Help me studying Respiratory System from Medicine
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Here are your comprehensive study notes on the Respiratory System, sourced from Murray & Nadel's Textbook of Respiratory Medicine (the gold standard reference).
🫁 Respiratory System - Detailed Study Notes
Source: Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume Set
1. ANATOMY & PHYSIOLOGY OF THE RESPIRATORY SYSTEM
Functional Overview
- The respiratory system serves gas exchange (O₂ delivery, CO₂ removal), airway defense, and phonation.
- The lung has two circulations: pulmonary (for gas exchange, low pressure) and bronchial (systemic, nourishes airways).
- Normal mean pulmonary artery pressure (mPAP) in healthy individuals: ≤20 mm Hg. Pulmonary hypertension is defined as mPAP ≥21 mm Hg.
Key Physiological Concepts
- V/Q ratio (Ventilation/Perfusion): mismatch is the most common cause of hypoxemia in lung disease.
- Low V/Q areas → venous admixture → hypoxemia
- High V/Q areas → wasted ventilation (dead space) → hypercapnia
- Alveolar-arterial (A-a) gradient: elevated in most lung diseases; normal in pure hypoventilation.
- FEV1/FVC ratio: key spirometric measurement
- < 0.70 = obstructive pattern (COPD, Asthma)
- Normal FEV1/FVC with reduced FVC = restrictive pattern (IPF, fibrosis)
- DLCO (Diffusing Capacity for Carbon Monoxide): reduced in emphysema, IPF, pulmonary vascular disease.
Lung Lymphatics
- Lymphatics are crucial for fluid balance and immune surveillance.
- In COPD: there is an increase in lymphatic vessel density, particularly near alveolar spaces, associated with worse disease severity.
- In IPF: alveolar lymphangiogenesis occurs (increase in both blood capillaries and lymphatics near alveoli). - Murray & Nadel's, p.179
2. OBSTRUCTIVE LUNG DISEASES
2.1 ASTHMA
Definition
A chronic inflammatory airway disease characterized by variable and reversible airflow obstruction, airway hyperresponsiveness, and airway inflammation.
Diagnosis & Control Assessment (GINA Guidelines)
Asthma control is assessed over the past 4 weeks with 4 criteria:
| Question | Controlled (all "No") |
|---|---|
| Daytime symptoms >2×/week? | No |
| Any night waking due to asthma? | No |
| Reliever needed >2×/week? | No |
| Any activity limitation? | No |
- Well controlled: 0 criteria present
- Partly controlled: 1-2 criteria present
- Uncontrolled: 3-4 criteria present
Severity Classification (GINA Step-Based)
- Mild asthma: well controlled on Step 1 or 2 (SABA or low-dose ICS)
- Moderate asthma: well controlled on Step 3 (low-dose ICS/LABA)
- Severe asthma: requires Step 4 or 5 to prevent becoming uncontrolled, or remains uncontrolled despite Step 4-5
Risk Factors for Poor Outcomes
- Uncontrolled symptoms
- Frequent SABA use, poor inhaler technique, not on ICS
- Comorbidities: obesity, chronic rhinosinusitis, GERD, pregnancy
- Exposures: smoking, allergens, air pollution
- Low FEV1 (<60% predicted) or highly reversible bronchoconstriction
- Psychological/socioeconomic factors
- History of severe exacerbation
Treatment Steps (NHLBI/GINA Framework)
- Core components: reverse bronchoconstriction, reduce inflammation, identify/control environmental triggers, patient-provider partnership
- Step-up if symptoms uncontrolled; step-down if controlled for ≥3 months
- Key pharmacology:
- SABA (salbutamol): reliever/rescue
- ICS (inhaled corticosteroids): cornerstone controller
- LABA (long-acting beta-2 agonists): always add to ICS, never alone
- Biologics: anti-IgE (omalizumab), anti-IL-5 (mepolizumab), anti-IL-4/13 (dupilumab) for severe eosinophilic asthma
Acute Severe Asthma Management
- Systemic corticosteroids
- Continuous nebulized SABA ± ipratropium
- IV magnesium sulfate if severe
- Heliox, NIV, intubation in life-threatening cases
Chronic Obstructive Asthma
A subtype where airflow limitation becomes fixed over time (overlap with COPD). - Murray & Nadel's, p.1684
2.2 CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD)
Definition
COPD is characterized by fixed (irreversible) airflow obstruction, excess mucus production, and enlarged alveolar spaces, most commonly caused by cigarette smoke exposure. - Murray & Nadel's, p.179
Phenotypes
- Pink Puffer (emphysema-predominant): thin, breathless, relatively preserved gas exchange, lower BMI, lung hyperinflation - may be protected against OSA
- Blue Bloater (chronic bronchitis-predominant): obese, cyanotic, high BMI, lower respiratory drive, peripheral fluid retention - higher risk for OSA
Exercise Physiology in COPD
- Mild COPD: may have normal exercise capacity
- Moderate-severe COPD: impaired VO₂max and peak work rate proportional to GOLD stage
- Unlike heart failure (cardiovascular limitation), COPD patients are limited by ventilatory pump failure
- Arterial PCO₂ remains stable or increases at peak exercise (inability to raise alveolar ventilation)
- VE at peak exercise approaches MVV (maximum voluntary ventilation)
- Low tidal volume, high respiratory rate, high end-expiratory lung volume
Dynamic Hyperinflation (key concept in COPD)
- Due to expiratory flow limitation during exercise → patients must increase end-expiratory lung volumes
- Results in:
- Flattening of diaphragm → decreased contractile strength
- Increased respiratory muscle fatigue
- Increased dyspnea
- Hemodynamic effects: impaired cardiac preload/afterload → reduced VO₂/HR
- Increased pulmonary vascular resistance → right ventricular dysfunction
- Interventions to reduce dynamic hyperinflation: lung volume reduction surgery, bronchodilators
COPD and Pulmonary Hypertension (COPD-PH)
- COPD-PH accounts for >80% of all chronic lung disease-associated PH
- Prevalence varies: 2.7-90.8% depending on definition and assessment method
- Key definitions (6th World Symposium on PH, 2019):
| Category | Criteria |
|---|---|
| CLD without PH | mPAP <21 mm Hg, or 21-24 mm Hg + PVR <3 WU |
| CLD with PH | mPAP 25-34 mm Hg, or 21-24 mm Hg + PVR ≥3 WU |
| CLD with severe PH | mPAP ≥35 mm Hg, or ≥25 mm Hg + cardiac index <2.0 L/min/m² |
- Severe PH (mPAP ≥40 mm Hg) in COPD is uncommon (~1-2%) and often has another cause (left heart disease, CTEPH)
COPD-OSA Overlap Syndrome
- First described in the 1980s. A separate named entity.
- OSA prevalence in COPD is not clearly higher than in the general population
- Mechanisms linking OSA and COPD: upper airway inflammation, skeletal myopathy (airway collapsibility), lower respiratory drive
- Clinical impact: at higher risk for hypercapnia, hypoxemia, and PH at an earlier stage than expected
- Diagnosis: polysomnography (PSG) preferred over HSAT in moderate-severe COPD; include CO₂ monitoring
- Note: medications used for COPD can be beneficial (theophylline) or harmful (inhaled corticosteroids) for concurrent OSA
2.3 BRONCHIECTASIS
Definition
Permanent abnormal dilation of the bronchi, with impaired mucociliary clearance and recurrent infections.
Hallmark Features
- Chronic productive cough (typically ≥30 mL mucoid or mucopurulent sputum/day)
- Fever, hemoptysis, weight loss in exacerbations
- Association with postnasal drip, rhinosinusitis, asthma, GERD, chronic bronchitis
Common Pathogens
- Haemophilus influenzae
- Staphylococcus aureus
- Pseudomonas aeruginosa
Imaging
- Chest X-ray: increased bronchial wall thickening (lower lobes in advanced disease)
- Thin-section (HRCT) CT chest: gold standard - shows airway wall thickening, dilation, distortion, mucus plugging, bronchiolitis
Management
- Chest physiotherapy (airway clearance) - essential
- Inhaled β₂-agonists: improve mucociliary clearance, reverse bronchoconstriction
- Postural drainage
- Intermittent antibiotic therapy
- Long-term macrolide therapy: improves exacerbations and lung function
- Antitussives: not recommended as routine (cough is the main clearance mechanism)
- Murray & Nadel's, p.875
3. RESTRICTIVE / INTERSTITIAL LUNG DISEASES
3.1 IDIOPATHIC PULMONARY FIBROSIS (IPF)
Definition
IPF is a progressive interstitial lung disease characterized by scarring (fibrosis) of the lungs, with peak incidence in the 6th decade.
Key Clinical Features
- Dyspnea on exertion (cardinal symptom)
- Chronic dry or mildly productive cough - refractory to antitussives
- Cough is often the first symptom; more common during the day than at night
- Increased capsaicin cough reflex sensitivity
- Cough is an independent predictor of progression in IPF
- Common comorbidities: postnasal drip, GERD, cough-variant asthma
Pathogenesis
- Lung microbiome: high bacterial burden (by 16S qPCR) independently associated with shorter survival
- BAL microbial communities correlate with systemic/local innate immune responses
- Murine models: lung dysbiosis preceded peak lung injury; germ-free mice had longer survival
- Rationale for studies of chronic antibiotic therapy in early IPF
- Lymphangiogenesis: increased lymphatics near alveolar spaces (Fig: CD34+/D2-40+ staining)
IPF and Pulmonary Hypertension (IPF-PH)
- Most data from patients evaluated for lung transplantation
- 32% of 79 IPF patients referred for transplant had PH on right heart catheterization
Treatment
Currently no cure; approved agents slow the rate of FVC decline:
- Pirfenidone (anti-fibrotic, anti-inflammatory) - observational data shows reduction in cough frequency
- Nintedanib (tyrosine kinase inhibitor)
- Neither pirfenidone nor nintedanib halt progression - unmet need remains
- Thalidomide: some benefit for IPF cough (trial data)
- Lung transplantation: definitive treatment in eligible patients
- Inhaled formulations under development (targeting alveolar deposition)
3.2 SARCOIDOSIS
- Systemic granulomatous disease of unknown etiology
- No reproducible microbial profile found despite long-standing hypotheses about microbial triggers
- Sensitive metagenomic analyses reveal no clearly associated microbial lineages
- After lung transplantation: sarcoidosis has the greatest propensity for recurrence in the allograft (typically asymptomatic; noncaseating granulomas on transbronchial biopsy)
4. RESPIRATORY INFECTIONS
4.1 PNEUMONIA
Pathophysiology of Hypoxemia
Hypoxemia in pneumonia is caused by:
- Increased perfusion to shunt units (consolidated lung)
- Increased perfusion to low V/Q units
Severity correlation:
- Mild-moderate pneumonia (PaO₂ ~74 mm Hg): shunt ~7.5%, low V/Q ~4.2%
- Severe pneumonia (requiring mechanical ventilation): shunt ~21.9%, low V/Q ~10.9%
- As consolidation worsens → both shunt fraction and low V/Q areas increase
Response to Supplemental Oxygen
- Depends on the degree of shunt
- True shunts (>30%) respond poorly to supplemental O₂ alone
4.2 TUBERCULOSIS (TB)
Pulmonary TB
- Caused by Mycobacterium tuberculosis
- Classic upper lobe involvement (apical and posterior segments)
- Cavitation is characteristic of reactivation disease
Extrapulmonary TB
- More difficult to diagnose: inaccessible sites, fewer bacilli, greater damage
- Common forms: pleural, lymphatic, disseminated (miliary), CNS, genitourinary, skeletal
- Bacteriologic confirmation difficult; invasive procedures often needed
Pleural TB (Tuberculous Pleuritis)
Mechanism: Type IV delayed hypersensitivity reaction triggered by TB antigens released into pleural space from rupture of subpleural parenchymal disease.
Clinical presentation:
- Can be acute or subacute
- Fever, cough, pleuritic chest pain, dyspnea, weight loss
- Effusion usually small, rarely bilateral
Pleural fluid analysis:
- Nearly always straw-colored (may be slightly bloody)
- Leukocytes: 100-5,000 cells/μL
- Early: polymorphonuclear predominance → later: lymphocyte predominance (>75% lymphocytes typical)
- Exudative (protein >50% serum protein)
- Glucose: normal to low
- Lymphocyte:neutrophil ratio typically >0.75 in established effusions
Diagnosis:
- Thoracentesis: fluid for cell count, cytology, biochemistry, microbiology
- GeneXpert (MTB/RIF), microscopy, culture from fluid or pleural tissue
- Caseating granulomas on pleural biopsy = diagnostic
- Reserve enough fluid for biopsy if exudative
Second form: TB Empyema (uncommon)
- Results from rupture of cavity → bronchopleural fistula
- Thick, cloudy fluid; may contain cholesterol (chyle-like appearance)
- Exudative; almost all lymphocytes; acid-fast smear often positive
Prognosis:
- Patients with resolved TB pleuritis have high likelihood of developing active TB within 2 years → must treat
- 10% may develop restrictive ventilatory defect after treatment (follow-up spirometry)
- Steroids in TB pleuritis: improve CXR appearance but no long-term benefit on respiratory function and associated with more adverse events (Cochrane review)
TB and the Lung Microbiome
- High abundance of oral anaerobes (Prevotella) and elevated serum short-chain fatty acids are associated with:
- Diminished IFN-γ and IL-17 production
- Increased risk for TB infection
5. HYPOXEMIA - MECHANISMS BY DISEASE
| Disease | Primary Mechanism |
|---|---|
| Pneumonia | ↑ Shunt + ↑ low V/Q (consolidation) |
| COPD | V/Q mismatch (emphysema) + diffusion impairment |
| Pleural effusion | Mild ↑ shunt (~6.9%); also right heart compression |
| Pulmonary embolism | V/Q mismatch (dead space); shunt; low mixed venous PO₂ |
| Pulmonary hypertension | Shunt + V/Q mismatch |
Pleural Effusion and Hypoxemia:
- Mild hypoxemia; shunt ~6.9%
- Thoracentesis has inconsistent effect on PaO₂ (can increase, stay same, or decrease)
- Large right-sided effusions can cause hemodynamic tamponade effect
- Treatment: early recognition and thoracentesis
Pulmonary Embolism and Hypoxemia:
- PE directly creates dead space, but patients hyperventilate in response → often present with hypocarbia
- 12% of PE patients have PaO₂ >80 mm Hg; A-a gradient can even be normal in some cases
- Mechanism is multifactorial: V/Q mismatch, atelectasis, low mixed venous PO₂
6. LUNG CANCER
Epidemiology
- Most common cause of cancer death worldwide
- Strong association with cigarette smoking
Risk After Lung Transplantation
- Arises predominantly in the native lung of single-lung transplant (SLT) recipients with underlying COPD or pulmonary fibrosis
- Frequency after SLT: up to 6.9%
- Aggressive progression - may mimic infection in the immunosuppressed host
- Mechanism: loss of antitumor immune surveillance + calcineurin inhibitor effects
- Overall prognosis: poor; curative resection only possible in rare early-stage disease
7. PLEURAL DISEASE
Pleural Effusion Classification
| Parameter | Transudate | Exudate |
|---|---|---|
| Protein (% serum) | <50% | >50% |
| Glucose | Normal | Low to normal |
| LDH | Low | Elevated |
| Causes | Heart failure, cirrhosis, nephrotic syndrome | TB, pneumonia, malignancy, PE |
IgG4-Related Pleural Disease
A rare, systemic fibroinflammatory condition.
- Pathology: lymphoplasmacytic IgG4+ plasma cell infiltration + storiform (cartwheel) fibrosis + obliterative phlebitis
- Pleural manifestations: effusion, pleural thickening (most common)
- Diagnosis: biopsy (characteristic features); elevated serum IgG4 (not sensitive/specific alone)
- PET imaging: often avid
- Increased risk of malignancy - further imaging required
- Treatment: oral corticosteroids; rituximab for resistant/relapsing cases
8. DRUG-INDUCED RESPIRATORY DISEASE
ACE Inhibitor Cough
- Incidence: 2-33% of patients taking ACE inhibitors
- Character: dry, tickly, irritating sensation in throat
- Onset: hours to months after starting
- Resolution: days to weeks after stopping
- Mechanism: accumulation of bradykinin and prostaglandins → sensitize cough receptors
- Management: stop ACE inhibitor → switch to ARB (angiotensin II receptor antagonist)
- First step in any workup of cough in a patient on an ACE inhibitor: stop the drug and reassess
Post-Infectious Cough
- Occurs in up to 25% of patients with chronic cough
- Up to 50% after Mycoplasma or Bordetella pertussis infection
- B. pertussis cough can last 4-6 weeks especially in older children and adults
- Initial trigger: usually upper respiratory tract infection
- Treatment: macrolide antibiotics or TMP-SMX to eliminate B. pertussis (but does NOT alter subsequent clinical course); inhaled corticosteroids with variable success; oral steroids may help
9. RESPIRATORY PHYSIOLOGY - HIGH-YIELD SUMMARY TABLE
| Measure | Normal | Obstructive (COPD/Asthma) | Restrictive (IPF) |
|---|---|---|---|
| FEV1/FVC | >0.70 | <0.70 | Normal or ↑ |
| FVC | Normal | Normal or ↓ | ↓↓ |
| FEV1 | Normal | ↓ | ↓ |
| TLC | Normal | ↑ (hyperinflation) | ↓ |
| RV | Normal | ↑ | ↓ |
| DLCO | Normal | ↓ (emphysema) | ↓ (IPF) |
10. KEY MNEMONICS & HIGH-YIELD FACTS
COPD key features:
- Fixed airflow obstruction (FEV1/FVC <0.70, no significant reversibility)
- Dynamic hyperinflation → dyspnea during exercise
- Ventilatory pump fails before cardiovascular system at peak exercise
Asthma key features:
- Variable, reversible airflow obstruction
- FEV1 improves ≥12% AND ≥200 mL with bronchodilator = significant reversibility
- Nighttime/early morning symptoms are characteristic
IPF key facts:
- Only disease where cough independently predicts progression
- Two approved antifibrotics: pirfenidone and nintedanib
- Honeycombing on HRCT in lower lobes = IPF pattern
TB pleuritis key facts:
- Lymphocytic exudate
- Type IV hypersensitivity mechanism
- Resolve spontaneously but need treatment (active TB develops in 2 years if untreated)
Bronchiectasis treatment backbone:
- Airway clearance + chest physiotherapy + macrolides
All content sourced from: Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume Set (ISBN: 9780323655873). These are among the most detailed, authoritative respiratory medicine study notes available.
This covers the full respiratory system curriculum. Let me know which area you want to dive deeper into - for example, I can expand on COPD management (GOLD guidelines), TB treatment regimens, pulmonary function testing interpretation, pleural disease workup, or lung cancer staging and treatment.
Can you make detailed notes based on Davidson book
Finding Sources
Finding Sources
Finding Sources
Davidson's Principles and Practice of Medicine is not in the library. The available internal medicine books are Harrison's (22nd Ed, 2025), Goldman-Cecil Medicine, Washington Manual, and Frameworks for Internal Medicine. Harrison's is the closest equivalent in scope and prestige to Davidson's.
Let me confirm and offer alternatives:
Davidson's Principles and Practice of Medicine is not available in the textbook library. The library does not have that specific title.
However, these equivalent internal medicine references are available:
| Book | Edition | Notes |
|---|---|---|
| Harrison's Principles of Internal Medicine | 22nd Ed (2025) | Most comprehensive; global gold standard |
| Goldman-Cecil Medicine | Current Ed | Strong clinical focus, similar to Davidson's |
| Washington Manual of Medical Therapeutics | Current Ed | Concise, practical management focus |
| Frameworks for Internal Medicine | Current Ed | Evidence-based, diagnostic approach |
Harrison's 22nd Edition (2025) is the closest alternative to Davidson's in depth, structure, and exam relevance - it covers all the same respiratory topics (COPD, Asthma, TB, Pneumonia, IPF, Lung Cancer, Pleural disease, Respiratory Failure) in a similar clinical style.
Would you like me to:
- Make the same detailed Respiratory System notes from Harrison's 22nd Edition - this is the most direct alternative and is considered more comprehensive than Davidson's
- Use Goldman-Cecil Medicine - strong clinical correlation focus
- Combine Harrison's + Goldman-Cecil for the most complete notes
Which would you prefer?
Make detailed respiratory notes from Harrison's 22nd Edition
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Here are your detailed Respiratory System notes directly from Harrison's Principles of Internal Medicine, 22nd Edition (2025):
🫁 Respiratory System - Detailed Study Notes
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025)
1. ASTHMA (Chapter 298)
Definition & Overview
Asthma is a chronic inflammatory airway disease with variable and reversible airflow obstruction, airway hyperresponsiveness, and mucosal inflammation. It requires both trigger reduction and pharmacologic management.
Goals of Therapy
Two main domains:
- Control of current symptoms - minimize day-to-day symptoms and activity limitation
- Reduce future risk - prevent exacerbations, preserve lung function, avoid medication side effects
Reducing Triggers
- Occupational exposures: removal from environment may result in complete resolution
- Allergen immunotherapy: reduces IgE-mediated reactions; recommended only in patients with mild to moderate controlled asthma (risk of anaphylaxis in uncontrolled asthma)
- Sublingual immunotherapy: evidence base is not substantial for isolated asthma
- Vaccination: strongly advised - annual influenza, pneumococcal vaccines (regardless of age), COVID-19, RSV vaccines
- Environmental control: dust mite covers effective only as part of a comprehensive allergen mitigation strategy
Medications
Bronchodilators
β₂-Agonists
- Activate β₂-receptors on airway smooth muscle → G protein-coupled → activate adenyl cyclase → ↑ cyclic AMP → smooth muscle relaxation
- SABAs (Short-acting β₂-agonists): primary reliever/rescue; also used before exercise
- ⚠ Regular SABA use → tachyphylaxis of bronchoprotective effect + possible increased airway reactivity
- LABAs (Long-acting β₂-agonists): must NEVER be used alone in asthma (increased risk of asthma death)
- Always combine with ICS
Anticholinergics (Muscarinic antagonists)
- Short-acting: ipratropium - useful in acute settings, additive to β₂-agonists
- Long-acting: tiotropium - approved as add-on therapy in uncontrolled asthma
Theophylline
- Narrow therapeutic window; now rarely used
- Potential benefit in OSA-COPD overlap
Controller Medications
- Inhaled Corticosteroids (ICS): cornerstone of asthma control; reduce airway inflammation
- Leukotriene receptor antagonists (LTRAs): montelukast - useful add-on or alternative
- Biologics (for severe, uncontrolled asthma):
- Anti-IgE: omalizumab
- Anti-IL-5: mepolizumab, benralizumab
- Anti-IL-4/13: dupilumab
Management of Acute Asthma Attacks
Mild-moderate:
- Nebulized β₂-agonist up to every 20 min
- PEFR or FEV₁ assessment
- If PEFR >60% predicted → usually responds to β₂-agonists alone
- If fails to respond in 1-2 h → IV corticosteroids
- Supplemental O₂ for hypoxemia
- LTRA and magnesium sometimes added
- Nebulized anticholinergics for additional bronchodilation
Severe/Refractory:
- Continuous bronchodilator nebulization
- NIV (non-invasive positive pressure ventilation) to prevent intubation
- Helium-oxygen (heliox) mixtures to reduce work of breathing
- Normal or near-normal PCO₂ in a breathless asthmatic = warning sign of impending respiratory failure
- If intubation needed: aim for low respiratory rate and low tidal volume
- Permissive hypercapnia: allow PCO₂ to rise; correct critical acidosis temporarily with bicarbonate
- Neuromuscular paralysis sometimes beneficial
- Antibiotics ONLY if clear evidence of bacterial infection
High-Risk Patients for Asthma Mortality
(Harrison's Table 298-6)
- History of ICU admission for asthma
- History of intubation for asthma
- Illicit drug use
- Depression
- New diagnosis within past year
- Non-adherence to treatment
Exercise-Induced Asthma
- May reflect poor overall asthma control → step-up therapy first
- Strategies: warm-up before exercise, mask in cold weather
- Pre-treatment with SABA raises threshold for exercise-induced bronchoconstriction
- LABAs extend protection but should not be used alone
Asthma-COPD Overlap (ACO)
- Patients with features of both asthma and COPD
- Variable airflow limitation but incompletely reversible
- Treatment: ICS is essential (unlike pure COPD where ICS has more limited role)
2. CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) (Chapter 303)
Definition
Fixed (irreversible) airflow obstruction (FEV₁/FVC <0.70 post-bronchodilator) caused primarily by cigarette smoke exposure; encompasses emphysema and chronic bronchitis.
Clinical Features
Symptoms (progressive):
- Dyspnea on exertion → at rest in advanced disease
- Chronic productive cough
- Use of validated questionnaires: CAT (COPD Assessment Test) and mMRC (Modified Medical Research Council) dyspnea scale
Common comorbidities (must assess):
- Cardiovascular disease
- Gastroesophageal reflux (GERD)
- Osteoporosis
- Frailty, depression, anxiety
Physical Examination
- Early COPD: normal examination
- Moderate-severe COPD:
- Prolonged expiratory phase
- Expiratory wheeze
- Barrel chest (hyperinflation)
- ↓ diaphragmatic excursion (on percussion)
- Use of accessory muscles (SCM, scalene, intercostal)
- Tripod sitting position
- Cyanosis (lips, nail beds)
- Advanced disease:
- Cachexia - weight loss, loss of subcutaneous fat (due to poor intake + elevated TNF-α) → independent poor prognostic factor
- Cor pulmonale (rare since supplemental O₂ era)
- ⚠ Clubbing is NOT a sign of COPD - if present, investigate for lung cancer
Laboratory Findings
- Spirometry: FEV₁/FVC <0.70 (post-bronchodilator) - diagnostic criterion
- Severity grading: GOLD classification by FEV₁ % predicted
- With worsening disease: ↑ TLC, ↑ FRC, ↑ RV (air trapping/hyperinflation)
- DLCO reduced in emphysema (parenchymal destruction)
- BODE Index (better mortality predictor than FEV₁ alone):
- B - Body mass index
- O - airflow Obstruction (FEV₁)
- D - Dyspnea (mMRC scale)
- E - Exercise tolerance (6-minute walk distance)
- ABG/oximetry: resting or exertional hypoxemia; assess for hypercapnia
COPD Treatment Goals
- Symptomatic relief: reduce symptoms, improve exercise tolerance, improve health status
- Reduce future risk: prevent disease progression, prevent/treat exacerbations, reduce mortality
Interventions That Improve Survival in COPD
(Harrison's - explicitly listed):
- Smoking cessation - returns rate of FEV₁ decline toward non-smoker rate
- Long-term oxygen therapy (LTOT) in chronically hypoxemic patients (PaO₂ ≤55 mmHg, or ≤59 mmHg with cor pulmonale/polycythemia)
- Lung Volume Reduction Surgery (LVRS) in selected emphysema patients
- Triple inhaled therapy (LABA + LAMA + ICS) - reduces mortality in selected patients
- Pulmonary rehabilitation (especially after hospitalization)
- NIV (NIPPV) in severe hypercapnia
- Lung transplantation (evidence less strong)
Pharmacotherapy
Smoking Cessation Pharmacotherapy:
- Nicotine replacement therapy (patch, gum, lozenge, inhaler, nasal spray)
- Bupropion
- Varenicline (nicotinic acid receptor agonist/antagonist) - most effective
- All adult non-pregnant smokers should be offered pharmacotherapy + counseling
Bronchodilators (primary pharmacotherapy):
| Drug Class | Examples | Effect |
|---|---|---|
| LAMA (Long-acting muscarinic antagonist) | Tiotropium, aclidinium, glycopyrrolate, umeclidinium | ↓ Symptoms, ↓ exacerbations; most effective bronchodilator class in COPD |
| LABA (Long-acting beta agonist) | Formoterol, salmeterol, indacaterol, olodaterol, vilanterol | ↓ Symptoms, ↓ exacerbations (less than LAMA) |
| LABA + LAMA combination | Multiple combinations | Superior to either alone for symptoms + exacerbation prevention |
| SABA (Short-acting beta agonist) | Salbutamol (albuterol) | Acute relief |
| SAMA | Ipratropium | Acute relief, improves FEV₁ |
ICS in COPD:
- NOT first-line; added when exacerbations persist on LABA+LAMA
- Triple therapy (LABA + LAMA + ICS): reduces mortality in high-risk patients
- Side effects: pneumonia risk, oral candidiasis, adrenal suppression
PDE4 inhibitors:
- Roflumilast: oral; reduces exacerbations in severe COPD with chronic bronchitis phenotype; add-on therapy
COPD Exacerbations
Definition: Acute worsening of respiratory symptoms beyond normal day-to-day variation requiring a change in therapy.
Triggers: Respiratory infections (viral >bacterial), air pollution
Treatment:
- Short-acting bronchodilators: SABAs ± SAMAs - first-line
- Systemic corticosteroids: 40 mg prednisolone for 5 days (not longer - no additional benefit, more side effects)
- Antibiotics: if 2 or more of: increased dyspnea, increased sputum volume, increased sputum purulence (Anthonisen criteria); amoxicillin/doxycycline/macrolide
- NIV (NIPPV): for acute hypercapnic respiratory failure (pH <7.35 + PaCO₂ >45 mmHg) - reduces need for intubation and mortality
- Hospitalization if severe
Chronic Hypercapnic COPD
- Indicates advanced disease; associated with worse survival
- Home NIPPV (High-intensity BiPAP): for stable chronic hypercapnic COPD (PaCO₂ >52 mmHg, normal pH)
- Target: reduce PaCO₂ to <48 mmHg or >20% drop from baseline
- IPAP: 24-28 cmH₂O with backup rate
- Improves 1-year mortality vs. standard care (home O₂ alone)
- After acute exacerbation: retest for PaCO₂ 2-4 weeks post-discharge; only start NIV if persistent hypercapnia (PaCO₂ >52 mmHg) after exacerbation resolves → reduces hospital readmissions and 1-year mortality
3. PNEUMONIA (Chapter 131)
Classification (Revised)
- Community-acquired pneumonia (CAP) - acquired outside hospital
- Hospital-acquired pneumonia (HAP) - ≥48 h after hospital admission, not incubating on admission
- Ventilator-associated pneumonia (VAP) - ≥48-72 h after endotracheal intubation
- ⚠ "Healthcare-associated pneumonia (HCAP)" - discontinued category (did not reliably predict resistant organisms, led to overuse of broad-spectrum antibiotics)
- Aspiration pneumonia: accounts for 5-15% of CAP; involves oropharyngeal or gastric contents
Pathophysiology
- New concept: lungs are NOT sterile - they have a resident lung microbiota
- Microbial entry: inhalation, microaspiration (most common), direct mucosal spread
- Microbiota determined by: rate of entry, rate of elimination, and regional growth conditions (pH, O₂ tension, temperature)
- Positive feedback loop model:
- Inflammatory event → epithelial/endothelial injury → cytokines/chemokines/catecholamines → selectively promotes growth of pathogens (e.g., S. pneumoniae, Pseudomonas)
- This cycle accelerates → dominant pathogen emerges → clinical pneumonia
- In CAP/HAP: trigger often viral infection + microaspiration
- Innate + adaptive immunity may contain the infection, but if positive feedback loop becomes self-sustaining → full pneumonia syndrome
Common Causative Organisms
CAP:
- Streptococcus pneumoniae (most common)
- Haemophilus influenzae
- Atypicals: Mycoplasma pneumoniae, Chlamydophila pneumoniae, Legionella pneumophila
- Respiratory viruses (influenza, RSV, SARS-CoV-2)
HAP/VAP:
- Gram-negatives: Pseudomonas aeruginosa, Klebsiella pneumoniae, Escherichia coli, Acinetobacter
- MRSA (especially in ICU)
- Risk factors for drug-resistant organisms: prior hospitalization, recent antibiotics, structural lung disease, immunosuppression
Assessment of Severity: PSI and CURB-65
CURB-65 Score (1 point each):
- C - Confusion (new onset)
- U - Urea >7 mmol/L (BUN >19 mg/dL)
- R - Respiratory rate ≥30/min
- B - Blood pressure (systolic <90 or diastolic ≤60 mmHg)
- 65 - Age ≥65 years
| Score | Risk | Management |
|---|---|---|
| 0-1 | Low | Outpatient |
| 2 | Moderate | Consider hospitalization |
| 3-5 | High | Hospitalize; ICU if ≥4 |
Treatment
Outpatient CAP (no comorbidities):
- Amoxicillin OR doxycycline OR azithromycin
Outpatient CAP (with comorbidities - diabetes, chronic liver/lung/heart/renal disease, immunosuppression, prior antibiotics in last 3 months):
- Respiratory fluoroquinolone (levofloxacin, moxifloxacin) OR
- Beta-lactam + macrolide combination
Inpatient CAP (non-ICU):
- Beta-lactam (ampicillin-sulbactam, cefotaxime, ceftriaxone) + macrolide OR
- Respiratory fluoroquinolone alone
Inpatient CAP (ICU):
- Beta-lactam + macrolide OR beta-lactam + respiratory fluoroquinolone
- Add MRSA coverage (vancomycin/linezolid) or Pseudomonas coverage if risk factors present
4. TUBERCULOSIS (Chapter 186)
Historical Background
- Earliest documented human case: 9000 years ago
- Streptomycin isolated from Streptomyces griseus in 1943 → launched antibiotic era
- Treatment shortened progressively from years → 6 months for drug-susceptible TB
Diagnosis
Methods used:
- History, physical examination, chest X-ray
- Tuberculin Skin Test (TST) (Mantoux)
- Interferon-γ release assays (IGRAs) - e.g., QuantiFERON-TB Gold, T-SPOT.TB
- Acid-fast staining (Ziehl-Neelsen)
- Mycobacterial cultures (gold standard but slow - weeks)
- Molecular diagnostics: GeneXpert MTB/RIF - rapid, detects TB and rifampin resistance
Latent TB Infection (LTBI) Treatment
Preferred regimen (current):
- 3HP: Isoniazid + Rifapentine once weekly × 3 months (12 doses)
- Regimen of choice for children >2 years, all adults including HIV+
- NOT for pregnant women or those with hypersensitivity to INH or rifampin
Other regimens:
- 4R: Rifampin daily × 4 months - preferred over INH alone in adults/children
- 3HR: Isoniazid + Rifampin daily × 3 months
- 6-9H: Isoniazid alone × 6-9 months (less preferred now)
- 1HP: Rifapentine + Isoniazid daily × 1 month - for HIV+ (noninferior to 9H); included in 2020 WHO guidelines
⚠ Caution in HIV+: potential drug interactions; possibility of subclinical TB disease → could develop rifampin resistance
Active TB Treatment
Standard regimen (drug-susceptible TB):
| Phase | Duration | Drugs |
|---|---|---|
| Intensive phase | 2 months | HRZE: Isoniazid (H) + Rifampin (R) + Pyrazinamide (Z) + Ethambutol (E) |
| Continuation phase | 4 months | HR: Isoniazid + Rifampin |
| Total | 6 months |
Extension to 9 months (7-month continuation phase) if ANY of:
- Cavitary disease on chest X-ray
- 2-month course of pyrazinamide not completed
- Sputum cultures remain positive at 2 months (delayed culture conversion)
- Delayed culture conversion also warrants evaluation for drug resistance
New 4-Month Regimen (2020 multinational RCT):
- Rifapentine + Isoniazid + Pyrazinamide + Moxifloxacin × 8 weeks, then
- Rifapentine + Isoniazid + Moxifloxacin × 9 weeks
- Noninferior to standard 6-month HRZE regimen
- Includes HIV+ patients with CD4 >100
- Conditional WHO recommendation (newer guidelines)
Drug-Resistant TB
- MDR-TB: resistant to at least isoniazid AND rifampin → requires 18-24 month regimens with second-line drugs
- XDR-TB: MDR-TB + resistant to fluoroquinolones + second-line injectables
- New drugs: bedaquiline, delamanid - now incorporated into WHO-recommended regimens
5. INTERSTITIAL LUNG DISEASES (ILD) (Chapter 304)
Classification of ILD
- Idiopathic Interstitial Pneumonias (IIPs): IPF, NSIP, COP, DIP, RB-ILD
- ILD with known cause: CTD-associated, drug-induced, occupational
- Granulomatous ILD: Sarcoidosis, HP (hypersensitivity pneumonitis)
- Other: LAM, PLCH
5.1 IDIOPATHIC PULMONARY FIBROSIS (IPF)
Epidemiology:
- Most common ILD of unknown cause
- Prevalence: 50-200 per 100,000
- Peak incidence: 5th-6th decade
- Men > Women
- Associated with smoking history and other environmental exposures
- Poor prognosis: estimated 50% 3-5 year survival
Clinical Manifestations:
- Progressive dyspnea on exertion
- Chronic dry cough (refractory to antitussives)
- Bibasal fine inspiratory crackles ("Velcro crackles")
- Clubbing (in ~50%)
- Eventually: pulmonary hypertension, cor pulmonale, respiratory failure
HRCT Findings (UIP pattern - Usual Interstitial Pneumonia):
- Subpleural, posterior basal predominance of reticulation
- Honeycombing (stacked cystic airspaces)
- Traction bronchiectasis
- The combination = UIP pattern = diagnostic of IPF (in right clinical context, no need for biopsy)
- ⚠ Extensive ground-glass opacities, upper lung predominance, bronchovascular pattern, micronodules → suggest alternative diagnosis
Histopathology (VATS biopsy - UIP pattern):
- Subpleural reticulation with honeycomb changes
- Fibroblast foci (subepithelial collections of myofibroblasts + collagen)
- Fibrotic changes alternating with normal alveolar architecture = temporal and spatial heterogeneity
Imaging comparison:
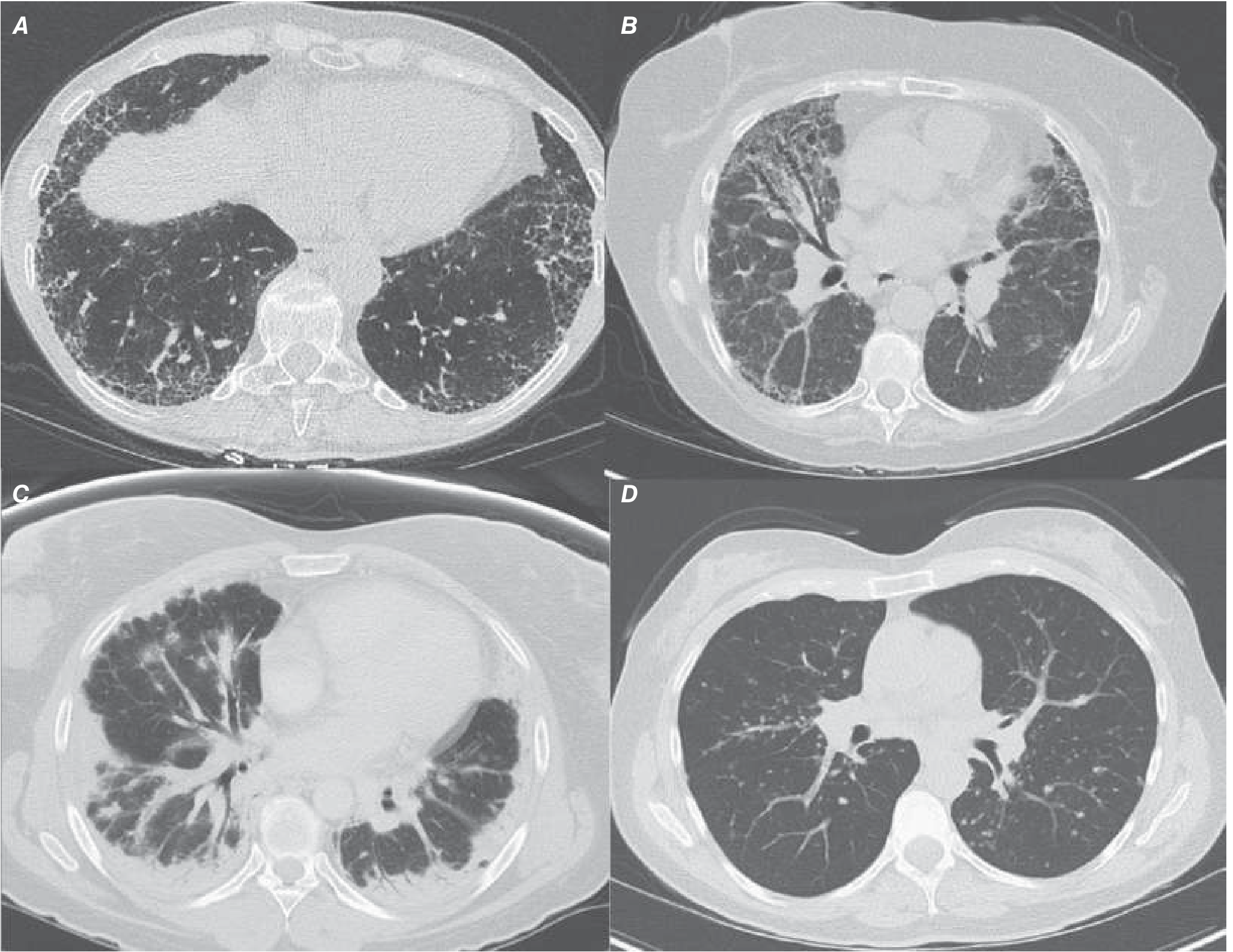 A: IPF (UIP pattern - basal, subpleural honeycombing + traction bronchiectasis) | B: NSIP (symmetric ground-glass) | C: COP (patchy subpleural consolidation) | D: Sarcoidosis (hilar lymphadenopathy + bronchovascular nodules)
A: IPF (UIP pattern - basal, subpleural honeycombing + traction bronchiectasis) | B: NSIP (symmetric ground-glass) | C: COP (patchy subpleural consolidation) | D: Sarcoidosis (hilar lymphadenopathy + bronchovascular nodules)
Treatment:
- Historically felt to be refractory → changed in 2014 with landmark antifibrotic trials
- Pirfenidone and Nintedanib: approved antifibrotics; both slow rate of FVC decline
- Meta-analyses suggest antifibrotics may also improve survival
- ⚠ Immunosuppression (steroids + azathioprine + NAC): shown to increase morbidity and mortality in IPF → do NOT use
- Physical therapy + supplemental O₂: improves exercise tolerance, reduces pulmonary hypertension risk
- Lung transplantation: extends survival and improves QoL in eligible patients
- Antifibrotics are also showing efficacy in other progressive fibrotic ILDs
5.2 NON-SPECIFIC INTERSTITIAL PNEUMONIA (NSIP)
Clinical:
- Commonly diagnosed in non-smoking women in their 5th decade
- Frequently associated with CTD (connective tissue disease)
- Also: familial interstitial pneumonia, drug toxicity, infection
- Positive CTD serologies often found
- Better prognosis than IPF: 5-year survival >80%
HRCT:
- Diffuse subpleural, symmetric, bilateral ground-glass + reticular opacities
- Lower lung zone predominance
- Volume loss, traction bronchiectasis
- Occasional subpleural sparing
- Honeycombing uncommon (key distinction from IPF)
Histopathology:
- Uniform interstitial inflammation and fibrosis (unlike temporal heterogeneity of IPF)
- Two subtypes:
- Cellular NSIP: better prognosis, more responsive to therapy
- Fibrotic NSIP: worse prognosis, less responsive
Treatment:
- Oral corticosteroids (prednisone)
- Cytotoxic agents: mycophenolate, azathioprine, cyclophosphamide
- Biologics: rituximab, tocilizumab
- Progressive fibrotic NSIP: may benefit from antifibrotics (recent trials)
5.3 SARCOIDOSIS
HRCT pattern: Mediastinal and hilar lymphadenopathy + circular-nodular opacities along bronchovascular bundles (most characteristic); also miliary pattern, ground-glass, mosaic attenuation.
5.4 SMOKING-RELATED ILD
- RB-ILD (Respiratory Bronchiolitis-ILD)
- DIP (Desquamative Interstitial Pneumonia)
- PLCH (Pulmonary Langerhans Cell Histiocytosis)
- All associated with active or prior tobacco smoke exposure
6. LUNG CANCER (Chapter 83)
Pathology (WHO Classification)
Tumors arising from respiratory epithelium (bronchi, bronchioles, alveoli):
| Type | Key Features |
|---|---|
| Adenocarcinoma | Most common overall; peripheral; often in never-smokers; EGFR, ALK, ROS1 mutations |
| Squamous cell carcinoma | Central; associated with smoking; cavitation; hypercalcemia (PTHrP) |
| Large-cell carcinoma | Peripheral; anaplastic; diagnosis of exclusion |
| Small-cell lung cancer (SCLC) | Central; small cells with scant cytoplasm; neuroendocrine; very aggressive; responds initially to chemo |
| NSCLC | Collective term for adenocarcinoma + squamous cell + large-cell |
Inherited Predisposition
- CYP1A1 polymorphisms (P450 enzyme system) → ↑ carcinogen metabolism risk
- First-degree relatives of lung cancer patients: 2-3-fold excess risk
- Germline mutations: RB (retinoblastoma patients), TP53 (Li-Fraumeni syndrome)
- Common genetic loci: 5p15 (telomerase), 6p21, 15q25 (acetylcholinergic receptors)
- Rare EGFR germline mutation (T790M) - lung cancer in never smokers
- 14.9% of primary lung cancer patients have ≥1 pathogenic germline variant (mostly DNA damage repair genes)
Staging
NSCLC (TNM staging - anatomic):
- Stage I-II: localized → surgery curative intent
- Stage III: locally advanced → concurrent chemoradiation
- Stage IV: metastatic → systemic therapy (targeted therapy if driver mutation; immunotherapy if no driver; chemotherapy)
SCLC (two-stage system):
- Limited disease (LD): confined to one hemithorax + regional lymph nodes (can be encompassed in radiotherapy field) → concurrent chemoradiation + prophylactic cranial irradiation (PCI)
- Extensive disease (ED): beyond above → systemic chemotherapy ± immunotherapy; PCI controversial
Molecular Targets in NSCLC (Adenocarcinoma)
- EGFR mutations: osimertinib (3rd-gen TKI) - first-line
- ALK rearrangements: alectinib, brigatinib, lorlatinib
- ROS1 rearrangements: crizotinib, entrectinib
- BRAF V600E: dabrafenib + trametinib
- MET exon 14 skipping: capmatinib, tepotinib
- KRAS G12C: sotorasib, adagrasib
- PD-L1 high (≥50%), no driver mutation: pembrolizumab first-line immunotherapy
7. PLEURAL DISEASE (Chapter 305)
Pleural Effusion
Normal physiology:
- Fluid enters pleural space from parietal pleural capillaries → removed by parietal pleural lymphatics
- Lymphatics can absorb 20× normal fluid formation rate
- Effusion forms when fluid formation overwhelms lymphatic removal
Etiology: Transudative vs. Exudative
| Feature | Transudate | Exudate |
|---|---|---|
| Mechanism | Systemic hydrostatic-oncotic imbalance | Local factors disrupting pleural fluid homeostasis |
| Common causes | LV failure (most common in US), cirrhosis, nephrotic syndrome | Bacterial pneumonia (parapneumonic), malignancy, viral infection, pulmonary embolism, TB |
Light's Criteria for Exudate
(Effusion is exudate if it meets ≥1):
- Pleural fluid protein / serum protein > 0.5
- Pleural fluid LDH / serum LDH > 0.6
- Pleural fluid LDH > 2/3 of upper limit of normal serum LDH
⚠ Pseudoexudates: Light's criteria misidentify ~25% of transudates as exudates (often "diuresed transudates" in heart failure patients). If clinically a transudate but meets exudate criteria → use serum-to-pleural fluid protein gradient (SPPG) or serum-to-pleural fluid albumin gradient (SPAG):
- SPAG >1.2 g/dL = transudate despite meeting Light's criteria
Diagnostic Approach
- Imaging (US / CT / CXR) to evaluate extent and guide thoracentesis
- Thoracentesis to differentiate transudate vs. exudate
- If exudate → further workup: cytology, cultures, adenosine deaminase (ADA), pH, glucose
8. RESPIRATORY FAILURE (Chapter 311)
Classification
Type I: Acute Hypoxemic Respiratory Failure
- Mechanism: Alveolar flooding → V/Q mismatch + intrapulmonary shunt
- Causes: pulmonary edema (cardiogenic or ARDS), pneumonia, alveolar hemorrhage, COVID-19, near-drowning, aspiration, sepsis, multiple transfusions, pancreatitis
- ARDS = Type I RF with: acute onset (≤1 week), bilateral opacities on imaging, not fully explained by cardiac failure, requiring PEEP
- Traditional ARDS mortality: 50-70%; current rates closer to 30% due to improved care
- COVID-19 pandemic → substantially increased incidence of viral-mediated ARDS
ARDS Management (Lung-Protective Ventilation):
- Key principle: mechanical ventilation can worsen lung injury (volutrauma)
- ARDS pressure-volume curve is nonlinear (Fig 311-5):
- Lower inflection point: collapsed alveoli begin to open
- Upper deflection point: alveoli become overdistended
- Low tidal volume strategy: 6 mL/kg ideal body weight (vs. traditional 12 mL/kg)
- Landmark RCT: mortality reduced from 39.8% → 31%
- Prone positioning: improves survival in severe ARDS; widely used in COVID-19 ARDS
- Neuromuscular blockade: select patients may benefit
- Fluid-conservative strategy (low CVP/PCWP): associated with fewer ventilator days vs. fluid-liberal strategy
- PEEP: prevents end-expiratory alveolar collapse
Type II: Hypercapnic (Ventilatory Failure)
- Mechanism: inability to maintain adequate alveolar ventilation → CO₂ retention
- Causes: COPD, neuromuscular disease, chest wall disease, central hypoventilation, obesity hypoventilation
- Chronic hypercapnic COPD: PaCO₂ >52 mmHg with normal pH
- Home high-intensity BiPAP improves 1-year mortality (see COPD section)
Type III: Perioperative / Atelectatic
- Mechanism: atelectasis due to anesthesia, pain, secretion retention
Type IV: Hypoperfusion
- Mechanism: shock → respiratory muscle ischemia → failure
Central Hypoventilation Syndrome
- Congenital form: Ondine's Curse (CCHS) - mutation in PHOX2B gene (transcription factor in neuronal development)
- Features:
- Absent respiratory response to hypoxia OR hypercapnia
- Mildly elevated PaCO₂ while awake
- Markedly elevated PaCO₂ during non-REM sleep
- Can normalize PaCO₂ during exercise and REM sleep
- Treatment: NIPPV or mechanical ventilation; consider phrenic nerve or diaphragmatic pacing
Hyperventilation Syndrome
- Ventilation in excess of metabolic requirements → ↓ PaCO₂
- Symptoms: dyspnea, paresthesias, tetany, headache, dizziness, visual disturbances, atypical chest pain
- Anxiety disorders: both initiating and sustaining factor (but not necessary for development)
- Important: anxiety disorders ≠ hyperventilation syndrome (they are separate entities that can coexist)
9. HIGH-YIELD SUMMARY TABLES
Spirometry Pattern Summary
| Pattern | FEV₁/FVC | FVC | FEV₁ | TLC | DLCO | Examples |
|---|---|---|---|---|---|---|
| Obstructive | <0.70 | N or ↓ | ↓↓ | ↑ (air trap) | ↓ (emphysema) | COPD, Asthma |
| Restrictive | N or ↑ | ↓↓ | ↓ | ↓ | ↓ | IPF, NSIP, pleural disease |
| Mixed | <0.70 | ↓↓ | ↓↓ | ↓ or N | ↓ | Advanced COPD + fibrosis |
Pleural Fluid Analysis Quick Reference
| Test | Transudate | Exudate |
|---|---|---|
| Protein ratio (PF/serum) | <0.5 | >0.5 |
| LDH ratio (PF/serum) | <0.6 | >0.6 |
| Glucose | Normal | Low (empyema, TB, malignancy) |
| pH | Normal | <7.2 (empyema, needs drainage) |
| ADA | Low | High in TB (>40 U/L) |
| Cytology | Negative | Positive in malignancy |
Key Drug Mnemonics
TB active treatment: HRZE × 2 months → HR × 4 months
- H = Isoniazid
- R = Rifampin
- Z = Pyrazinamide
- E = Ethambutol
COPD survival-improving interventions: STOP-LT
- Smoking cessation
- Triple inhaled therapy (selected patients)
- Oxygen long-term (hypoxemic patients)
- Pulmonary rehabilitation
- LVRS (selected emphysema)
- Transplant
10. CLINICAL PEARLS FROM HARRISON'S 22nd ED
| Scenario | Key Harrison's Teaching |
|---|---|
| COPD + digital clubbing | Investigate for lung cancer (not a COPD sign) |
| Normal/rising PCO₂ in breathless asthmatic | Warning of impending respiratory failure → prepare for intubation |
| Misdiagnosis in pneumonia | HCAP category discontinued - assess resistance risk individually |
| "Diuresed transudate" (CHF on diuretics) | Light's criteria gives false exudate → use SPAG to confirm transudate |
| IPF + immunosuppression | Harmful - increases morbidity/mortality; use antifibrotics instead |
| ARDS ventilation | 6 mL/kg tidal volume (not 12) - reduces mortality by ~9% |
| Chronic hypercapnic COPD at home | High-intensity BiPAP targets PaCO₂ <48 mmHg - improves 1-year mortality |
| LTBI preferred regimen 2024 | 3HP (weekly INH + rifapentine × 3 months) for all adults including HIV+ |
| SCLC staging | Limited vs. Extensive (not TNM); LD → chemoradiation + PCI |
| NSIP vs IPF | NSIP: symmetric ground-glass, subpleural sparing, 5-year survival >80%; IPF: honeycombing, basal, 50% die in 3-5 years |
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025), McGraw-Hill Medical - ISBN: 9781265977061
These are the full detailed notes from Harrison's across all major respiratory topics. Let me know if you want me to expand on any specific section - drug doses, GOLD staging tables, PE workup, sarcoidosis, pulmonary hypertension, sleep-disordered breathing, or any other topic.
This is a shared conversation. Sign in to Orris to start your own chat.