Give me in detail explanation of cardiovascular system examination with which conditions contain which type of signs and symptoms in order wise and differentiation between diseases if any diseases are similar
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the content needed to write a comprehensive, detailed answer. Let me compile everything.
Cardiovascular System Examination - Complete Guide
Sources: Harrison's Principles of Internal Medicine 22E (2025), Goldman-Cecil Medicine
ORDER OF EXAMINATION
The cardiovascular exam follows a structured sequence:
- General Appearance
- Vital Signs (BP, HR, RR)
- Ophthalmologic Exam
- Jugular Venous Pressure (JVP)
- Carotid Pulse
- Precordial Inspection and Palpation
- Cardiac Auscultation
- Abdominal and Peripheral Exam
1. GENERAL APPEARANCE
Before touching the patient, observe for features pointing to specific diagnoses:
| Finding | Associated Condition |
|---|---|
| Tachypnea, labored breathing | Heart failure, pulmonary edema |
| Cheyne-Stokes respirations | Advanced heart failure |
| Exophthalmos, stare | Hyperthyroidism (atrial fibrillation, high-output failure) |
| Ptosis, expressionless face | Myotonic dystrophy (AV block, arrhythmia) |
| Tall, thin build with arm span > height | Marfan syndrome (aortic root dilation, MVP) |
| Blue sclerae | Osteogenesis imperfecta (aortic dilation, MVP) |
| Webbed neck, low hairline | Turner syndrome (coarctation, bicuspid aortic valve) |
| Short stature, flat face | Down syndrome (ASD, VSD, AV canal) |
| Malar rash, joint swelling | SLE, rheumatoid arthritis (pericarditis, endocarditis) |
| Tight skin, sclerodactyly | Scleroderma (pulmonary hypertension) |
| Skin bronzing | Hemochromatosis (cardiomyopathy, heart block) |
2. VITAL SIGNS
Blood Pressure
Technique: Seated, arm at heart level, 5-10 min rest, appropriately sized cuff. Cuff bladder length 80%, width 40% of arm circumference.
| BP Finding | Interpretation |
|---|---|
| BP difference >10 mmHg between arms | Subclavian artery atherosclerosis/inflammation, aortic dissection, supravalvular aortic stenosis, coarctation |
| Arm BP >> leg BP | Normal: leg systolic is ~20 mmHg higher; reversed ratio suggests coarctation of the aorta |
| Very low diastolic (near 0) | Chronic severe aortic regurgitation (AR) or large arteriovenous fistula |
| Wide pulse pressure | Severe AR, hyperthyroidism, fever, anemia, high-output states |
| Narrow pulse pressure | Severe aortic stenosis (AS), cardiac tamponade, severe LV dysfunction |
Pulsus Paradoxus
A fall in systolic BP >10 mmHg with inspiration.
| Cause | Key Distinguishing Feature |
|---|---|
| Pericardial tamponade | Most classic cause; also has elevated JVP, muffled heart sounds |
| Massive pulmonary embolism | Tachycardia, hypoxia, pleuritic chest pain |
| Severe obstructive lung disease | Wheeze, prolonged expiratory phase |
| Tension pneumothorax | Absent breath sounds, tracheal deviation |
| Hemorrhagic shock | Hypotension, bleeding source |
Pulsus Alternans
Beat-to-beat variability of pulse amplitude at regular rhythm. Indicates severe LV systolic dysfunction. Every other Korotkoff sound is audible as cuff deflates.
3. OPHTHALMOLOGIC EXAM
| Finding | Associated Condition |
|---|---|
| Diabetic retinopathy | Ischemic cardiomyopathy |
| Hypertensive retinopathy | Hypertensive heart disease, LVH |
| Roth spots (white-centered hemorrhages) | Infective endocarditis |
| Beading of retinal arteries | Severe hypercholesterolemia |
| Retinal artery occlusion | Embolus from left atrial thrombus, myxoma, aortic atheroembolism |
4. JUGULAR VENOUS PRESSURE (JVP)
Measurement: Vertical distance from sternal angle (angle of Louis) to top of jugular pulsation at 30-45 degrees. Normal <4.5 cm at 30°; add 5 cm to get central venous pressure in cm H₂O. Normal CVP = 5-10 cm H₂O. Pulsations above the clavicle in the sitting position are always abnormal.
Distinguishing JVP from carotid:
- JVP: biphasic (two peaks), not palpable, changes with posture and respiration
- Carotid: monophasic, palpable, does not change with respiration
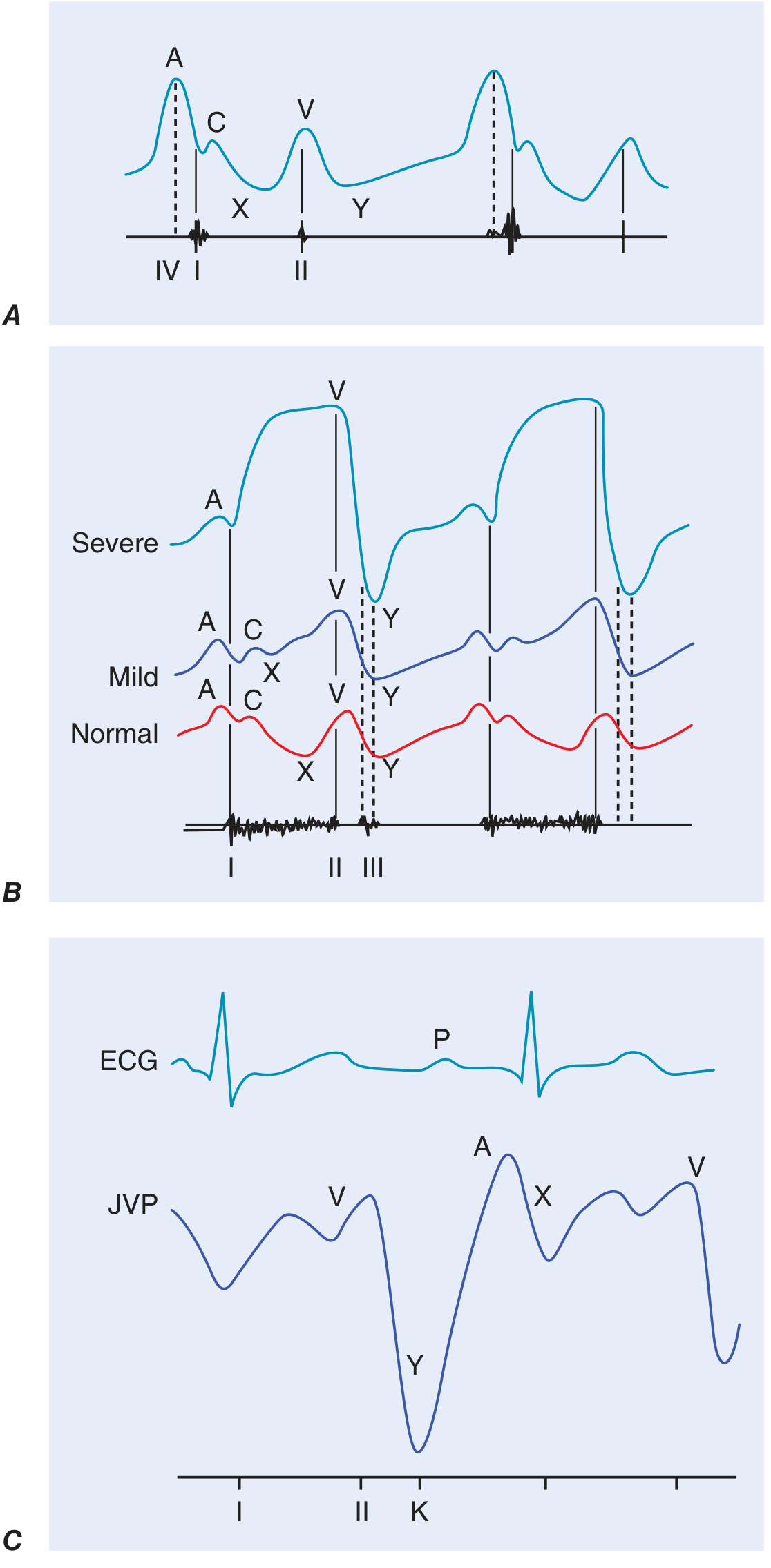
JVP Waveform Components and Their Abnormalities
| Wave/Descent | Normal Meaning | Abnormality | Disease |
|---|---|---|---|
| a wave | RA presystolic contraction (after P wave, before S1) | Prominent a wave | Reduced RV compliance (pulmonic stenosis, pulmonary hypertension, RV hypertrophy) |
| Cannon a wave | AV dissociation (VT, complete heart block) - RA contracts against closed tricuspid valve | ||
| Absent a wave | Atrial fibrillation | ||
| x descent | Fall in RA pressure after tricuspid opening | Absent/blunted | Atrial fibrillation, tamponade |
| v wave | Atrial filling during ventricular systole | Accentuated v wave (cv wave) | Tricuspid regurgitation - waveform becomes "ventriculized" |
| y descent | After v peak, tricuspid valve opens | Blunted/prolonged y descent | Tricuspid stenosis, pericardial tamponade |
| Rapid, prominent y descent | Constrictive pericarditis, severe TR |
Elevated JVP: Differential Diagnosis
| JVP Pattern | Diagnosis |
|---|---|
| Elevated JVP + blunted/absent y descent + pulsus paradoxus + quiet heart | Cardiac tamponade - echocardiography urgently needed |
| Elevated JVP + sharp prominent y descent + Kussmaul sign + quiet precordium | Constrictive pericarditis - CT/MRI/catheterization needed |
| Elevated JVP + sharp brief y descent + Kussmaul sign + evidence of pulmonary hypertension + TR | Restrictive cardiomyopathy |
| Elevated JVP without y descent | Right heart failure of any cause |
| Prominent a wave (no elevated mean JVP) | Tricuspid stenosis, pulmonic stenosis, pulmonary hypertension |
| Prominent v wave + sharp y descent | Tricuspid regurgitation |
Kussmaul's sign (JVP rises or fails to fall with inspiration): Constrictive pericarditis (classic), restrictive cardiomyopathy, massive PE, RV infarction, advanced LV systolic failure.
Abdominojugular (hepatojugular) reflux: Firm pressure over RUQ for >15 seconds; positive = sustained JVP rise >3 cm. Indicates volume-overloaded state; predicts pulmonary artery wedge pressure >15 mmHg in heart failure.
5. CAROTID PULSE (CHARACTER OF PULSE)
Best assessed at the carotid artery. Describes pulse volume and contour.
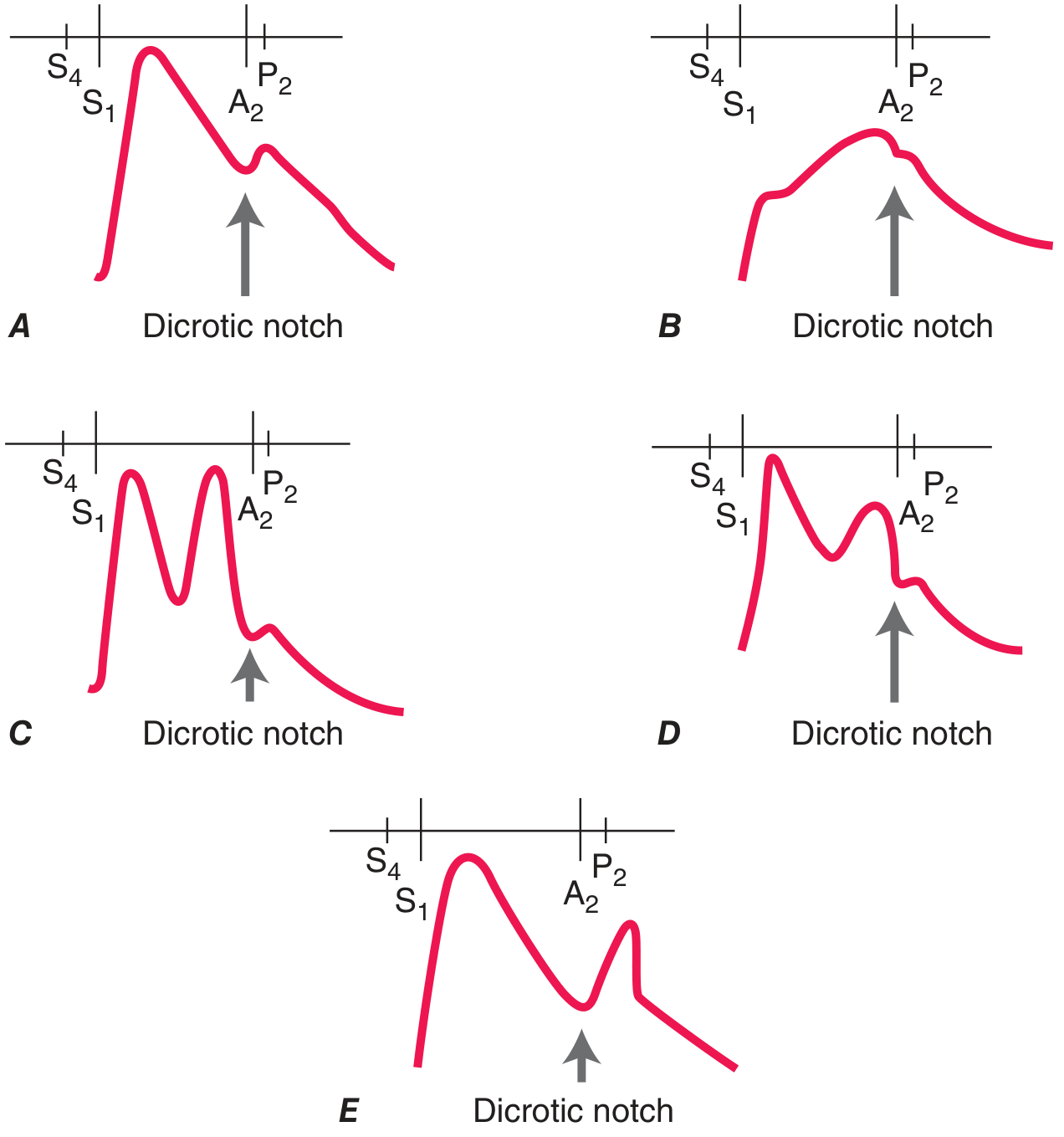
| Pulse Character | Description | Disease(s) |
|---|---|---|
| Pulsus parvus et tardus | Weak, delayed upstroke to a small peak | Severe Aortic Stenosis |
| Anacrotic pulse | Slow notched upstroke, peak near S2 | Severe Aortic Stenosis |
| Corrigan's (water-hammer) pulse | Sharp rapid rise, collapsing fall | Chronic severe Aortic Regurgitation |
| Bisferiens pulse (two systolic peaks) | Percussion wave + tidal wave | Severe AR; HOCM; combined AS+AR with dominant AR |
| Dicrotic pulse (one systolic + one diastolic peak) | Exaggerated dicrotic wave | Sepsis, severe heart failure, hypovolemic shock, tamponade, after AVR |
| Hyperkinetic pulse | Increased amplitude and frequency | AR, AV fistula, hyperthyroidism, fever, anemia |
| Normal contour, reduced amplitude | Normal shape but weak | Any cause of reduced stroke volume |
Differentiating Aortic Stenosis vs Aortic Regurgitation by Pulse
| Feature | Aortic Stenosis | Aortic Regurgitation |
|---|---|---|
| Pulse character | Parvus et tardus (weak, delayed) | Water-hammer (sharp rise, collapsing) |
| Pulse pressure | Narrow | Wide |
| BP diastolic | Normal/elevated | Low (near 0 in severe) |
| Systolic murmur | Ejection (crescendo-decrescendo), midsystolic | None (unless combined lesion) |
| Diastolic murmur | None | Decrescendo, high-pitched, early diastolic |
6. PRECORDIAL INSPECTION AND PALPATION
Inspection
| Finding | Meaning |
|---|---|
| Visible apex beat at 5th ICS mid-clavicular line | Normal in thin adults |
| Apex beat displaced leftward/downward | LV enlargement |
| Visible sternal/parasternal pulsation | RV enlargement |
| Right upper parasternal pulsation | Ascending aortic aneurysm |
| Epigastric pulsation | Cardiac impulse displaced (COPD, emphysema) vs. pulsatile liver |
| Unilateral left chest asymmetry | RV hypertrophy developing before puberty |
Palpation (Technique: supine at 30°, left lateral decubitus to enhance)
| Finding | Meaning | Disease |
|---|---|---|
| Normal apex (<2 cm, brief outward movement) | Normal LV | - |
| Sustained (heaving) apex | Pressure overload | AS, chronic hypertension |
| Displaced, enlarged apex | Volume overload + LV dilation | Severe MR, severe AR, DCM |
| Palpable S4 (presystolic impulse) | Reduced LV compliance | LV hypertrophy, active ischemia, AS |
| Palpable S3 | Rapid early filling (advanced HF) | Dilated cardiomyopathy, severe MR |
| Ectopic dyskinetic impulse (separate from apex) | LV aneurysm | Post-MI aneurysm |
| Triple cadence at apex (S4 + bisferiens) | Very rare | HOCM |
| Sternal/parasternal lift | RV pressure or volume overload | Pulmonary hypertension, RV failure, ASD |
| Loud palpable P2 | Pulmonary hypertension | |
| Systolic thrill | Turbulent flow | Grade ≥4 murmur: severe AS, VSD, MR |
| Diastolic thrill | Turbulent diastolic flow | Severe MS |
7. CARDIAC AUSCULTATION
Heart Sounds
First Heart Sound (S1)
Produced by mitral and tricuspid valve closure.
| S1 Character | Disease |
|---|---|
| Loud S1 | Early rheumatic mitral stenosis (leaflets pliable but narrowed), hyperkinetic states, short PR interval |
| Soft S1 | Late MS (leaflets rigid/calcified), after beta-blockers, long PR interval, LV contractile dysfunction |
| Variable S1 | Complete AV block, atrial fibrillation |
| Wide splitting of S1 | RBBB (delayed tricuspid closure) |
Second Heart Sound (S2)
A2 (aortic closure) + P2 (pulmonic closure). Normally A2 before P2. Splitting increases with inspiration.
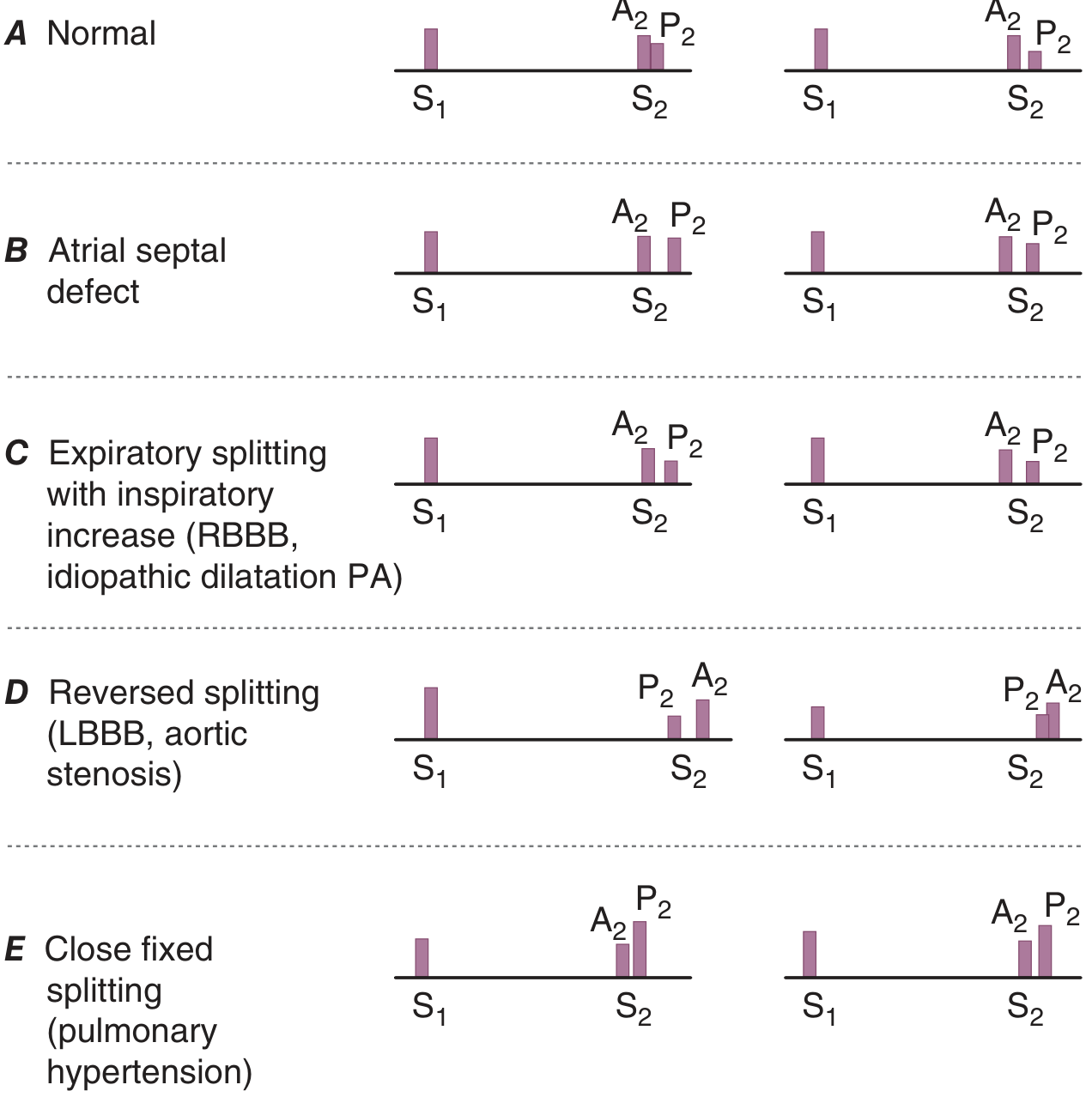
| S2 Pattern | Cause | Disease |
|---|---|---|
| Fixed splitting (A2-P2 gap same in inspiration and expiration) | Equalization of RV/LV filling | Atrial Septal Defect (ASD) |
| Wide splitting (physiologic, inspiratory increase) | Delayed P2 | RBBB, idiopathic PA dilation |
| Paradoxical (reversed) splitting (splits on expiration, closes on inspiration) | Delayed A2 | LBBB, severe AS (mechanical delay), HOCM |
| Close fixed splitting | Loud P2 + fixed gap | Pulmonary hypertension |
| Single S2 | Only one valve audible | Severe AS (A2 absent/inaudible), severe pulmonary hypertension (P2 overwhelms A2) |
| Loud A2 | Increased aortic pressure | Systemic hypertension |
| Soft A2 | Reduced aortic valve excursion | Aortic stenosis |
| Loud P2 | Increased pulmonary artery pressure | Pulmonary hypertension, large ASD |
Third Heart Sound (S3) - Early Diastolic Gallop
Low-pitched sound after S2, in early diastole (rapid ventricular filling phase).
| Context | Significance |
|---|---|
| In patient <40 years | Often normal (physiologic) |
| In adults with dyspnea + dilated LV | LV systolic failure - high sensitivity for elevated wedge pressure |
| After MR | Chronic severe Mitral Regurgitation |
| Right-sided S3 (louder with inspiration) | RV failure, severe TR |
Fourth Heart Sound (S4) - Presystolic Gallop
Low-pitched sound before S1 (late diastole), due to atrial contraction into non-compliant ventricle. Not present with atrial fibrillation.
| Cause | Disease |
|---|---|
| Reduced LV compliance | LV hypertrophy, hypertensive heart disease, AS |
| Active myocardial ischemia | Acute MI, angina |
| Hypertrophic cardiomyopathy | HOCM |
| Right-sided S4 | RV hypertrophy (pulmonary hypertension, pulmonic stenosis) |
Differentiating S3 vs S4
| Feature | S3 | S4 |
|---|---|---|
| Timing | Early diastole (after S2) | Late diastole (before S1) |
| Mechanism | Rapid filling into diseased ventricle | Atrial kick into non-compliant ventricle |
| Present in AF | Yes | NO |
| Implies | LV systolic dysfunction / volume overload | Reduced compliance / pressure overload |
| Pitch | Low (bell) | Low (bell) |
Additional Sounds
| Sound | Timing | Disease |
|---|---|---|
| Ejection click (early systolic) | Just after S1 | Bicuspid aortic valve, mobile aortic valve in congenital AS; pulmonic valve stenosis (click disappears with inspiration); pulmonary hypertension with forceful valve opening |
| Mid-late systolic click | Variable during systole | Mitral Valve Prolapse (MVP) - moves toward S1 with standing/Valsalva; moves toward S2 with squatting |
| Opening snap (OS) | Early diastole (after A2) | Mitral Stenosis - shorter A2-OS interval = more severe MS |
| Pericardial knock | Early diastole | Constrictive pericarditis - high-pitched, occurs at the nadir of Y descent |
| Tumor plop | Early diastole | Atrial myxoma (movement of tumor through mitral valve) |
| Pericardial friction rub | Two or three component (systolic + diastolic) scratching sound | Pericarditis - best heard with patient leaning forward; may disappear with effusion |
Heart Murmurs
Graded 1-6 (thrill present at grade 4+).
SYSTOLIC MURMURS
Holosystolic (Pansystolic) Murmurs
Persist throughout systole (S1 to S2), flat or decrescendo.
| Disease | Location | Radiation | Character | Key Signs |
|---|---|---|---|---|
| Mitral Regurgitation (MR) | Apex | Left axilla (anterior leaflet to back; posterior leaflet to base - can mimic AS) | Holosystolic blowing | Displaced apex, S3, reduced S1 |
| Tricuspid Regurgitation (TR) | Left lower sternal border | None | Holosystolic, increases with inspiration (Carvallo sign) | CV waves in JVP, pulsatile liver, peripheral edema |
| Ventricular Septal Defect (VSD) | Left sternal border 3rd-4th ICS | Right sternal border | Holosystolic harsh | Thrill common; if large: signs of pulmonary hypertension |
Midsystolic (Ejection) Murmurs
Crescendo-decrescendo, begin after S1, end before S2.
| Disease | Location | Radiation | Key Signs | Differentiation |
|---|---|---|---|---|
| Aortic Stenosis (AS) | Right 2nd ICS (aortic area) | Carotids (Gallavardin - to apex, can mimic MR) | Parvus et tardus pulse, sustained apex, soft/absent A2, paradoxical S2 split, S4 | Late-peaking murmur = more severe |
| Pulmonary Stenosis | Left 2nd ICS (pulmonic area) | Left shoulder | Loud P2 if mild (soft if severe), ejection click (decreases with inspiration) | Right-sided signs; no carotid radiation |
| Hypertrophic Obstructive Cardiomyopathy (HOCM) | Left lower sternal border | Does NOT radiate to carotids well | Bisferiens pulse, S4, dynamic murmur | Increases with Valsalva/standing; decreases with squatting/hand-grip |
| ASD (relative pulmonic stenosis) | Left 2nd ICS | - | Fixed split S2 | Soft murmur (flow); fixed S2 splitting |
| Benign flow murmur | Left sternal border/pulmonary area | None | No abnormal signs | Grade 1-2, vibratory (Still's murmur in children) |
Differentiating AS vs MR vs HOCM (all are systolic murmurs)
| Feature | AS | MR | HOCM |
|---|---|---|---|
| Timing | Midsystolic (ejection) | Holosystolic | Mid-late systolic |
| Location | Right 2nd ICS | Apex | Left lower sternal border |
| Radiation | Carotids | Axilla | Not carotids |
| Pulse | Parvus et tardus | Normal or hyperdynamic | Bisferiens |
| S2 | Soft A2, paradoxical split | Wide physiologic split (early A2) | Normal |
| Valsalva | Decreases | Decreases | Increases |
| Squatting | Increases | Increases | Decreases |
| Standing | Decreases | Decreases | Increases |
| Handgrip | Increases | Increases | Decreases |
Late Systolic Murmur
| Disease | Feature |
|---|---|
| Mitral Valve Prolapse | Preceded by mid-systolic click; click-murmur complex moves toward S1 with standing/Valsalva; moves toward S2 with squatting |
DIASTOLIC MURMURS (always pathological)
Early Diastolic (Decrescendo)
| Disease | Location | Radiation | Quality | Key Signs |
|---|---|---|---|---|
| Aortic Regurgitation (AR) | Left sternal border (3rd ICS), also right 2nd ICS if aortic root dilated | Apex | High-pitched blowing decrescendo; best heard with patient sitting forward | Water-hammer pulse, wide pulse pressure, Austin Flint murmur (mid-diastolic low-pitched rumble at apex in severe AR), displaced apex, S3 |
| Pulmonary Regurgitation (Graham Steell murmur) | Left 2nd-3rd ICS | - | High-pitched decrescendo | Loud P2, signs of pulmonary hypertension |
Mid-Diastolic (Rumbling)
| Disease | Location | Radiation | Quality | Key Clues |
|---|---|---|---|---|
| Mitral Stenosis (MS) | Apex | None | Low-pitched rumble (use bell); follows opening snap | Loud S1, OS, shorter A2-OS interval = more severe; pre-systolic accentuation in sinus rhythm; AF eliminates presystolic component |
| Tricuspid Stenosis | Left lower sternal border | None | Rumble; increases with inspiration | Prominent a wave in JVP, hepatomegaly |
| Austin Flint murmur | Apex | None | Low-pitched rumble | In context of severe AR; no OS; no loud S1 |
Differentiating MS vs Austin Flint Murmur
| Feature | Mitral Stenosis | Austin Flint (AR) |
|---|---|---|
| Opening snap | Present | Absent |
| S1 | Loud (early), soft (late) | Normal or soft |
| AR signs | Absent | Present (water-hammer pulse, wide PP) |
| Response to amyl nitrite | Louder (MS) | Softer (Flint - less AR) |
CONTINUOUS MURMURS (systole + diastole)
| Cause | Feature |
|---|---|
| Patent Ductus Arteriosus (PDA) | Left infraclavicular area; "machinery" murmur; wide pulse pressure |
| Ruptured sinus of Valsalva aneurysm | Sudden onset, may have thrill |
| Arteriovenous fistula | Over fistula site |
| Mammary souffle | Over breast in pregnancy |
| Combined AS + AR | Can mimic continuous; two separate murmurs |
8. ABDOMINAL AND PERIPHERAL EXAMINATION
| Finding | Disease |
|---|---|
| Hepatomegaly | Right heart failure (congestive hepatopathy) |
| Pulsatile liver | Tricuspid regurgitation |
| Hepatojugular reflux | Advanced RV failure / obstruction to RV filling |
| Splenomegaly | Infective endocarditis, portal hypertension from chronic HF |
| Pulsatile abdominal mass | Abdominal aortic aneurysm |
| Ascites | Advanced right heart failure, constrictive pericarditis |
| Peripheral edema (pitting) | Right heart failure |
| Ankle-brachial index <0.9 | Peripheral arterial disease |
| Femoral/popliteal aneurysm | Associated with AAA |
| Absent foot pulses | PAD, aortic coarctation (in legs) |
DISEASE-BY-DISEASE SUMMARY: SIGNS IN ORDER
Aortic Stenosis
- General: symptoms on exertion (angina, syncope, dyspnea = classic triad)
- Pulse: parvus et tardus; narrow pulse pressure
- JVP: may show prominent a wave (if pulmonary hypertension develops)
- Apex: sustained (heaving), not displaced (unless LV dilation in late disease)
- Palpation: systolic thrill at 2nd right ICS
- S1: normal; S2: single or paradoxically split (P2 soft/absent A2)
- S4 gallop present
- Murmur: midsystolic ejection crescendo-decrescendo at right 2nd ICS, radiating to carotids
Aortic Regurgitation (Chronic)
- Pulse: water-hammer (Corrigan's); wide pulse pressure; bisferiens if severe
- BP: high systolic, very low diastolic
- Apex: displaced laterally and inferiorly (volume overloaded LV)
- S1: normal; early diastolic decrescendo murmur at left sternal border
- Austin Flint murmur at apex (in severe AR)
- S3 in decompensated AR
- Peripheral signs: pistol-shot femoral pulse (Traube's), Duroziez sign, Quincke pulses, de Musset's sign (head nodding)
Mitral Stenosis
- General: dyspnea, hemoptysis, AF, systemic emboli
- Pulse: irregular if AF
- JVP: elevated if pulmonary hypertension present
- Apex: not displaced; "tapping" quality (palpable S1)
- S1: loud (pliable leaflets); S2: loud P2 if pulmonary hypertension
- Opening snap (shortly after S2)
- Mid-diastolic rumble at apex (bell of stethoscope, left lateral decubitus)
- Presystolic accentuation (in sinus rhythm)
Mitral Regurgitation (Chronic)
- Pulse: brisk, hyperdynamic
- Apex: displaced laterally (volume overload); palpable S3
- S1: soft; S2: wide splitting (early A2 due to rapid LV emptying); S3 present
- Holosystolic blowing murmur at apex, radiating to axilla
- If posterior leaflet: murmur radiates anteriorly to base (mimics AS)
Hypertrophic Obstructive Cardiomyopathy (HOCM)
- General: dyspnea, syncope, chest pain, palpitations in young patient; family history of sudden death
- Pulse: bisferiens; spike-and-dome character
- Apex: triple cadence (S4 + bisferiens); sustained but not displaced
- S4 prominent
- Midsystolic murmur at left lower sternal border
- Dynamic character is key: increases with Valsalva and standing; decreases with squatting and handgrip
- Coexistent MR murmur often present
Constrictive Pericarditis
- General: fatigue, peripheral edema, ascites - often misdiagnosed as liver disease
- JVP: elevated with prominent/rapid y descent; Kussmaul sign (JVP rises with inspiration)
- Pulse: may have pulsus paradoxus (mild)
- Precordium: quiet precordium (no heave)
- S3 equivalent = pericardial knock (high-pitched early diastolic sound; earlier than usual S3, occurs at nadir of rapid Y descent)
- Hepatomegaly, ascites, peripheral edema
Cardiac Tamponade
- General: Beck's triad - Hypotension + Elevated JVP + Muffled heart sounds
- JVP: elevated; blunted/absent Y descent (impaired diastolic filling)
- Pulse: pulsus paradoxus >10 mmHg (may be palpable >15 mmHg)
- Precordium: quiet, no heave, heart sounds muffled
- No Kussmaul sign
Differentiating Tamponade vs Constrictive Pericarditis
| Feature | Tamponade | Constrictive Pericarditis |
|---|---|---|
| Pulsus paradoxus | Present (prominent) | Mild or absent |
| JVP Y descent | Absent/blunted | Prominent, rapid |
| Kussmaul sign | Absent | Present |
| Heart sounds | Muffled | Normal intensity + pericardial knock |
| Pericardial knock | Absent | Present |
| Echo | Pericardial effusion + RV collapse | Thickened/calcified pericardium |
Pulmonary Hypertension
- Pulse: normal or reduced volume
- JVP: elevated; prominent a wave; if TR develops - prominent v wave
- RV heave at left parasternal area
- Palpable P2 at left 2nd ICS
- S2: loud P2, narrow or single splitting
- Right-sided S4; then right-sided S3 if RV fails
- Ejection click in pulmonic area
- TR murmur (holosystolic, left lower sternal border, increases with inspiration) develops late
- PR murmur (Graham Steell) - high-pitched early diastolic decrescendo at left 2nd-3rd ICS
Infective Endocarditis
- General: fever, weight loss, fatigue, embolic phenomena
- Eyes: Roth spots (fundus), petechiae
- Hands: Osler nodes (painful tender nodules - fingertips), Janeway lesions (non-tender hemorrhagic macules - palms/soles), splinter hemorrhages (nails)
- New or changing murmur (most commonly MR or AR)
- Splenomegaly
- Signs of heart failure if severe valvular destruction
NYHA FUNCTIONAL CLASSIFICATION (Summary)
| Class | Limitation |
|---|---|
| I | No limitation; ordinary activity does not cause symptoms |
| II | Slight limitation; ordinary activity causes fatigue/palpitation/dyspnea/angina |
| III | Marked limitation; less than ordinary activity causes symptoms |
| IV | Unable to do any activity without discomfort; symptoms at rest |
Harrison's Principles of Internal Medicine 22E (2025), Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.