Hernia. Femoral hernia and umbilical , Para umbilical hernia
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple surgical textbooks. Let me compile a thorough answer.
Hernias: Femoral, Umbilical & Para-umbilical
1. FEMORAL HERNIA
Definition & Anatomy
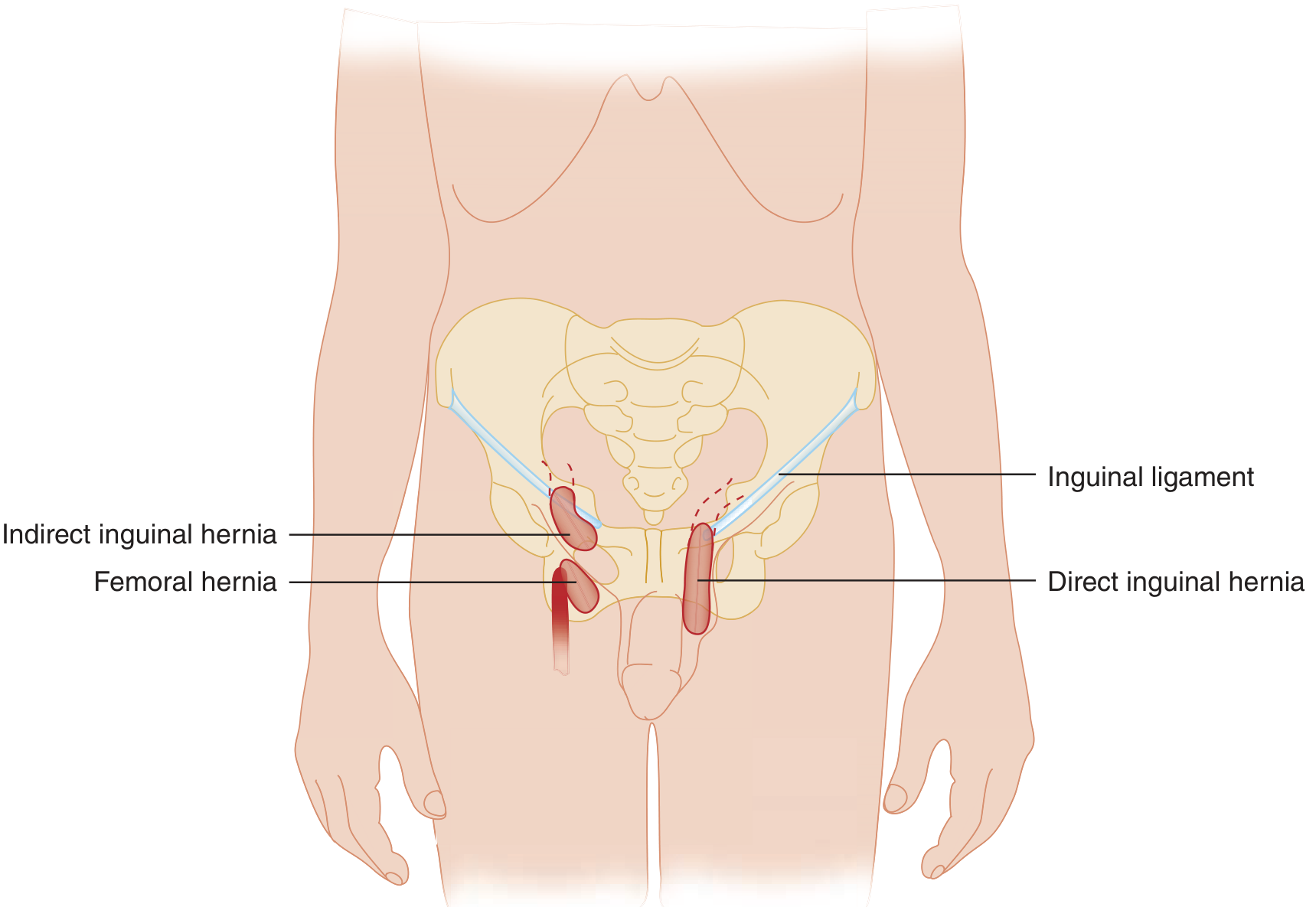
A femoral hernia occurs when the hernia sac protrudes through the femoral canal, producing a mass that lies below the inguinal ligament and medial to the femoral vein. It never enters the scrotum or labia.
Boundaries of the femoral ring (the entry point):
- Anteriorly: Inguinal ligament
- Posteriorly: Pectineus muscle and its fascia
- Medially: Lacunar ligament
- Laterally: Femoral vein
Path of the hernia sac:
- Enters the femoral ring → descends through the femoral canal
- Reaches the saphenous opening in the fascia lata
- Protrudes through, carrying the cribriform fascia with it
- Turns superiorly in the superficial fascia — may ascend above the inguinal ligament
Coverings (external → internal): skin → superficial fascia → cribriform fascia → femoral sheath → femoral septum → peritoneum
Epidemiology
- Accounts for 2–4% of groin hernia repairs
- Female predominance: ~10:1 female-to-male ratio (wider female pelvis)
- Usually acquired (not congenital); predominantly middle-aged and elderly
- In children, extremely rare (<0.5% of pediatric hernias)
Key Danger: High Complication Rate
Femoral hernias have a narrow femoral ring neck — this makes them highly prone to:
- Incarceration and strangulation
- One study reported a 40% emergency surgery rate in patients with known femoral hernias
- Strangulation rate reaches 45% at 21 months if repair is delayed
- Mortality ~13% from delayed repair
All femoral hernias should be urgently referred for elective repair — they cannot be watched safely.
Important Surgical Warning
The aberrant obturator artery (a large pubic branch of the inferior epigastric artery) may curve along the margin of the lacunar ligament. If cut during femoral hernia repair, it causes significant hemorrhage. This is sometimes called the "crown of death" or corona mortis.
Surgical Repair Options
| Approach | Description |
|---|---|
| Crural (lower) approach | Transverse incision over femoral triangle; hernia reduced from below the inguinal ligament; defect closed by suturing inguinal ligament to Cooper's ligament. Mesh plug may be used |
| Inguinal (McVay) approach | Posterior inguinal floor dissected; Cooper's ligament repair after reduction |
| Preperitoneal repair | Access via abdominal incision or laparoscopy; covers the entire myopectineal orifice — best for women per Swedish national register data |
| Lichtenstein modification | Mesh extended inferiorly as an inverted triangle sutured to Cooper's ligament covering the femoral space |
Preperitoneal mesh (open or laparoscopic) is the preferred approach for women with femoral hernias; the Swedish register showed much higher femoral recurrence in women after non-preperitoneal repair, often because a femoral hernia was misidentified as a direct inguinal hernia.
2. UMBILICAL HERNIA
Definition & Anatomy
Failure of the umbilical ring to close results in a fascial defect in the linea alba, allowing protrusion of abdominal contents covered by normal umbilical skin and subcutaneous tissue.
The umbilical ring normally closes after birth, reinforced by:
- Paired lateral umbilical ligaments (obliterated umbilical arteries)
- Round ligament (obliterated umbilical vein)
- Urachal remnant
- Transversalis fascia
Two Distinct Groups: Congenital (Pediatric) vs. Acquired (Adult)
Congenital / Pediatric Umbilical Hernia
- Most common abdominal wall defect in infants and children
- Incidence: 25–50% in Black infants, 4–9% in white infants in the first months of life
- Increased incidence in prematurity; familial tendency
- 80% close spontaneously by age 2, virtually all programmed to close
- Incarceration is rare (~1:1,500 cases)
Management (pediatric):
- Watchful waiting until age 2–3 years (spontaneous closure expected)
- Repair indicated if:
- Defect fails to close by age 5
- Large defect causing disfigurement or significant protrusion
- Any episode of incarceration
- Skin ulceration
Surgical technique (pediatric): Curved infraumbilical incision; sac dissected free; fascial defect closed with transverse, interrupted permanent or long-lasting absorbable sutures; subcuticular skin closure. Recurrence is rare.
Acquired (Adult) Umbilical Hernia
Predisposing factors:
- Multiple pregnancies
- Obesity
- Cirrhosis with ascites
- Large intra-abdominal tumors
- Male sex (peak incidence of repair ~age 60)
Differential diagnosis (important — do not confuse with):
- Caput medusae — periumbilical varicosities from portal hypertension (bluish, fill on straining)
- Sister Mary Joseph's nodule — umbilical metastasis of intra-abdominal cancer (hard nodule, biopsy diagnostic)
- Umbilical granuloma, epidermal inclusion cyst, urachal cyst, omphalomesenteric duct remnant
Surgical repair (adult):
- Defect <1–2 cm: primary suture repair (interrupted/figure-8, permanent or slow-absorbable); ~90% long-term success; Mayo "vest-over-pants" technique is classic but losing favor (tension creates recurrence risk)
- Defect >2 cm or recurrent: mesh repair — preperitoneal placement preferred; intraperitoneal (barrier-coated mesh) is an alternative but a recent multicenter RCT showed higher complications vs. preperitoneal mesh
- Laparoscopic/robotic approach increasingly used
Recurrence factors: High BMI, diabetes, smoking, large defect size
3. PARA-UMBILICAL HERNIA
Definition & Key Distinction from Umbilical Hernia
| Feature | Umbilical Hernia | Para-umbilical Hernia |
|---|---|---|
| Location | Through the umbilical ring itself | Adjacent to (not through) the umbilicus — in the linea alba immediately above or below the umbilicus |
| Age group | Congenital (infants) or acquired adults | Predominantly adults |
| Spontaneous closure | Yes (in children) | No — surgical treatment required |
| Neck | Variable | Often small neck → high strangulation risk |
Clinical Features
- Occurs in the midline in the epigastric–umbilical–hypogastric region (epigastric, umbilical/paraumbilical hernias form a spectrum)
- Para-umbilical hernias in adults occur at and around the umbilicus and often have small necks — requiring surgical treatment
- Higher risk of strangulation than congenital umbilical hernias due to the narrow neck
- Same predisposing factors as adult umbilical hernias (obesity, pregnancy, ascites)
Classification (Mulholland & Greenfield's Surgery)
Ventral abdominal wall hernias are classified as:
| Congenital | Omphalocele, Gastroschisis, Umbilical (infant) |
|---|---|
| Acquired midline — umbilical area | Umbilical (adult), Para-umbilical (adult, acquired) |
| EHS Classification (midline) | M3 = Umbilical |
Management
- All para-umbilical hernias in adults require surgery — spontaneous closure does not occur
- Repair technique mirrors adult umbilical hernia repair:
- Infraumbilical (or periumbilical) semilunar incision
- Sac dissected free; contents reduced
- For small defects: primary suture repair
- For larger or recurrent defects: mesh repair (preperitoneal preferred)
- Laparoscopic/robotic approach: 3 ports placed lateral to the semilunar line for robotic preperitoneal midline hernia repair
Quick Comparison Summary
| Feature | Femoral Hernia | Umbilical Hernia | Para-umbilical Hernia |
|---|---|---|---|
| Location | Below inguinal ligament, through femoral canal | Through umbilical ring | Adjacent to umbilicus in linea alba |
| Gender predilection | Female (10:1) | Male (adult peak ~60 yrs) | Adults, any gender |
| Spontaneous closure | No | Yes (children <5 yrs) | No |
| Complication risk | Very high (narrow neck) | Low in children | Moderate–high (small neck) |
| Emergency surgery rate | ~40% | Rare in children | Moderate |
| Key surgical risk | Aberrant obturator artery | — | Small neck → strangulation |
| Preferred repair | Preperitoneal mesh (women) | Suture <2 cm; mesh >2 cm | Mesh for larger defects |
Sources: Mulholland and Greenfield's Surgery 7e; Gray's Anatomy for Students; Tintinalli's Emergency Medicine; Schwartz's Principles of Surgery 11e
This is a shared conversation. Sign in to Orris to start your own chat.