femoral and acetabular anteversion in total hip, arthroplasty
Reading File
Finding Sources
Finding Sources
Searching PubMed
femoral acetabular anteversion total hip arthroplasty combined
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
I have all the material needed for a thorough answer. Here is the complete synthesis:
Femoral and Acetabular Anteversion in Total Hip Arthroplasty
Component orientation - particularly anteversion - is one of the most consequential technical factors in THA, directly affecting dislocation risk, impingement, polyethylene wear, and overall function.
1. Definitions
Anteversion refers to the anterior rotation of a component's opening or axis relative to a reference plane (typically the coronal/frontal plane for the cup, and the tibial axis for the stem).
- Acetabular anteversion: the angle between the cup's opening plane and the coronal plane when the pelvis is in a neutral position. It determines how much the cup faces anteriorly.
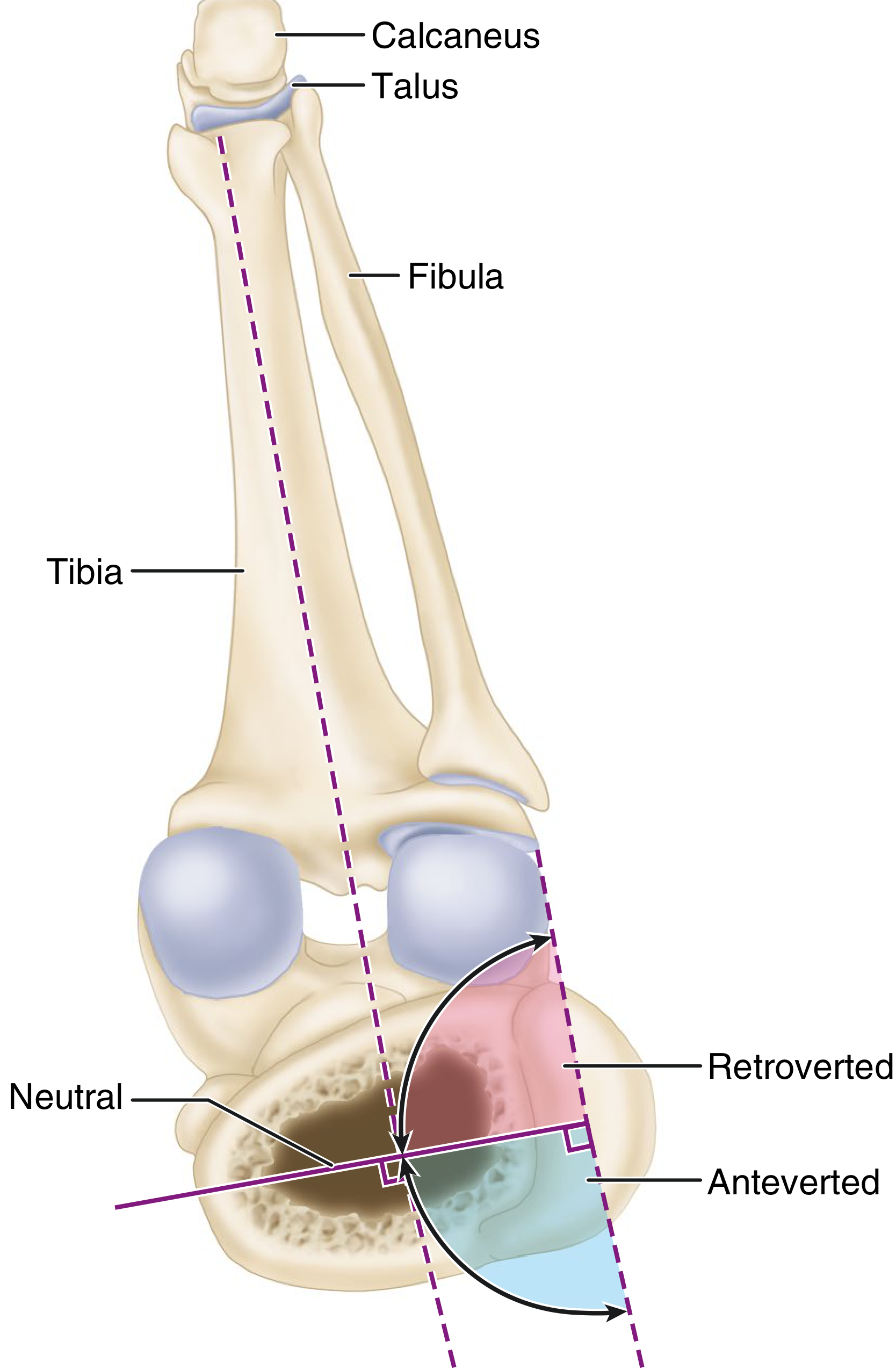
- Femoral anteversion: the angle between the axis of the prosthetic femoral neck and the shaft of the tibia with the knee at 90° of flexion. Neutral = 90° (neck perpendicular to tibia); obtuse angle = anteversion; acute angle = retroversion.
2. Target Angles
Acetabular Component
| Parameter | Target (Lewinnek "safe zone") | Updated range |
|---|---|---|
| Anteversion | 15 ± 10° (5°-25°) | 18°-38° |
| Inclination (abduction) | 40 ± 10° (30°-50°) | 27°-47° |
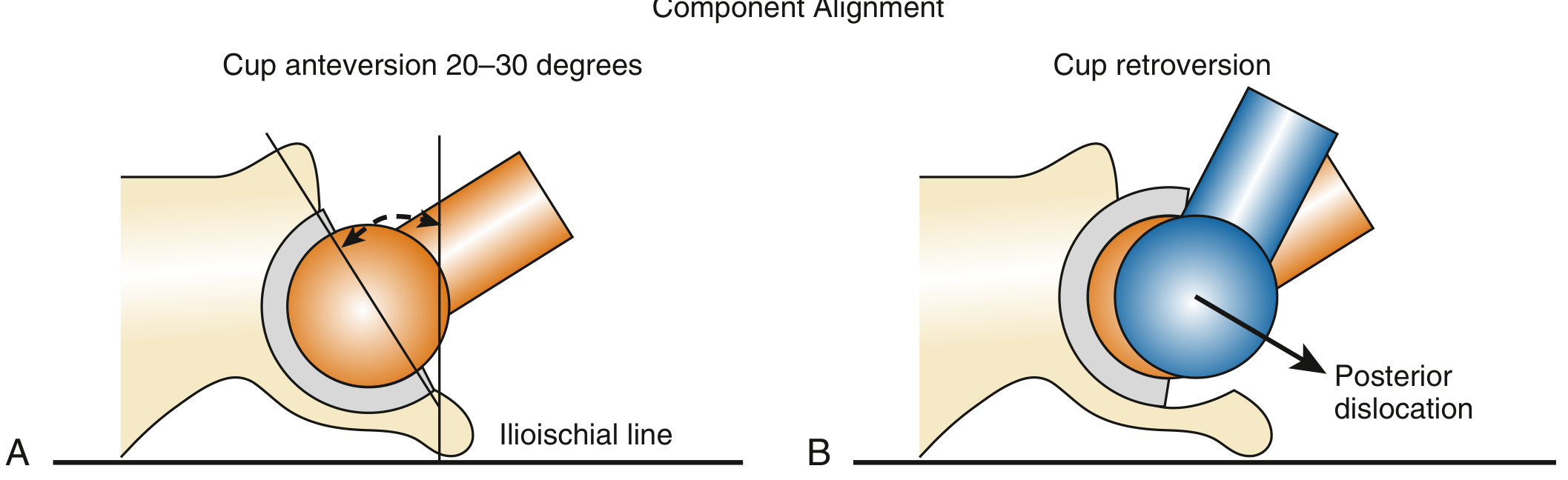
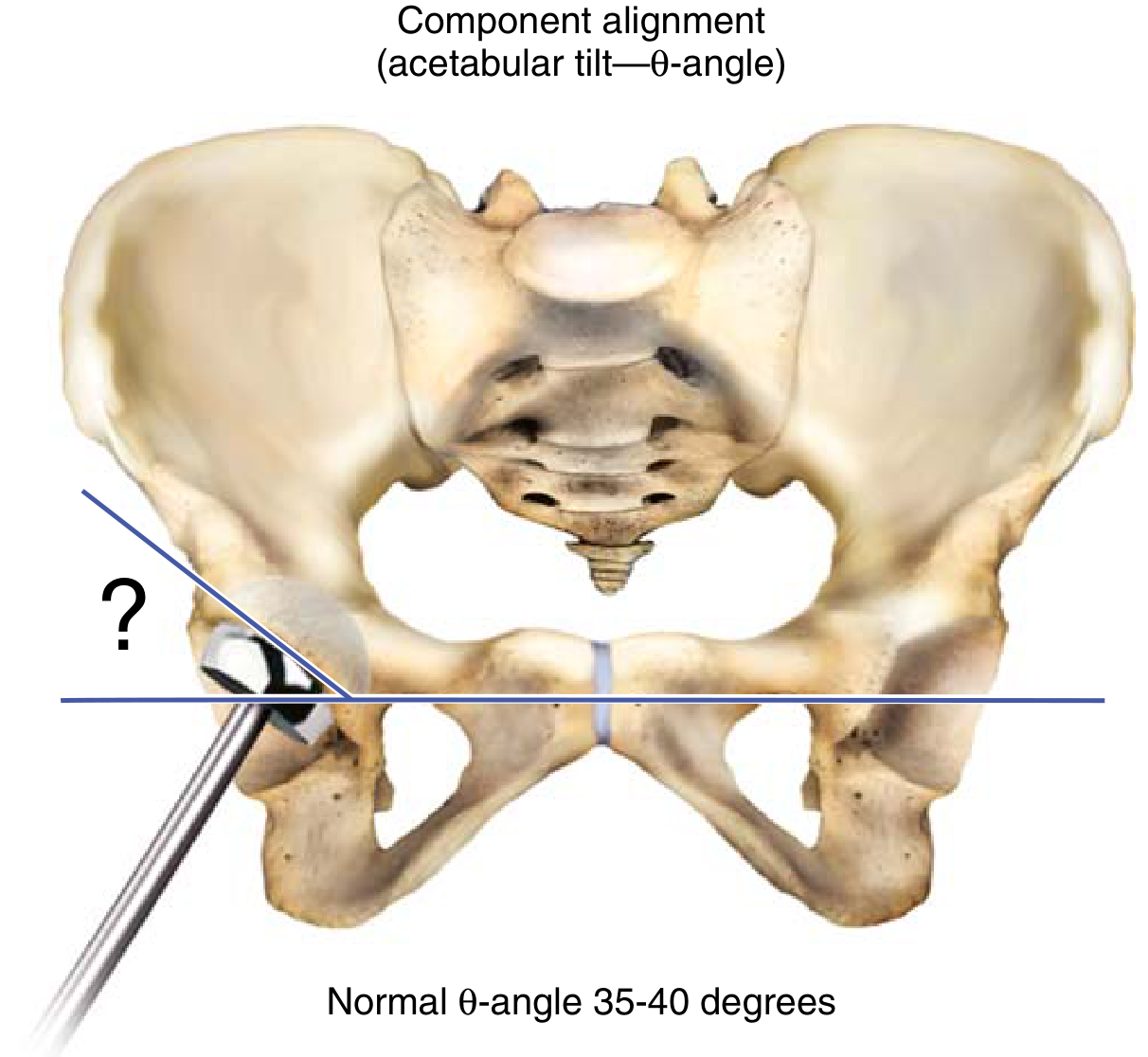
Miller's Review specifies cup anteversion of 20-30° referenced to the ilioischial line, and a theta (θ) angle (coronal tilt) of 35-40° (see diagram below).
Femoral Component
The femoral stem should be implanted with the neck in 5-15° of anteversion. Severe excess anteversion (e.g., 70°) causes recurrent anterior dislocation (Fig. 4.111 in Campbell's).
Intraoperative assessment: Compare the axis of the prosthetic femoral neck with the tibial shaft at 90° knee flexion. Neutral = 90°; >90° = anteversion; <90° = retroversion.
3. Combined Anteversion
The combined anteversion concept recognizes that the cup and stem work together - their individual anteversions must be considered as a sum to achieve hip stability.
Target: 25-50° combined anteversion (traditional safe zone) - Campbell's and Miller's are in agreement here.
The "combined anteversion technique" (Dorr/Amuwa, 2008) adjusts acetabular anteversion intraoperatively based on the achieved femoral component version:
Combined anteversion = Acetabular anteversion + Femoral anteversion
Practical rule: If the stem ends up with more anteversion than planned (e.g., in DDH), the cup should be placed with correspondingly less anteversion to keep the combined value in range - and vice versa.
4. Consequences of Malposition
| Malposition | Mechanism | Result |
|---|---|---|
| Cup retroversion | Femur impinges on posterior rim in flexion/IR | Posterior dislocation |
| Cup excess anteversion | Femur levers out in extension/ER | Anterior dislocation |
| High θ angle (vertical cup) | Superior rim impingement in adduction | Posterior-superior dislocation |
| Stem retroversion | Same as cup retroversion | Posterior dislocation |
| Stem excess anteversion | Same as cup excess anteversion | Anterior dislocation |
| Horizontal cup | Early impingement in flexion (± low anteversion) | Posterior dislocation |
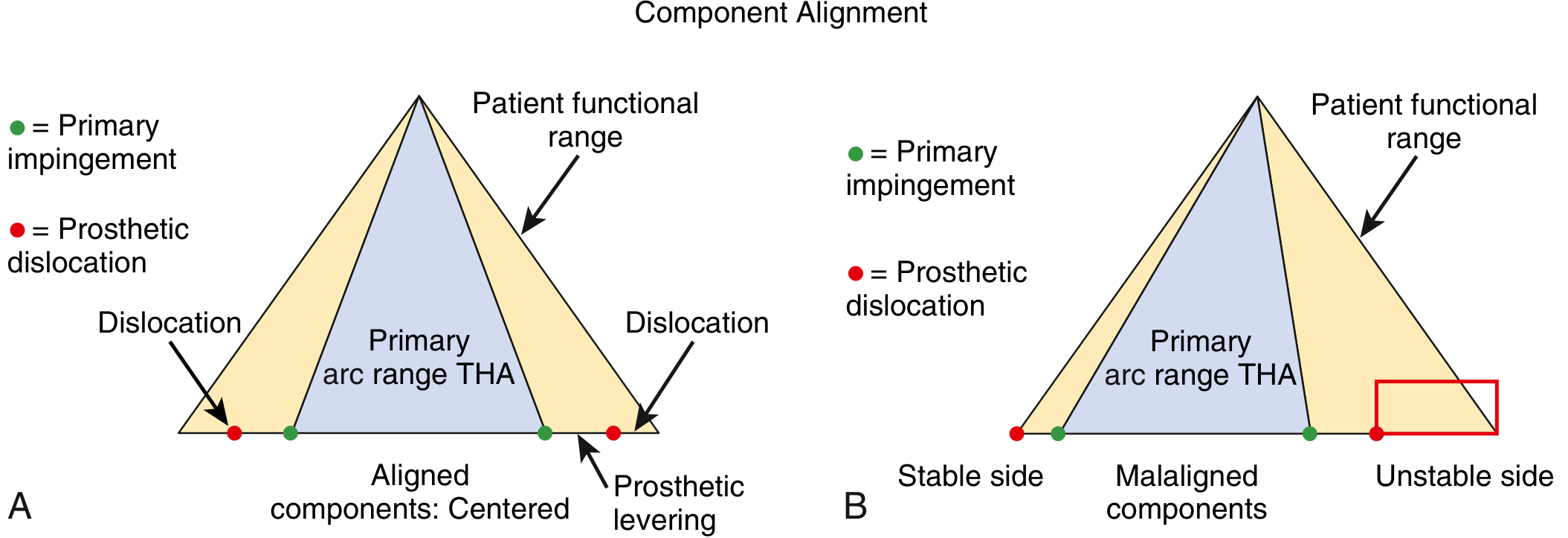
Component malposition does not shrink the total arc of motion of the prosthesis - it offsets it, creating a stable side and an unstable side within the patient's functional range.
5. The Hip-Spine Relationship and Adjusting Safe Zone Targets
The Lewinnek safe zone is not universal. Spinal fusion history confers a 2x risk of early dislocation and 3x risk for revision after THA (meta-analysis cited in Campbell's), because spinal deformity and stiffness alter functional acetabular orientation with posture changes.
Key concepts:
- With each 1° of posterior pelvic tilt (standing to sitting), acetabular anteversion functionally increases by 0.7-0.8°, totalling ~15.6° of change normally
- Normal sacral slope (SS) change from standing to sitting: 11-30°
- Spinopelvic stiffness = SS change ≤10° - these patients cannot "roll back" their pelvis when sitting, causing anterior impingement
Adjusted targets by spinopelvic mobility (Campbell's Table 4.4):
| Spinopelvic Type | Inclination | Cup Anteversion | Combined Anteversion |
|---|---|---|---|
| Normal | 35°-45° | 15°-25° | 25°-45° |
| Stiff | 45°-50°+ | 20°-25° | 35°-45° |
| Kyphotic | 35°-40° | 15°-20° | 25°-35° |
| Hypermobile | 35°-40° | 12°-20° | 25°-35° |
Vigdorchik classification for hip-spine patients:
- 1A: Normal alignment + normal motion (standard targets)
- 1B: Normal alignment + stiff spine (increase anteversion)
- 2A: Flatback deformity (PI - LL >10°) + normal motion
- 2B: Flatback + stiffness (highest risk - narrowest safe zone, consider dual mobility)
6. Clinical Notes
- Developmental dysplasia of the hip (DDH): femoral neck is often excessively anteverted natively; the implanted stem may need less anteversion, or combined anteversion must be carefully balanced
- Juvenile RA: similar issue with excess native femoral anteversion
- Post-fracture acetabula: posterior wall deficiency limits achievable cup anteversion; retained anterior osteophytes cause impingement in flexion/IR
- Radiographic assessment of cup anteversion: plain films are imprecise; CT is the gold standard; a cross-table lateral view is a reasonable alternative
- Navigation and robotic systems: achieving target anteversion within ±10° is difficult without guidance; these technologies improve precision and are increasingly used in hip-spine patients
Sources: Campbell's Operative Orthopaedics 15th Ed 2026, pp. 307-309, Table 4.4, and Hip-Spine Relationship section (pp. 253-254); Miller's Review of Orthopaedics 9th Edition, pp. 450-451
crossover sign in femoral retroversion
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
Loading Image
I have all the material needed. Here is the complete, precise answer - with an important clarification up front:
The Crossover Sign and Its Relationship to Retroversion
Important Clarification
The crossover sign is a radiographic sign of acetabular retroversion - not femoral retroversion. It is frequently asked about in the context of femoroacetabular impingement (FAI), where acetabular retroversion produces pincer-type impingement. Femoral retroversion is a separate entity that can coexist with or functionally mimic the same impingement pattern, but it does not produce the crossover sign itself.
1. What Is the Crossover Sign?
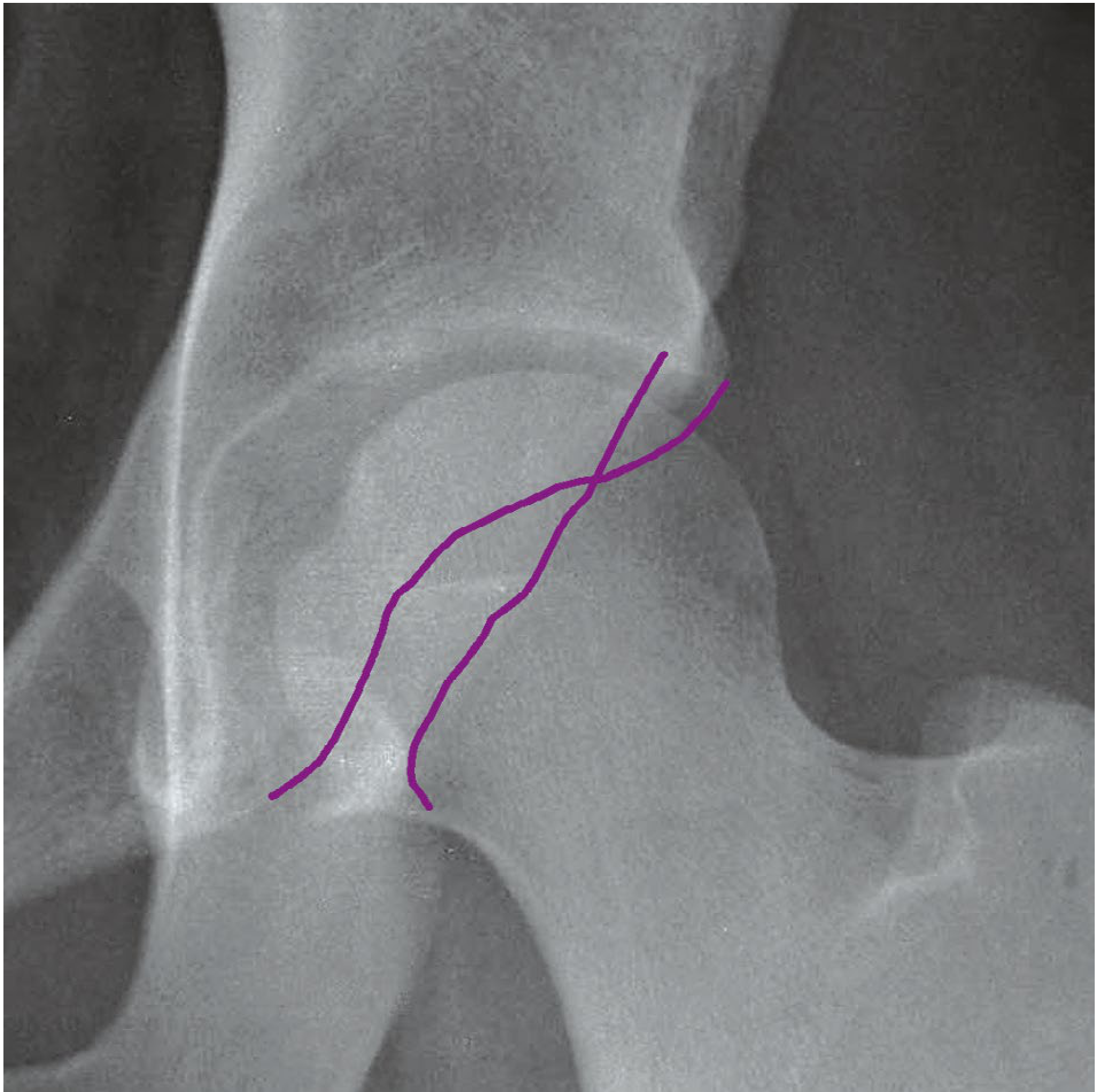
On a well-positioned AP pelvis radiograph, trace the outlines of the anterior and posterior acetabular walls:
- Normal: The anterior wall (runs medially) and posterior wall (runs laterally) converge at the superior lateral margin of the acetabulum - they meet at the top without crossing.
- Crossover sign (positive): The anterior wall outline crosses lateral to the posterior wall outline below the superior lateral margin of the acetabulum, forming an "X" shape.
This crossing occurs because in a retroverted acetabulum the anterior rim is tilted more anteriorly and laterally than normal, producing anterior overcoverage.
2. What Does It Mean?
The crossover sign indicates one of two things, and distinguishing them is critical because treatment differs:
| Finding | Interpretation |
|---|---|
| Crossover sign alone | Isolated anterior overcoverage (focal rim retroversion) |
| Crossover sign + posterior wall sign + prominent ischial spine | Retroversion of the entire acetabulum with deficient posterior coverage |
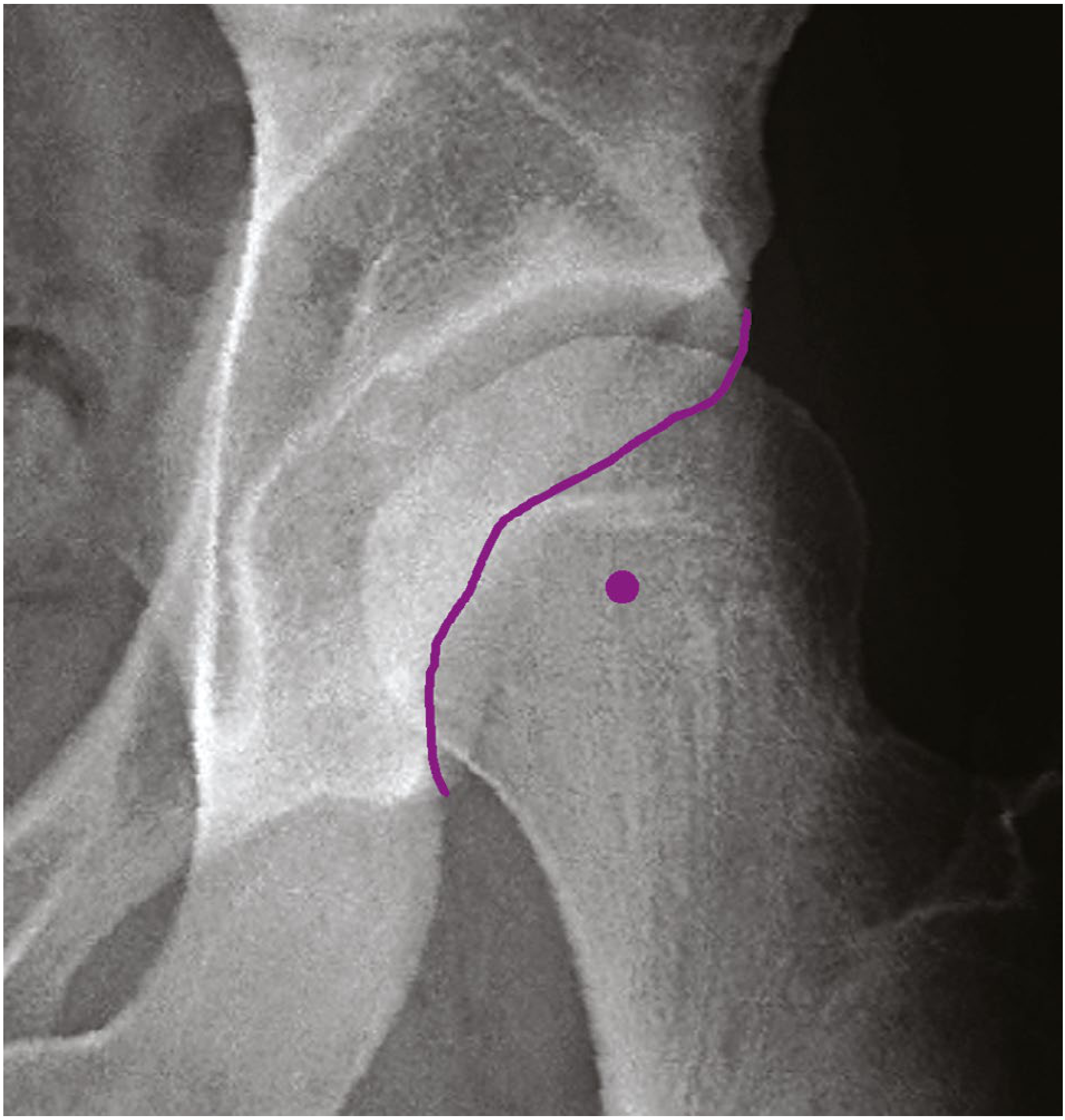
Posterior Wall Sign
The posterior wall sign is positive when the center of the femoral head lies lateral to the lateral margin of the posterior wall on an AP pelvis view. This indicates the posterior wall is deficient - the acetabulum has been retroverted globally, not just anteriorly.
Ischial Spine Sign
Ipsilateral prominence of the ischial spine on an otherwise well-positioned AP pelvis radiograph is an additional sign of global acetabular retroversion.
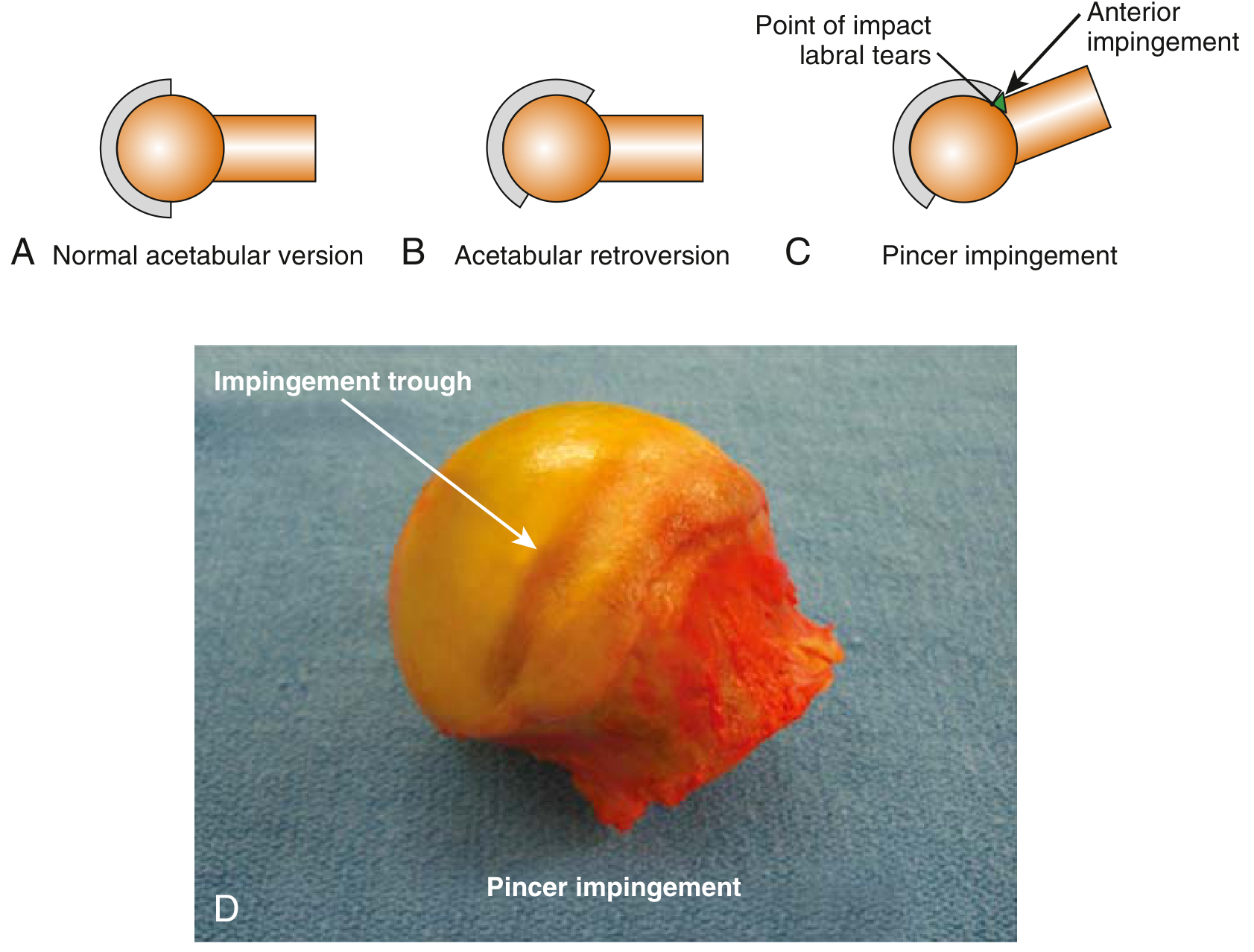
3. Pathomechanics: Pincer FAI from Acetabular Retroversion
A retroverted acetabulum causes the anterior rim to protrude anteriorly. During hip flexion, adduction, and internal rotation, the femoral neck contacts the anterior acetabular rim earlier than normal - this is pincer-type impingement.
The result:
- Intrasubstance labral tears, typically anterosuperior
- A contrecoup cartilage lesion on the posteroinferior acetabulum (the femoral head is levered into the posterior wall while the neck impinges anteriorly)
4. False Positives - A Key Caveat
Campbell's specifically notes: a crossover sign may also be caused by variations in the morphology of the anterior inferior iliac spine (AIIS) in the presence of normal acetabular version. This is a recognized pitfall.
Miller's goes further: later studies have demonstrated a high rate of false-positive radiographic findings for FAI. More than 90% of asymptomatic adolescents have at least one radiographic parameter suggesting FAI, and 50% have two. Therefore, imaging findings must always be correlated with clinical history and examination.
5. Femoral Retroversion vs. Acetabular Retroversion
Though the crossover sign itself reflects acetabular version, femoral retroversion creates a functionally similar impingement scenario:
| Feature | Acetabular Retroversion | Femoral Retroversion |
|---|---|---|
| Radiographic sign | Crossover sign (AP pelvis) | Increased external rotation, reduced IR (clinical); CT/MRI measurement of femoral neck-shaft angle |
| Impingement type | Pincer | Functional cam or extra-articular |
| Mechanism | Anterior rim protrudes, catches neck | Retroverted femoral neck presents the posterior head-neck junction anteriorly during flexion |
| Symptom | Pain with flexion + IR (anterior impingement test positive) | Pain with flexion + IR; more external rotation than internal rotation at rest |
| Treatment | Rim trimming (isolated retroversion) or PAO (global retroversion) | Femoral derotation osteotomy |
In clinical practice, both can coexist and both can cause a positive anterior impingement test (FADIR: flexion, adduction, internal rotation). CT is the definitive study to measure femoral torsion, while plain AP pelvis identifies the crossover sign for acetabular retroversion.
6. Treatment Implications Based on Crossover Sign Pattern
| Pattern | Treatment |
|---|---|
| Crossover sign only (isolated anterior overcoverage) | Arthroscopic labral reflection + rim trimming + labral reattachment; or limited open anterior approach |
| Crossover + posterior wall sign + ischial spine sign (global retroversion) | Periacetabular osteotomy (PAO) to antevert the entire acetabulum |
| Crossover + borderline dysplasia (LCE 20-25°) + cam deformity | Complex decision - may require PAO + osteochondroplasty; arthroscopy alone risks instability if anterior capsulotomy not repaired |
Sources: Campbell's Operative Orthopaedics 15th Ed 2026, pp. 429-437 (Acetabular Version on AP Radiograph; Pincer FAI treatment); Miller's Review of Orthopaedics 9th Edition, pp. 424-425, 450-451 (FAI imaging, component alignment)
coaxial stich technique in femoral trail in total hip arthroplasty
Finding Sources
Finding Sources
Searching the Web
coaxial stitch technique femoral trial total hip arthroplasty anteversion
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.