Properties of cardiac muscle physiology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from the textbooks. Let me compile the full answer.
Properties of Cardiac Muscle Physiology
Cardiac muscle has several unique physiological properties that set it apart from skeletal and smooth muscle. Here is a systematic overview.
1. Structural Basis
The contractile machinery of cardiac muscle is fundamentally similar to skeletal muscle - sarcomeres running from Z line to Z line, composed of thick filaments (myosin, with actin-binding globular heads and ATPase activity) and thin filaments (actin, tropomyosin, and troponin). Contraction follows the sliding filament model: cross-bridge formation and cycling between myosin and actin causes filaments to slide past each other, producing tension.
Key structural features unique to cardiac muscle:
-
T-tubules invaginate at the Z lines (not the A-I junctions as in skeletal muscle) and form dyad junctions with the SR (not triads)
-
T-tubules are 5x wider than in skeletal muscle, providing a large reservoir of extracellular calcium
-
Intercalated discs connect adjacent cardiomyocytes and contain gap junctions (connexins), allowing the heart to behave as a functional syncytium - an electrical impulse in one cell spreads rapidly to all cells
-
Costanzo Physiology 7th Edition, p. 150
-
Guyton and Hall Textbook of Medical Physiology, p. 124
2. The Cardiac Action Potential
Cardiac cells are classified into two groups based on their action potential characteristics:
Non-pacemaker (fast-response) cells - Ventricles, Atria, Purkinje fibers

The ventricular action potential has 5 phases:
| Phase | Name | Ion Movement |
|---|---|---|
| Phase 0 | Rapid upstroke | Fast Na+ channels open → rapid depolarization to ~+20 mV |
| Phase 1 | Early repolarization | Na+ channels close; transient K+ efflux |
| Phase 2 | Plateau | L-type Ca2+ channels (dihydropyridine receptors) open → inward Ca2+ current balances K+ efflux; this is the defining feature of cardiac AP |
| Phase 3 | Rapid repolarization | Ca2+ channels close; slow K+ channels open → K+ efflux returns membrane to resting potential |
| Phase 4 | Resting membrane potential | Stable at -85 to -90 mV; maintained by K+ conductance |
- Costanzo Physiology 7th Edition, pp. 140-142
Pacemaker (slow-response) cells - SA node, AV node
The SA node action potential lacks a true resting potential. Instead, Phase 4 shows spontaneous, slow depolarization (the pacemaker potential or "funny current", If) driven by a gradual decrease in K+ conductance and inward Na+/Ca2+ currents. When threshold is reached, Ca2+ channels (not Na+ channels) generate the upstroke. This is the basis of automaticity.
3. Key Physiological Properties
A. Automaticity (Rhythmicity)
The SA node spontaneously generates action potentials at ~60-100/min, making it the primary pacemaker. The AV node (~40-60/min) and Purkinje fibers (~20-40/min) also have automaticity but are normally suppressed by the faster SA node - a phenomenon called overdrive suppression. The SA node "resets" slower pacemakers with each impulse via the principle of the dominant pacemaker.
B. Conductivity
Electrical signals spread from cell to cell through gap junctions in intercalated discs, allowing coordinated contraction. Conduction velocity varies by tissue:
- Atrial/ventricular muscle: 0.3-0.5 m/sec
- Purkinje system: up to 4 m/sec (rapid delivery to all ventricular regions)
- AV node: 0.02-0.05 m/sec (intentional delay, allowing ventricular filling)
C. Excitability and Refractoriness
The absolute refractory period (ARP) of ventricular muscle lasts 0.25-0.30 seconds - nearly the entire duration of contraction. This prevents tetanic (sustained) contractions, which would be fatal for a pump. There is also a relative refractory period (~0.05 sec) during which stronger-than-normal stimuli can trigger a premature contraction, but wave summation (as in skeletal muscle) does not occur.
"The refractory period of atrial muscle is much shorter than that for the ventricles (about 0.15 second for the atria compared with 0.25 to 0.30 second for the ventricles)."
- Guyton and Hall Textbook of Medical Physiology, p. 125
D. Contractility (Inotropism)
Contractility is the intrinsic ability of myocardial cells to develop force at a given cell length, independent of preload or afterload. Agents affecting contractility:
- Positive inotropes (increase contractility): catecholamines, digoxin, Ca2+, sympathetic stimulation
- Negative inotropes (decrease contractility): beta-blockers, calcium channel blockers, acidosis, hypoxia
Contractility correlates directly with intracellular Ca2+ concentration, which depends on sarcoplasmic reticulum stores and the size of the Ca2+ current during the plateau phase. - Costanzo Physiology 7th Edition, p. 151
4. Excitation-Contraction (E-C) Coupling
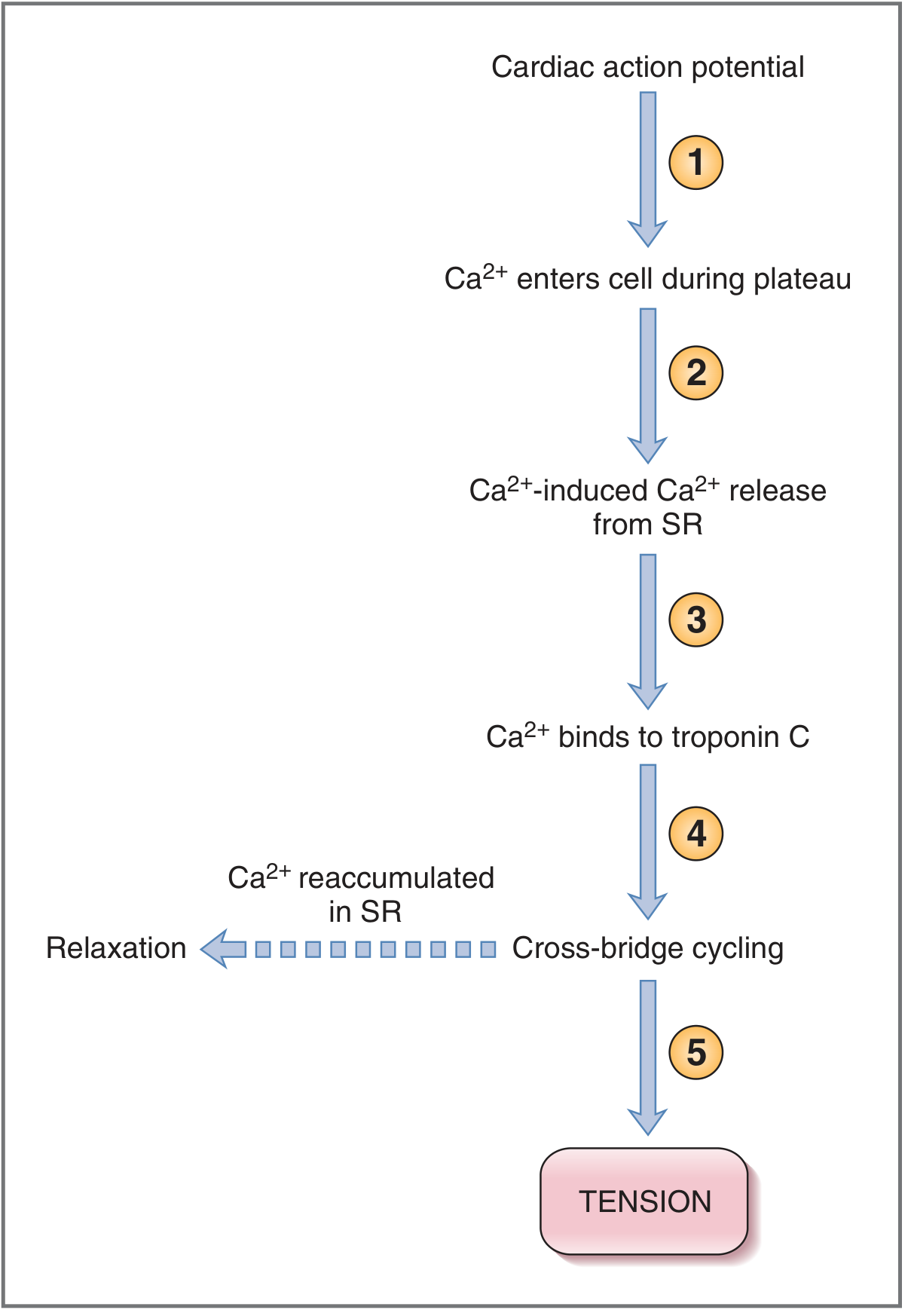
The unique cardiac EC coupling mechanism is Ca²⁺-induced Ca²⁺ release (CICR):
- Action potential spreads along sarcolemma and into T-tubules
- T-tubule depolarization opens L-type Ca2+ channels → small amount of Ca2+ enters ("trigger Ca2+")
- Trigger Ca2+ activates ryanodine receptor (RyR2) channels on the SR → large-scale Ca2+ release from SR stores
- Cytoplasmic Ca2+ rises → Ca2+ binds troponin C → conformational change removes tropomyosin inhibition → actin-myosin cross-bridge cycling → TENSION
- The magnitude of tension is proportional to intracellular Ca2+ concentration (unlike the all-or-nothing response of skeletal muscle)
Relaxation occurs when:
- SERCA2 (Ca2+-ATPase) pumps Ca2+ back into SR
- Na+-Ca2+ exchanger and sarcolemmal Ca2+-ATPase extrude Ca2+ to extracellular space
- Ca2+ dissociates from troponin C → cross-bridges stop → relaxation
"Without the calcium from the T tubules, the strength of cardiac muscle contraction would be reduced considerably because the sarcoplasmic reticulum of cardiac muscle is less well developed than that of skeletal muscle and does not store enough calcium to provide full contraction."
- Guyton and Hall Textbook of Medical Physiology, p. 125
5. Frank-Starling Mechanism (Length-Tension Relationship)
The Frank-Starling law states: within physiological limits, the heart pumps all the blood that returns to it. As end-diastolic volume increases (increased preload), cardiac muscle fibers stretch, actin-myosin filaments achieve more optimal overlap for force generation, and the ventricle contracts with greater force - pumping the extra volume.
- Increased atrial filling → fiber stretch → stronger contraction → greater stroke volume
- Right atrial stretch also increases heart rate by 10-20% (Bainbridge reflex)
- Guyton and Hall Textbook of Medical Physiology, p. 109
6. Differences from Skeletal Muscle - Summary
| Property | Cardiac Muscle | Skeletal Muscle |
|---|---|---|
| Action potential duration | ~200-400 ms | ~1-2 ms |
| Plateau phase | Yes (Phase 2) | No |
| Refractory period | Long (=contraction duration) | Short |
| Tetanus | Cannot occur | Can occur |
| EC coupling | CICR (extracellular Ca2+ essential) | Direct mechanical coupling (Ca2+ from SR only) |
| Pacemaker activity | Yes (intrinsic) | No |
| T-tubule location | Z lines (dyads) | A-I junction (triads) |
| Response to Ca2+ | Graded (proportional) | All-or-nothing |
| Frank-Starling | Prominent | Present but less pronounced |
Key sources used:
- Costanzo Physiology, 7th Edition - Cardiac Muscle Contraction section
- Guyton and Hall Textbook of Medical Physiology - Action Potentials in Cardiac Muscle; Frank-Starling Mechanism
- Medical Physiology (Boron & Boulpaep) - Ca2+-induced Ca2+ release mechanism
This is a shared conversation. Sign in to Orris to start your own chat.