Serotonin syndrome
- Heat stroke
- Meningitis / sepsis
- Manic episode / panic attack (especially if apathetic presentation in elderly)
Sources: Rosen's Emergency Medicine 9e, Tintinalli's Emergency Medicine, Katzung's Basic & Clinical Pharmacology 16e, Braunwald's Heart Disease, Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.