GLIOMA
Reading File
Finding Sources
Finding Sources
Searching PubMed
"glioma"[MeSH Terms] AND "classification"[MeSH Terms]
Reading File
Reading File
Searching PubMed
"glioma" AND "treatment"
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information to write a thorough, authoritative response on glioma. Let me compile everything.
Glioma: A Comprehensive Overview
Gliomas are intrinsic brain tumors of glial cell origin and are the most common type of malignant primary brain tumor. The 2021 WHO Classification of CNS Tumours fundamentally restructured how gliomas are classified, now using molecular genetic markers alongside histology.
1. Classification (2021 WHO)
The 2021 WHO Classification divides gliomas into adult-type and pediatric-type based on molecular differences. Within each category, tumors are further graded by histologic and molecular features.
Adult-Type Diffuse Gliomas
Classification is driven first by IDH mutation status, then by 1p/19q co-deletion:
| Entity | IDH | 1p/19q | WHO Grade |
|---|---|---|---|
| Astrocytoma, IDH-mutant | Mutant | Intact | 2, 3, or 4 |
| Oligodendroglioma, IDH-mutant and 1p/19q co-deleted | Mutant | Co-deleted | 2 or 3 |
| Glioblastoma, IDH-wildtype | Wild-type | N/A | 4 |
Harrison's Principles of Internal Medicine 22E (2025)
2. Epidemiology
- Low-grade glioma (WHO grade 2): Peak incidence in the 4th decade; often presents with seizures
- High-grade glioma (WHO grades 3-4): Peak incidence in the 5th-6th decades; typically presents de novo or by transformation from lower-grade tumors
- Glioblastoma: Most common malignant primary brain tumor; >12,000 new cases/year in the US; presents in the 6th-7th decades
- Bailey and Love's Short Practice of Surgery, 28th Ed.
3. Clinical Presentation
- Seizures - hallmark of low-grade glioma, especially temporal/frontal location
- Headache - from raised intracranial pressure
- Focal neurologic deficits - depending on location
- Cognitive decline - especially diffusely infiltrative tumors (formerly "gliomatosis cerebri")
4. Imaging
MRI with and without contrast is the preferred modality. CT of chest/abdomen/pelvis is added to exclude extracranial primary (metastasis is the main differential).
CT contrast scan showing heterogeneous right frontoparietal glioblastoma with mass effect and midline shift:
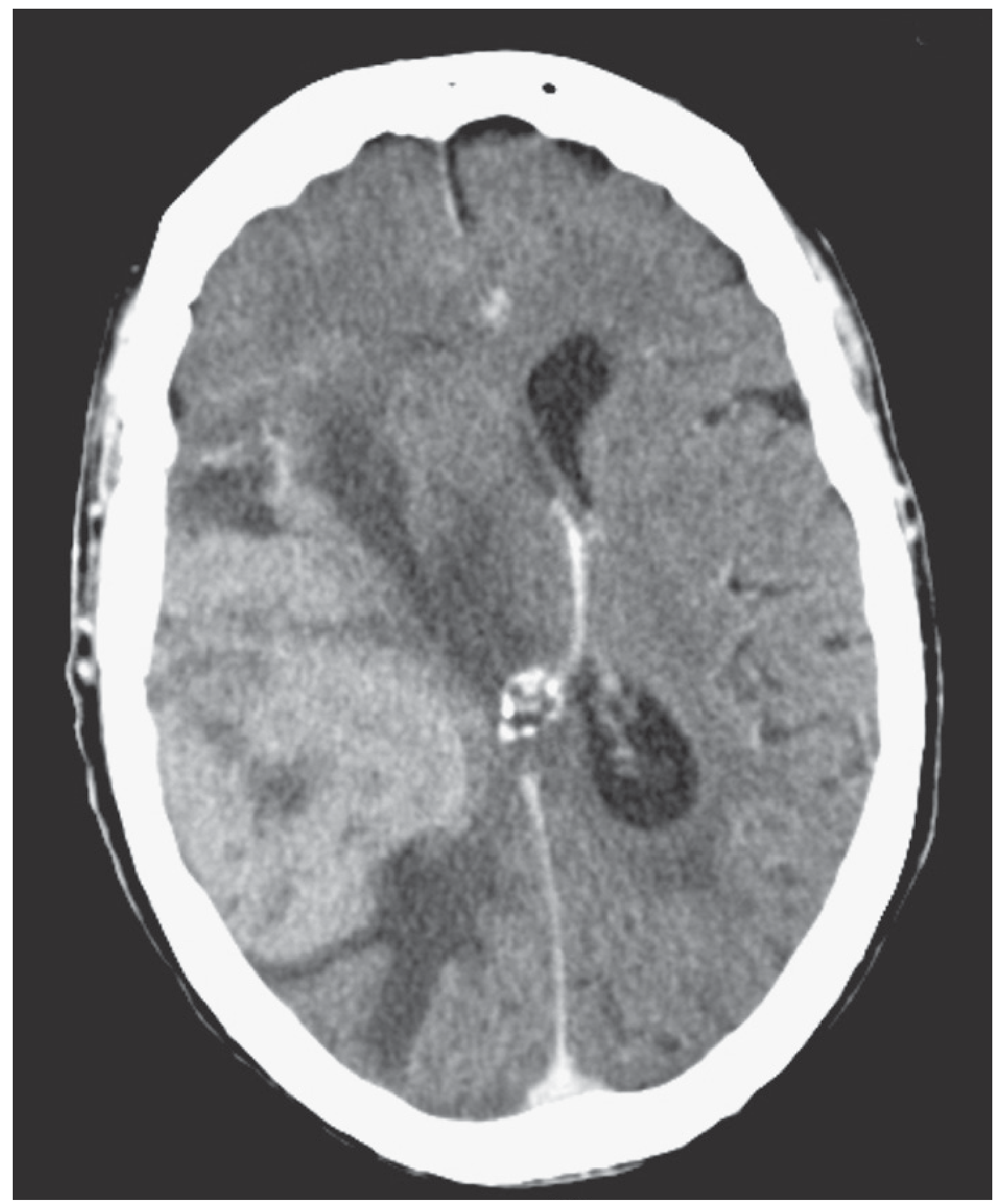
Figure: CT with contrast - heterogeneous right frontoparietal lesion consistent with glioblastoma. (Bailey & Love)
FLAIR MRI of a low-grade astrocytoma (non-enhancing):
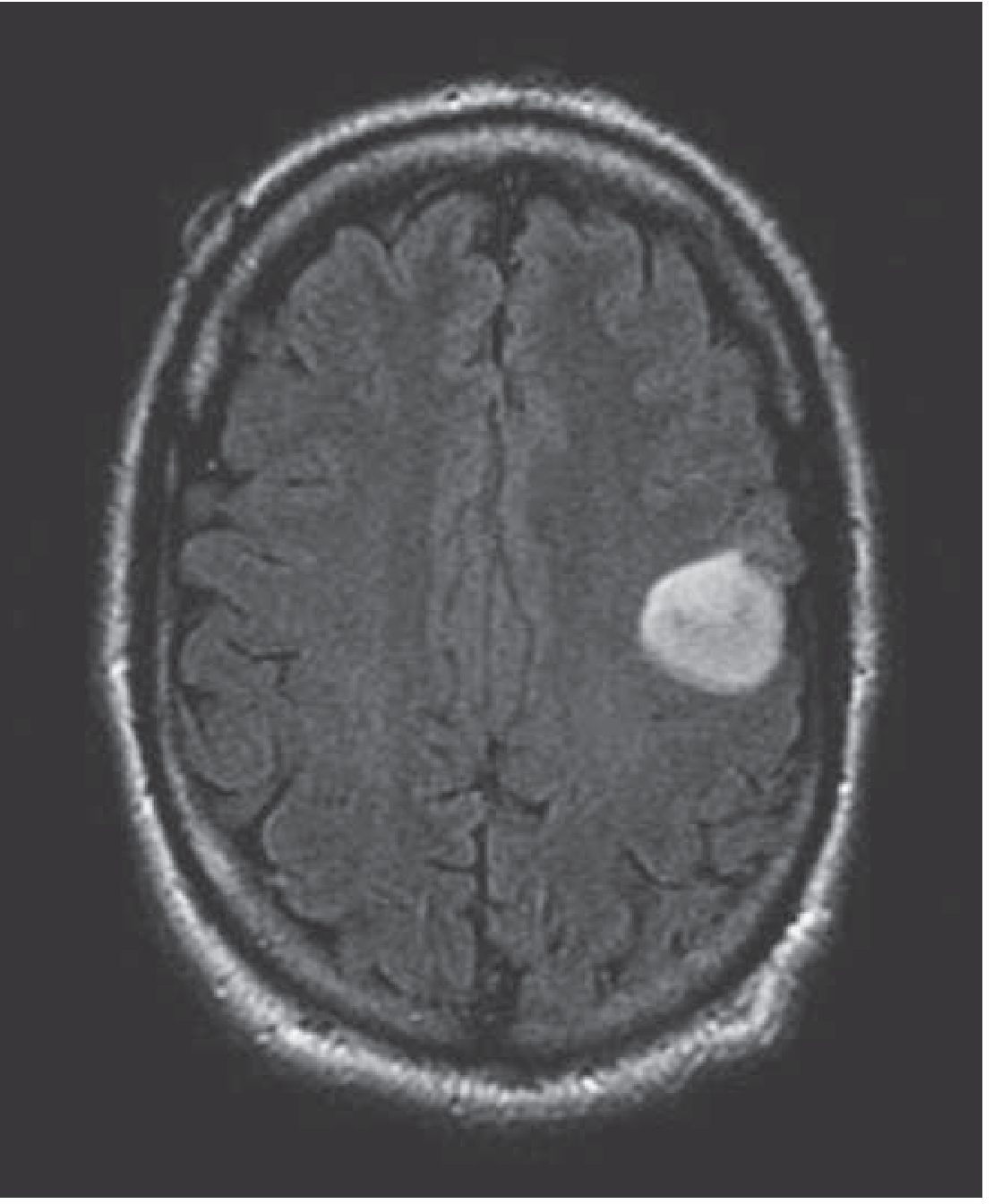
Figure 95-1: FLAIR MRI showing left frontal low-grade astrocytoma - non-enhancing T2/FLAIR hyperintensity. (Harrison's 22E)
Post-gadolinium T1 MRI of a large cystic glioblastoma:
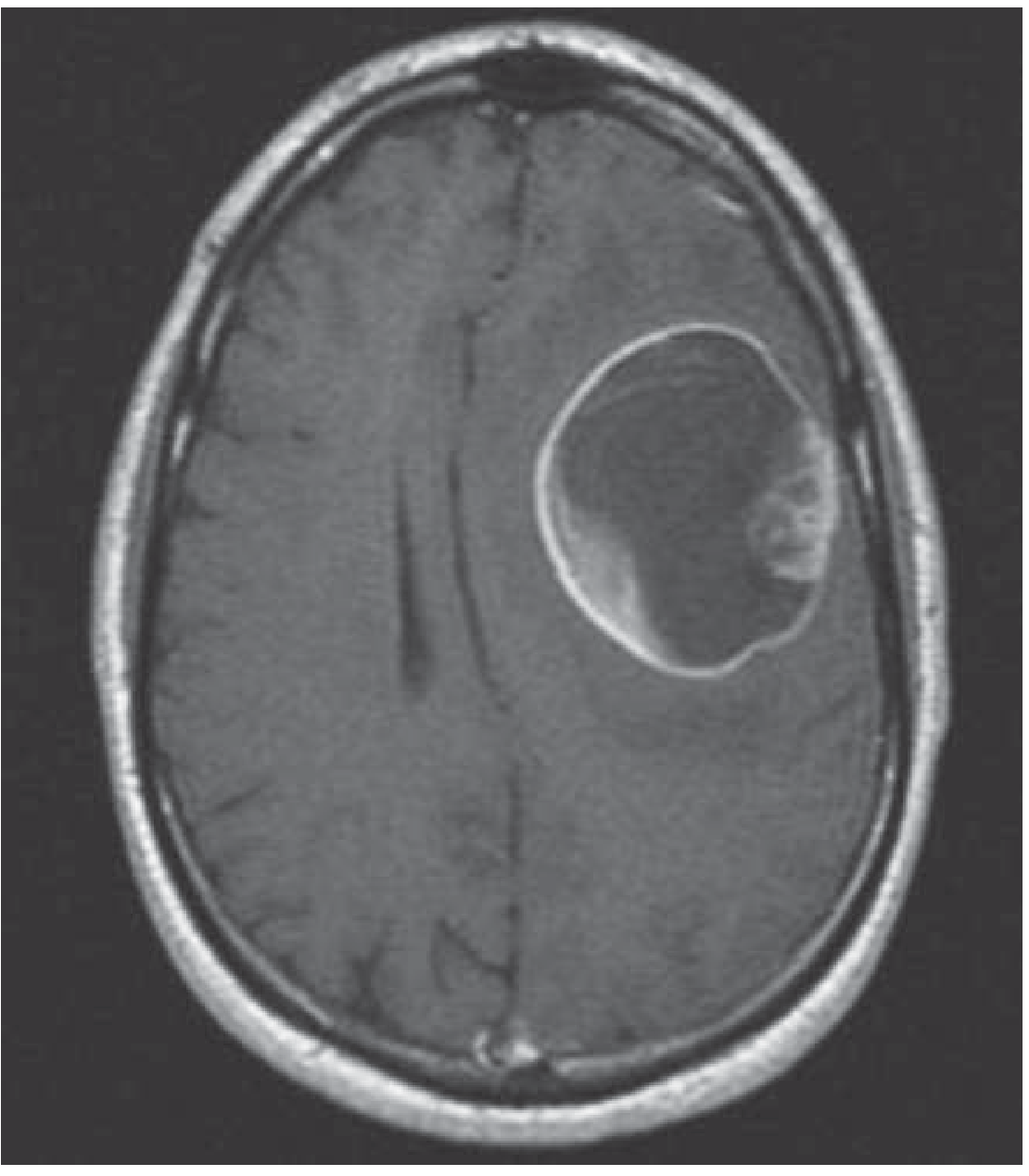
Figure 95-2: Postgadolinium T1 MRI - large cystic glioblastoma showing ring enhancement with central necrosis. (Harrison's 22E)
Pathological specimen of GBM:
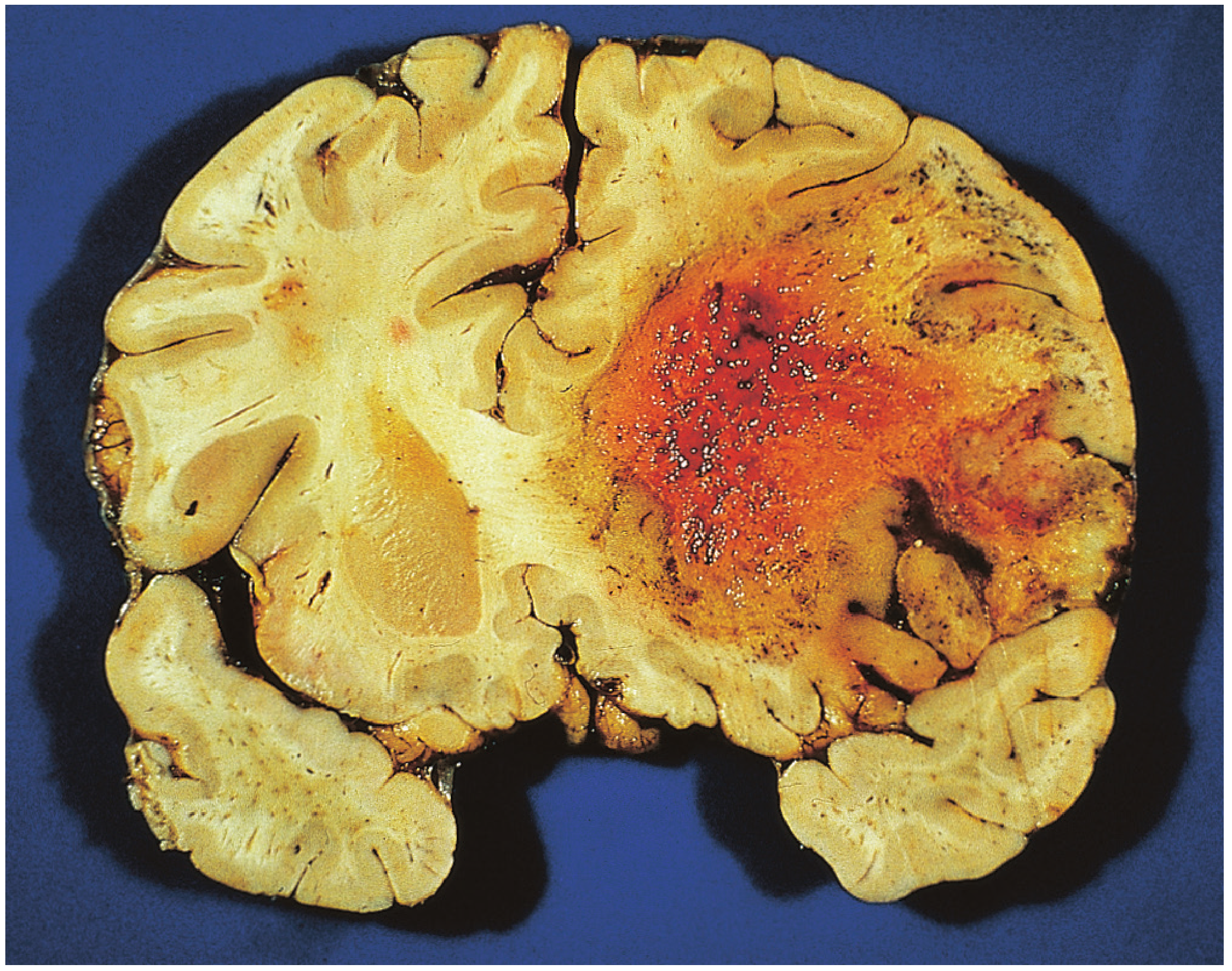
Figure 48.23: Pathological specimen of glioblastoma multiforme - note the large hemorrhagic, necrotic core. (Bailey & Love)
Diffusion-weighted imaging (DWI): Valuable for excluding brain abscess (which shows restricted diffusion) - a key differential.
5. Specific Tumor Entities
A. Astrocytoma, IDH-Mutant (Grades 2-4)
- Grade 2 (low-grade): Infiltrative, non-enhancing on MRI; presents with seizures in young adults; median survival ~10 years; transforms to higher grade in most patients
- Grade 3 (anaplastic astrocytoma): Variably enhancing; presents in 4th-5th decades
- Grade 4 (IDH-mutant glioblastoma): Treatment same as IDH-wildtype GBM; better prognosis than IDH-wildtype
- CDKN2A/B homozygous deletion upgrades IDH-mutant astrocytoma to grade 4 regardless of histology
B. Oligodendroglioma, IDH-Mutant and 1p/19q Co-deleted
- ~15-20% of all gliomas
- Hallmark histology: "fried egg" appearance (perinuclear clearing), reticular vascular pattern
- Often partially calcified on imaging
- Better response to therapy and better prognosis than pure astrocytic tumors
- Median survival >10 years for both grade 2 and grade 3
- Grade 3 (formerly anaplastic): treated with RT + PCV or temozolomide
C. Glioblastoma, IDH-Wildtype (WHO Grade 4)
- Most common malignant primary brain tumor
- MRI: ring-enhancing mass with central necrosis and surrounding edema
- Key molecular markers: EGFR amplification, TERT promoter mutation, chromosome 7 gain + 10 loss
- MGMT promoter methylation: Silences the DNA repair enzyme MGMT, making tumor more responsive to temozolomide; unmethylated MGMT = resistance to TMZ, worse prognosis
- Worst adverse prognostic factors: older age, unmethylated MGMT, poor Karnofsky performance status, unresectable tumor
6. Management
Initial Steps
- High-dose corticosteroids (dexamethasone) - to reduce peritumoral edema/mass effect
- Antiepileptics - when seizures present or temporal lobe involvement
- MRI brain with/without contrast + CT chest/abdomen/pelvis
Surgery
- Maximal safe surgical resection is primary treatment
- Aim: reduce disease burden + obtain tissue for molecular diagnosis
- Awake craniotomy used when tumor involves eloquent cortex (speech areas, motor cortex) to allow real-time mapping
- Unlike grade 1 pilocytic astrocytomas, diffuse gliomas are notably not curable by surgery alone
Low-Grade Glioma (Grade 2)
- Surgery + observation in younger patients with complete resection
- In higher-risk patients (subtotal resection or age >40): RT followed by PCV (procarbazine, lomustine, vincristine) or temozolomide
- Vorasidenib (IDH inhibitor) has shown efficacy in delaying progression and time to next intervention in IDH-mutant low-grade glioma
Glioblastoma - Standard of Care (Stupp Protocol)
- Maximal surgical resection
- Radiotherapy: 6000 cGy in 30 fractions (200 cGy/fraction) with concurrent temozolomide
- Adjuvant temozolomide for 6 months
- Result: median survival 15-18 months (vs. 12 months with RT alone); 5-year survival ~10%
Additional options:
- Carmustine wafers (BCNU): Biodegradable polymer implanted into tumor cavity at surgery - modest survival benefit
- Tumor Treating Fields (TTF): Scalp electrodes delivering low-intensity alternating electric fields - modest improvement in survival
- Bevacizumab (anti-VEGF): For recurrent GBM - improves progression-free survival and reduces edema, but does not improve overall survival
- Elderly patients (>65-70 yr): Hypofractionated RT (40 Gy over 3 weeks) + temozolomide is equivalent to standard 6-week regimen
Recurrent GBM
Options include: reoperation, re-irradiation, bevacizumab, enrollment in clinical trials. Immune checkpoint inhibitors (e.g., nivolumab) have not demonstrated benefit in GBM.
7. Molecular Markers Summary
| Marker | Significance |
|---|---|
| IDH mutation | Better prognosis; defines astrocytoma vs. oligodendroglioma vs. GBM |
| 1p/19q co-deletion | Defines oligodendroglioma; better response to PCV chemo |
| MGMT promoter methylation | Predicts temozolomide response; better prognosis in GBM |
| CDKN2A/B deletion | Upgrades IDH-mutant astrocytoma to grade 4 |
| EGFR amplification + chr 7 gain/chr 10 loss | Defines "molecular GBM" in IDH-wildtype tumors |
| TERT promoter mutation | Associated with IDH-wildtype GBM |
8. Hereditary Syndromes Associated with Glioma
Several inherited syndromes predispose to gliomas:
| Syndrome | Gene | Associated Tumors |
|---|---|---|
| NF1 | NF1/neurofibromin (17q) | Optic nerve gliomas, neurofibrosarcomas |
| NF2 | NF2/merlin (22q) | Astrocytomas, optic gliomas, meningiomas |
| Li-Fraumeni | TP53 (17p13) | Gliomas, medulloblastomas |
| Turcot syndrome | APC or hMLH1 | Glioma, medulloblastoma, colon polyps |
| TSC (Tuberous sclerosis) | TSC1/TSC2 | Subependymal giant cell astrocytoma |
| VHL | VHL gene (3p25) | Hemangioblastomas, renal cell carcinoma |
- Harrison's Principles of Internal Medicine 22E (2025)
9. Pediatric-Type Diffuse Gliomas
Pediatric gliomas have distinct molecular alterations (FGFR, MAPK, PDGFRA, EZHIP, MYCN) compared to adult-type. They can also occur in adults. Key subtypes:
- Diffuse Intrinsic Pontine Glioma (DIPG) / Diffuse Midline Glioma, H3K27-altered: WHO grade 4 regardless of histologic features; poor prognosis; arises in midline structures (pons, thalamus, spinal cord)
- Optic Pathway Glioma: Often associated with NF1; low-grade; managed with chemotherapy in young children to avoid radiation
- Pilocytic Astrocytoma (WHO grade 1): Circumscribed, often curable by surgery alone; most common in children (cerebellum, hypothalamus); only glioma type that may be cured by resection
10. Recent Evidence
A 2025 umbrella review (PMID 40598793) comparing glioma treatment strategies confirmed the survival benefit of the Stupp protocol and highlighted emerging data on vorasidenib and targeted therapies for IDH-mutant tumors. The IDH inhibitor vorasidenib (Mellinghoff et al., NEJM 2023) showed significant improvement in progression-free survival and time to next intervention in IDH1/2-mutant low-grade gliomas, and is becoming an integral part of management for this subgroup.
Sources:
- Harrison's Principles of Internal Medicine, 22nd Edition (2025), Ch. 95
- Bailey and Love's Short Practice of Surgery, 28th Edition, Ch. 48
- Bradley and Daroff's Neurology in Clinical Practice
- Adams and Victor's Principles of Neurology, 12th Edition
This is a shared conversation. Sign in to Orris to start your own chat.