Acute mi
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Searching PubMed
"myocardial infarction" AND pathophysiology
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have all the content needed for a comprehensive, well-illustrated answer. Let me compile it.
Acute Myocardial Infarction - Pathophysiology & Types
Definition
At the cellular level, an acute MI is myocardial cell death with necrosis of the myocardium. The Fourth Universal Definition of Myocardial Infarction (ACC/ESC) distinguishes two related terms:
- Myocardial injury: elevated cardiac troponin with at least one value above the 99th percentile upper reference limit (URL), with a rise or fall indicating acuity.
- Myocardial infarction: acute myocardial injury (elevated troponin > 99th percentile URL) PLUS at least one of:
- Symptoms of myocardial ischemia
- New ischemic ECG changes (ST/T changes or new pathologic Q waves)
- Imaging evidence of new loss of viable myocardium or regional wall motion abnormality
- Angiographic or autopsy evidence of coronary thrombus
(ROSEN's Emergency Medicine, p. 996)
Pathophysiology
1. Oxygen Supply-Demand Imbalance
The core mechanism is inadequate coronary perfusion relative to myocardial oxygen demand. Myocardial oxygen consumption is determined by:
- Heart rate
- Afterload
- Contractility
- Wall tension
Coronary stenosis typically does not cause resting ischemia until obstruction exceeds 95% of the vessel lumen. Below this threshold, ischemia may still occur with physiologic stress and increased demand. (ROSEN's, p. 996)
2. Atherosclerosis and Plaque Biology
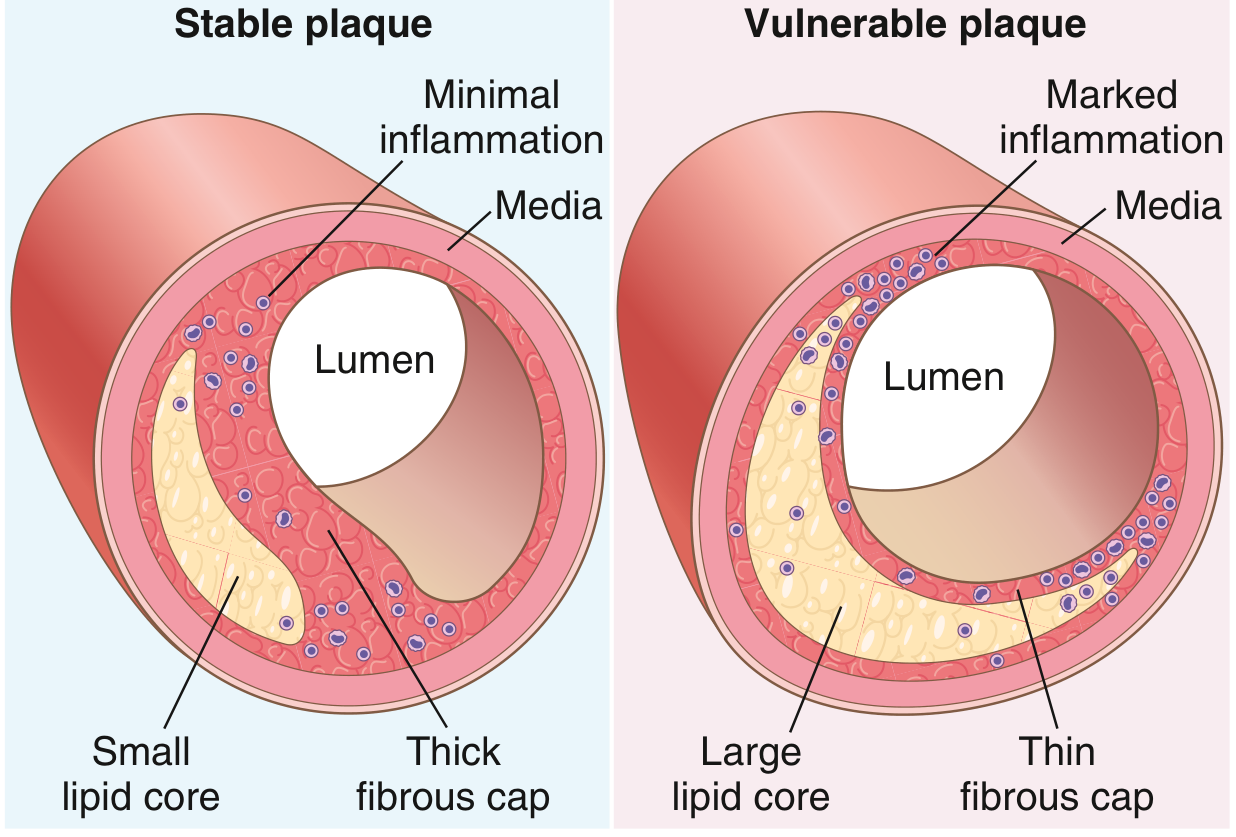
Coronary artery disease (CAD) develops through thickening and obstruction of the arterial lumen by atherosclerotic plaques. Two plaque types are relevant:
| Plaque Type | Features | Risk |
|---|---|---|
| Fibrous (stable) | Thick fibrous cap, small lipid core, minimal inflammation | Causes stable angina; unlikely to rupture |
| Fibro-lipid (vulnerable) | Thin fibrous cap (<55 µm), large lipid-rich necrotic core, abundant macrophages, marked inflammation | High risk of rupture |
The fibrous cap's mechanical stability is proportional to its collagen content. Inflammation destabilizes plaques by increasing metalloprotease-mediated collagen degradation and reducing smooth muscle cell collagen synthesis. Adrenergic stimulation (e.g., physical exertion, intense emotions) can also increase shear forces and trigger rupture. (Robbins & Kumar Basic Pathology, p. 322)
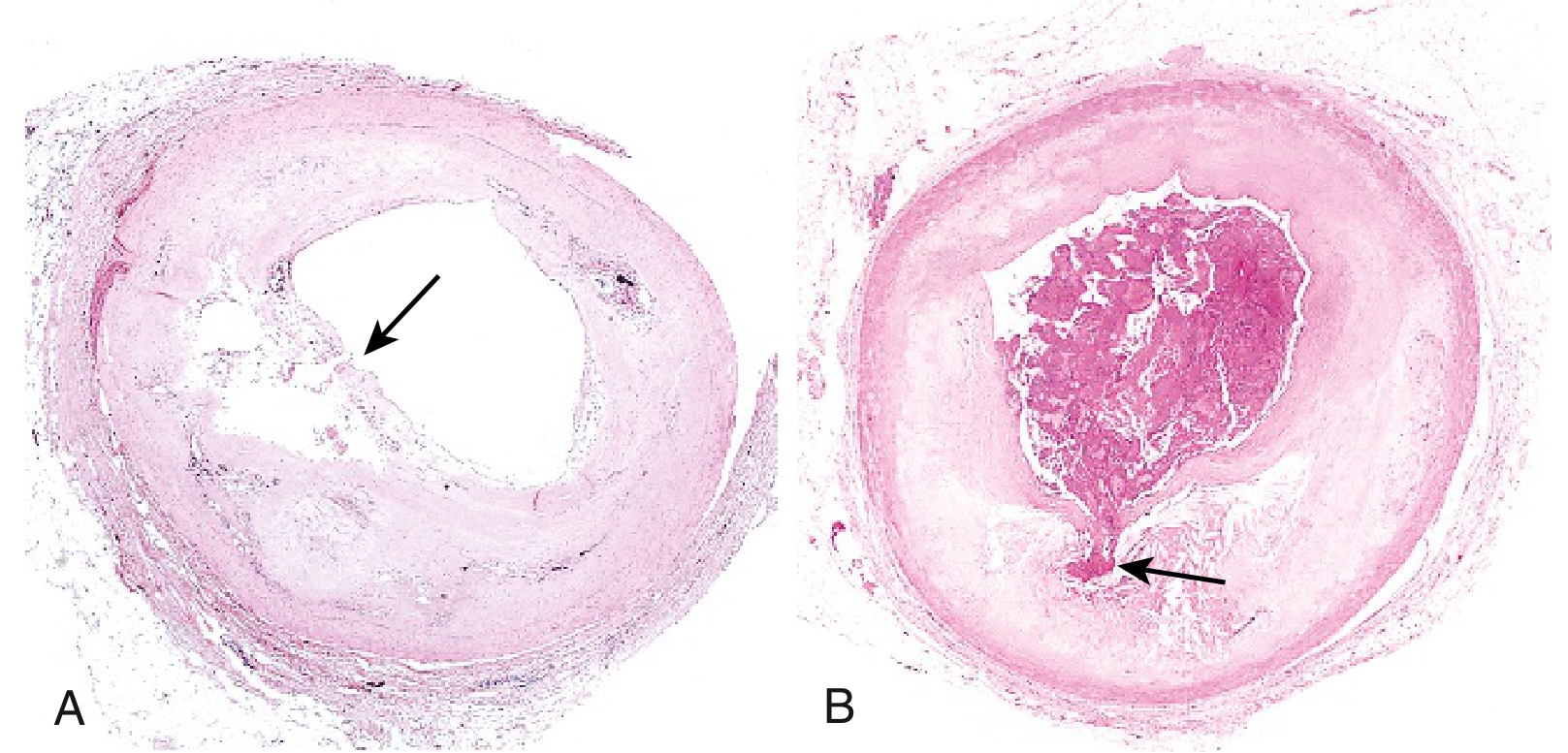
3. Plaque Rupture / Erosion - The Triggering Event
Rupture of the fibrous cap (most commonly at its shoulder regions) exposes the thrombogenic necrotic core to luminal blood. This initiates a cascade:
- Plaque disruption - rupture, erosion, or fissuring of the fibrous cap
- Platelet activation - platelets adhere to exposed subendothelial collagen and plaque contents
- White thrombus formation - platelet-rich thrombus forms at the rupture site
- Red thrombus propagation - fibrin-rich thrombus extends proximally and distally
- Luminal occlusion - partial (NSTEMI/UA) or complete (STEMI)
- Myocardial necrosis - irreversible cell death downstream
Note: plaques responsible for AMI are often not significantly stenotic beforehand - a catastrophic event can arise from a previously asymptomatic, non-flow-limiting plaque. (Robbins & Kumar, p. 322; Fuster and Hurst's The Heart, 15th ed.)
4. STEMI vs. NSTEMI
| Feature | STEMI | NSTEMI/UA |
|---|---|---|
| Coronary occlusion | Complete, total | Partial / subtotal |
| Extent of infarction | Transmural (full-wall thickness) | Subendocardial |
| ECG | ST-segment elevation | ST depression, T-wave changes, or normal |
| Troponin | Elevated (rise and fall) | Elevated (NSTEMI) / normal (UA) |
STEMI results from acute, total occlusion of an epicardial coronary artery - most often due to plaque rupture/erosion with complete thrombotic occlusion. The older terms "transmural" vs. "non-transmural" or "Q-wave" vs. "non-Q-wave" MI are no longer preferred because they imperfectly reflect the coronary event and its pathology. (Washington Manual of Medical Therapeutics; ROSEN's, p. 997)
Types of AMI - The Fourth Universal Classification
The five types reflect the clinical mechanism behind the infarction:
Type 1 - Spontaneous MI (True ACS)
Caused by a primary coronary event: atherosclerotic plaque rupture, erosion, fissuring, or dissection, with accompanying thrombus formation and/or vasospasm. This is the classic ACS mechanism - platelet and coagulation inhibition are the cornerstone of management.
Type 2 - Secondary MI (Supply-Demand Mismatch)
MI secondary to ischemia from increased oxygen demand or decreased supply, unrelated to primary plaque rupture. Examples:
- Coronary artery spasm
- Coronary embolism
- Severe anemia
- Sustained tachyarrhythmia or bradyarrhythmia
- Significant systemic hypotension (any cause)
Management focuses on identifying and treating the underlying imbalance, not simply antiplatelet therapy.
Type 3 - Sudden Cardiac Death Before Biomarker Sampling
Unexpected cardiac death with symptoms suggesting ischemia plus presumably new ST elevation or new LBBB, with fresh coronary thrombus found on angiography or autopsy - but death occurs before blood sampling can confirm elevated biomarkers.
Type 4 - PCI-Related MI
MI associated with percutaneous coronary intervention:
- In patients with normal baseline troponin, any elevation above the 99th percentile URL indicates periprocedural myocardial necrosis
- Values >3× the 99th percentile URL define PCI-related MI
- A subtype (Type 4b) includes stent thrombosis
Type 5 - CABG-Related MI
MI associated with coronary artery bypass grafting:
- In patients with normal baseline troponin, any elevation above the 99th percentile URL indicates periprocedural necrosis
- Values >5× the 99th percentile URL PLUS at least one of the following defines CABG-related MI:
- New pathologic Q waves or new LBBB
- Angiographically documented new graft or native coronary artery occlusion
- Imaging evidence of new loss of viable myocardium
(ROSEN's Emergency Medicine, p. 996-997; Sabiston Textbook of Surgery)
Summary Diagram
| Mechanism | Pathway |
|---|---|
| Vulnerable plaque | Large lipid core + thin cap + inflammation |
| Plaque rupture/erosion | Shear stress, adrenergic surge, proteases |
| Platelet activation | Exposed collagen + tissue factor |
| Thrombus | White (platelet) → Red (fibrin) |
| Partial occlusion | NSTEMI / Unstable Angina |
| Complete occlusion | STEMI |
| Myocardial ischemia >20-40 min | Irreversible necrosis (coagulative) |
Sources:
- ROSEN's Emergency Medicine, 9th ed., p. 995-997
- Robbins & Kumar Basic Pathology, p. 322
- Fuster and Hurst's The Heart, 15th ed., Ch. 16
- Washington Manual of Medical Therapeutics, p. 146
- Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.