Olliers disease etiology pathology signs and symptoms course of disease investigation and treatment explain in detail with appropriate illustrative diagrams
Reading File
Finding Sources
Finding Sources
Searching the Web
Ollier disease enchondromatosis etiology pathology signs symptoms treatment 2024
Searching Images
Ollier disease enchondromatosis radiograph pathology
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Searching Images
enchondroma histopathology hyaline cartilage microscopy
Finding Sources
Finding Sources
Loading Image
Loading Image
Searching PubMed
Ollier disease enchondromatosis IDH mutation management
I now have comprehensive data. Let me compile the full, detailed answer.
Ollier Disease (Multiple Enchondromatosis / Dyschondroplasia)
Overview
Ollier disease is a non-hereditary, sporadic skeletal dysplasia characterised by multiple enchondromas — benign cartilaginous tumours arising from the medullary canal of bone. It was first described by the French surgeon Louis Xavier Édouard Léopold Ollier in 1889, who reported limb deformity related to abnormal cartilage growth. The condition is classified as Spranger type I multiple enchondromatosis.
| Feature | Detail |
|---|---|
| Prevalence | ~1 in 100,000 |
| Sex | Males > Females (2:1) |
| Inheritance | Sporadic (non-hereditary) |
| Onset | Childhood (age 1–4 years typically) |
1. Etiology & Molecular Pathogenesis
Ollier disease is caused by somatic mosaic mutations in the IDH1 and IDH2 genes (isocitrate dehydrogenase 1 and 2) (Goldman-Cecil Medicine). Because the mutation is somatic (post-zygotic) and mosaic (affecting only a subset of cells), the condition is:
- Not inherited — it arises de novo during embryogenesis
- Unilateral or asymmetric — reflecting the mosaic distribution of mutant clones
- Variable in severity — depending on when in development the mutation occurred
Mechanism
The normal IDH1/IDH2 enzymes convert isocitrate to α-ketoglutarate. The mutant enzymes instead produce the oncometabolite 2-hydroxyglutarate (2-HG), which:
- Inhibits α-ketoglutarate–dependent enzymes (including histone and DNA demethylases)
- Causes global hypermethylation of histones and CpG islands
- Blocks normal differentiation of chondrocytes — particularly failure of resorption of primary growth plate cartilage
- Leads to accumulation of chondrocytic rests within the medullary canal
"Ollier disease is caused by somatic mosaic mutations in the IDH1 and IDH2 genes. The disease begins with localized swelling in childhood and interferes with linear bone growth." — Goldman-Cecil Medicine
"It is a disorder of the growth plate in which the primary cartilage is not resorbed. Cartilage ossification proceeds normally, but it is not resorbed normally, leading to cartilage accumulation." — Harrison's Principles of Internal Medicine, 22e
2. Pathology
Gross Pathology
Enchondromas are lobulated, translucent, blue-grey nodules of hyaline cartilage within the medullary cavity. They arise from displaced growth-plate cartilage and localize within trabecular bone. The bones are dysplastic and the lesions tend toward unilaterality.
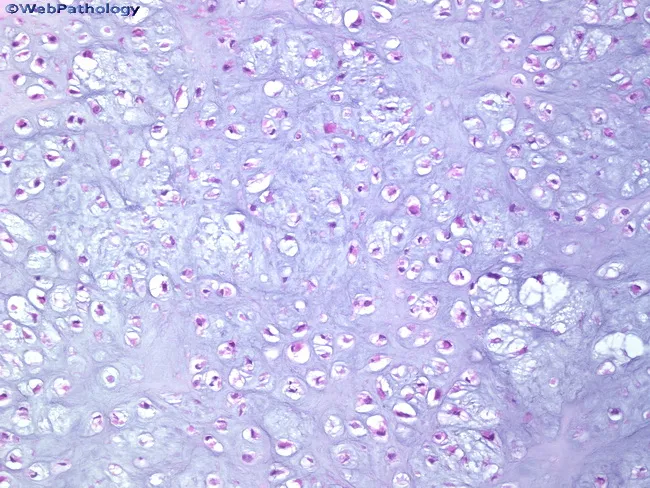
Histopathology
On H&E staining, enchondromas show:
- Lobulated hyaline cartilage matrix (bluish-purple, basophilic)
- Chondrocytes in lacunae — small, round-to-oval with regular nuclei
- Cells occur singly or in small clusters separated by fibrous septa
- Low cellularity, minimal atypia, rare mitoses
- Peripheral endochondral ossification and calcification
Key distinction from chondrosarcoma: Benign enchondromas are well-circumscribed and do not permeate or invade surrounding bony trabeculae. Infiltrative growth (invasion into cortex, marrow permeation) signals malignant transformation.
Radiological Pathology
- Enchondromas appear as lucent (lytic) defects in the metaphyses/diaphyses of tubular bones and flat bones
- Central calcific stippling (punctate calcification) is a hallmark
- Vertical lucent streaks (cartilage columns) in the metaphysis
- Bones become widened, shortened, and deformed due to cartilage expansion
3. Signs and Symptoms
Clinical Features (by system)
Skeletal — Primary manifestations:
| Feature | Description |
|---|---|
| Limb deformity | Bowing of long bones (tibia, fibula, femur, radius, ulna) |
| Limb length discrepancy (LLD) | Asymmetric shortening — causes limp if unilateral; short stature if bilateral |
| Swelling/masses | Hard, painless bony swellings — most common over hands (metacarpals, phalanges) |
| Pathological fractures | Through weakened, lesion-containing bone |
| Short stature | If both lower limbs are significantly affected |
| Scoliosis / pelvic deformity | If spine or pelvis is involved (less common) |
Distribution:
- Classically asymmetric / unilateral (reflects mosaic mutation)
- Most frequent sites: phalanges and metacarpals (hands), followed by long bones (femur, tibia, humerus, radius)
- Pelvis, ribs, sternum, skull: rarely affected
Maffucci Syndrome (variant): When enchondromas coexist with soft tissue hemangiomas and lymphangiomas, the diagnosis is Maffucci syndrome — a related but distinct condition with a much higher malignancy risk.
4. Course of Disease (Natural History)
Childhood
- Lesions first appear in early childhood (1–4 years)
- Progressive growth of enchondromas during skeletal development
- Increasing limb deformity, shortening, and pathological fractures
Puberty / Skeletal Maturity
- After growth plate closure at puberty, cartilaginous masses stop expanding
- Lesions may be replaced by mature bone (ossification)
- Deformities stabilise but do not resolve spontaneously
Malignant Transformation (Major Long-Term Complication)
This is the most feared complication. Risk varies:
| Condition | Risk of Malignancy |
|---|---|
| Ollier disease | 25–30% (some sources cite 5–50% range) |
| Maffucci syndrome | ~50–100% |
- Most common malignancy: Secondary chondrosarcoma (especially pelvis, shoulder, distal femur, proximal tibia)
- Enchondromas in the hands rarely transform to chondrosarcoma
- Chondrosarcoma invades locally, recurs locally, and can metastasise (usually to lungs)
- Additional malignancies associated with IDH mutations: gliomas (brain), granulosa cell tumours of ovary, gastrointestinal malignancies, acute myeloid leukaemia
Warning signs of malignant transformation:
- New or increasing pain in a previously painless lesion
- Rapid increase in size after skeletal maturity
- Cortical thinning or breach on imaging
- Soft tissue extension
5. Radiological Images
Lateral Radiograph — Lower Limb Bowing and Multiple Enchondromas

Lateral X-ray of left lower limb: Multiple radiolucent lesions with bowing deformity of the long bones. Expansile lytic lesions with internal punctate calcifications are visible at the metaphyses of the femur, tibia and fibula.
AP Radiograph — Bilateral Lower Limbs Post-Surgical Correction

AP radiograph: Bilateral lower limbs showing irregular radiolucencies and radiopacities characteristic of multiple enchondromas. Limb lengths appear symmetrical following deformity correction surgery.
Radiograph — Surgical Management with External Fixator
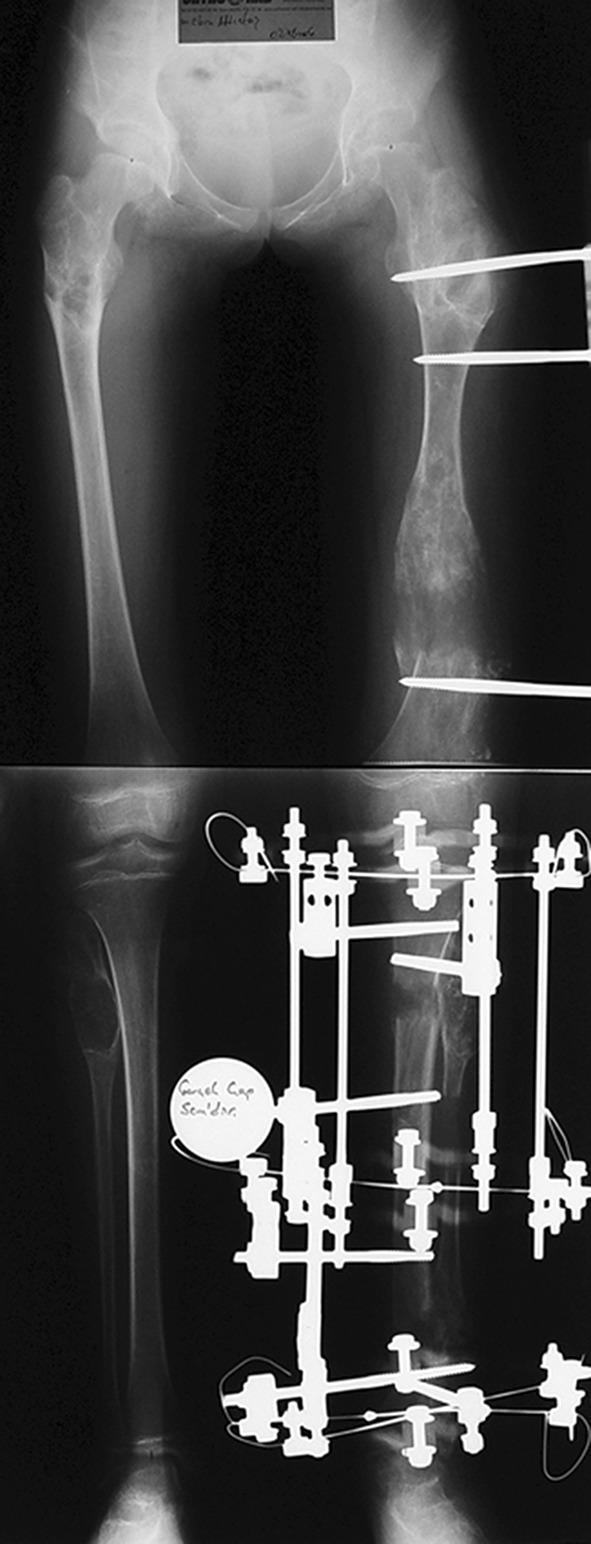
AP pelvis and bilateral femurs: Multiple radiolucent enchondromatous lesions causing bone dysplasia. An external fixator (Ilizarov-type) is applied to one femur for distraction osteogenesis (limb lengthening) and angular correction.
Ankle X-ray — Metaphyseal Enchondroma Features

Ankle AP X-ray: Multiple linear lucencies and vertical striations at the distal tibial metaphysis, irregular growth plates, and altered joint stress — classic features of metaphyseal enchondromatosis.
Multi-modal Imaging — IDH-Mutant Syndrome (Ollier + Brain Glioma)
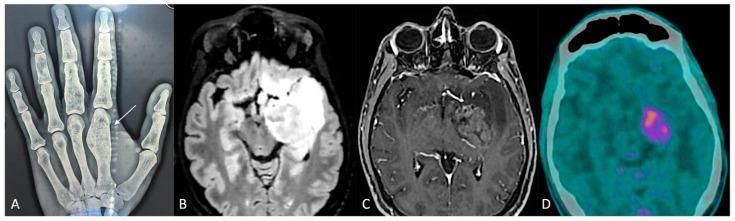
Panel A: PA hand X-ray showing expansile lucent enchondromas (arrow at first metacarpal). Panels B–D: Brain MRI and PET-CT showing malignant glioma — illustrating the IDH-mutant link between skeletal enchondromatosis and CNS malignancy.
6. Investigations
Imaging
| Modality | Findings |
|---|---|
| Plain X-ray (first-line) | Lytic lesions with central calcific stippling; metaphyseal vertical striations; bone shortening/bowing; well-defined sclerotic margins |
| MRI | Best for soft tissue detail, marrow involvement, cortical breach; helps distinguish benign from malignant transformation; low signal on T1, high on T2 (chondroid matrix) |
| CT scan | Better definition of matrix calcification, cortical integrity, and extent |
| Bone scintigraphy (Tc-99m) | Screens for malignant transformation (increased uptake); maps all skeletal lesions |
| PET-CT | Metabolic hyperactivity confirms malignant transformation |
Histopathology / Biopsy
- Performed when malignant transformation is suspected
- Core needle or open biopsy
- H&E staining shows hyaline cartilage lobules with chondrocytes in lacunae
- Look for permeative growth pattern, cortical invasion, mitotic activity (suggests chondrosarcoma)
Molecular / Genetic
- IDH1/IDH2 mutation analysis (tissue) — confirms diagnosis and relates to malignancy risk
- Helpful when distinguishing from hereditary multiple exostoses (EXT1/EXT2 mutations) or fibrous dysplasia (GNAS mutations)
Laboratory
- Routine bloods (FBC, CMP) — generally normal
- No specific serum markers for Ollier disease
- Elevated alkaline phosphatase may suggest active bone turnover
7. Treatment
Treatment is largely conservative unless lesions are symptomatic or complications arise. There is no medical therapy that reverses the enchondromas.
Conservative Management
- Observation — for asymptomatic lesions with classic radiographic appearances
- Physiotherapy — to maintain range of motion and muscle strength
- Orthotics — shoe lifts for mild limb length discrepancy
Surgical Management
| Indication | Procedure |
|---|---|
| Symptomatic enchondroma (pain, fracture risk) | Curettage + bone grafting (autograft or allograft) |
| Pathological fracture | Internal fixation ± curettage |
| Angular deformity | Corrective osteotomy ± internal fixation |
| Limb length discrepancy | Distraction osteogenesis (Ilizarov / Taylor Spatial Frame); epiphysiodesis of contralateral limb |
| Malignant transformation → Chondrosarcoma | Wide surgical resection with clear margins; limb-sparing surgery preferred; adjuvant chemotherapy/radiation have limited efficacy in conventional chondrosarcoma |
"Most common surgical treatments include curettage and bone grafting, internal fixation, or treatment for angular deformity or limb length discrepancy." — POSNA Study Guide
Surveillance (Critical)
Given the 25–30% lifetime risk of malignant transformation:
- Regular clinical follow-up — every 1–2 years (or more frequently in childhood)
- Serial plain radiographs — annual for known lesions
- Bone scintigraphy — to screen for new or transformed lesions
- MRI / CT — for any lesion showing new pain, rapid growth, or suspicious features
- Biopsy — for any lesion suspected of chondrosarcomatous change
IDH-Inhibitor Therapy (Emerging)
Based on the IDH1/IDH2 mutation basis of the disease, IDH inhibitors (enasidenib, ivosidenib) are used in IDH-mutant AML and are under investigation for IDH-mutant chondrosarcomas. Recent 2024 review identified IDH as the common denominator linking Ollier disease, AML, and brain glioma — opening new therapeutic avenues.
8. Comparison: Ollier Disease vs. Maffucci Syndrome
| Feature | Ollier Disease | Maffucci Syndrome |
|---|---|---|
| Enchondromas | ✓ | ✓ |
| Soft tissue hemangiomas | ✗ | ✓ |
| Inheritance | Sporadic | Sporadic |
| IDH1/IDH2 mutation | ✓ | ✓ |
| Malignancy risk | ~25–30% | ~50–100% |
| Visceral malignancies | Less common | AML, glioma, GI, ovarian |
9. Differential Diagnosis
| Condition | Key Distinguishing Feature |
|---|---|
| Solitary enchondroma | Single lesion; no dysplasia or limb deformity |
| Hereditary multiple exostoses | Exostoses (surface lesions); autosomal dominant; EXT1/EXT2 mutations |
| Fibrous dysplasia | Ground-glass matrix (not chondroid); GNAS mutation; McCune-Albright syndrome if polyostotic + café-au-lait |
| Chondrosarcoma | Pain, cortical breach, permeative growth on histology |
| Metachondromatosis | Both exostoses and enchondromas; PTPN11 mutation; autosomal dominant |
Key References
- Goldman-Cecil Medicine International Edition — Enchondromatosis (Dyschondroplasia, Ollier Disease)
- Harrison's Principles of Internal Medicine, 22e — Enchondromatosis
- Miller's Review of Orthopaedics, 9th Edition — Ollier Disease/Maffucci Syndrome
- Bailey & Love's Short Practice of Surgery, 28th Edition — Enchondromatosis
- Corvino S et al. "Ollier Disease, Acute Myeloid Leukemia, and Brain Glioma: IDH as the Common Denominator." Cancers (Basel), 2024 — PMID: 39335096
This is a shared conversation. Sign in to Orris to start your own chat.