Lasix drug MOA AND USE.
Reading File
Finding Sources
Searching PubMed
furosemide loop diuretic mechanism clinical use
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a complete breakdown of Lasix (Furosemide) - Mechanism of Action and Uses:
Lasix (Furosemide) - MOA and Clinical Uses
What Is It?
Furosemide (brand name Lasix, named because it "lasts six" hours) is a loop diuretic - the most potent class of diuretics available. It is the most commonly used drug in its class.
Mechanism of Action
Furosemide inhibits the Na⁺/K⁺/2Cl⁻ cotransporter located in the luminal membrane of the thick ascending limb of the loop of Henle.
Step-by-step mechanism:
- Furosemide is secreted into the tubular lumen at the proximal convoluted tubule (where it must reach to be effective)
- It blocks the Na⁺/K⁺/2Cl⁻ cotransporter, preventing reabsorption of Na⁺, K⁺, and Cl⁻ into the renal medulla
- This lowers the osmotic pressure of the medulla, so less water is reabsorbed from the descending limb
- The result is a large volume of dilute urine
Why it's the most potent diuretic: The ascending limb accounts for 25-30% of filtered NaCl reabsorption, and downstream sites (distal tubule, collecting duct) cannot compensate for the increased Na⁺ load.
Additional early effect - Venodilation: Before the diuretic effect kicks in, furosemide causes acute venodilation by enhancing prostaglandin synthesis, which reduces left ventricular filling pressures. This is why it helps in acute pulmonary edema even before significant urine output occurs.
Note: NSAIDs can blunt the diuretic effect by inhibiting renal prostaglandin synthesis.
Therapeutic Uses
| Indication | Notes |
|---|---|
| Acute pulmonary edema | Drug of choice; rapid IV onset + venodilation give fast relief |
| Chronic peripheral edema | Due to heart failure, hepatic cirrhosis, or renal impairment |
| Nephrotic syndrome | Reduces fluid overload |
| Hypertension | Especially when thiazides fail (e.g., GFR < 30 mL/min) |
| Hypercalcemia | Increases urinary Ca²⁺ excretion (used with IV hydration) |
| Hyperkalemia | Can be used with or without replacement IV fluids |
| Diuretic-resistant states | Effective even in patients with poor renal function |
Pharmacokinetics
- Route: Oral or IV/IM (IV preferred in emergencies)
- Oral bioavailability: Unpredictable - 10% to 90% (a major limitation vs. bumetanide/torsemide)
- Duration of action: ~6 hours
- Dose-response: Sigmoidal ("S"-shaped) curve - there is a threshold that must be crossed for any diuresis, a rapid rise, then a ceiling effect (doubling the dose won't increase diuresis further once ceiling is reached)
Clinical dosing tip: In hospitalized patients, the initial IV dose is typically 2-2.5 times the chronic oral dose. If no response in 2 hours, double the dose promptly.
Adverse Effects
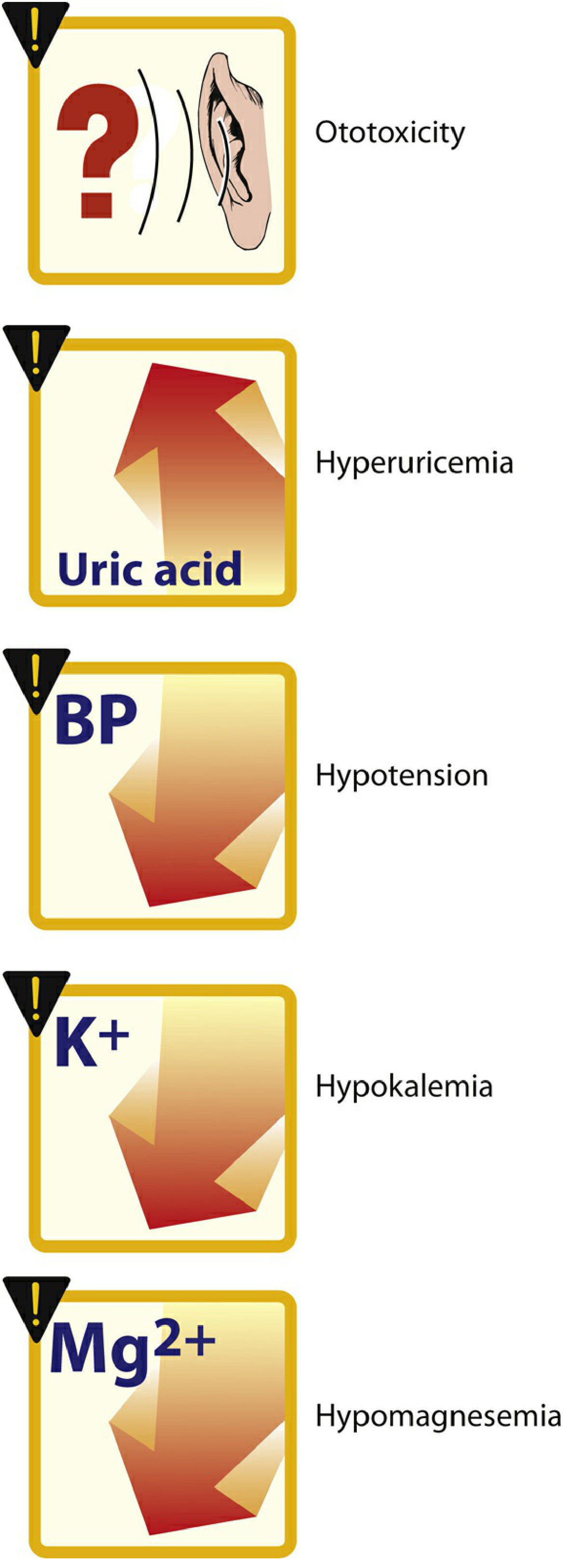
| Effect | Mechanism |
|---|---|
| Hypokalemia (most common) | Heavy Na⁺ load to collecting tubule → increased Na⁺/K⁺ exchange → K⁺ loss; causes hypokalemic alkalosis |
| Hypomagnesemia | Urinary Mg²⁺ loss |
| Hypovolemia / hypotension | Rapid, severe volume reduction; can cause shock or arrhythmias |
| Ototoxicity | Especially with rapid IV infusion, high doses, or co-use with aminoglycosides; usually reversible; ethacrynic acid is worst offender |
| Hyperuricemia / gout | Competes with uric acid for renal secretion, blocks uric acid excretion |
| Hyponatremia | Less common than with thiazides |
Prevention of hypokalemia: Co-prescribe potassium-sparing diuretics (e.g., spironolactone) or potassium supplements.
Key Comparisons Within Loop Diuretics
| Drug | Bioavailability | Notes |
|---|---|---|
| Furosemide (Lasix) | 10-90% (unpredictable) | Most widely used |
| Bumetanide | 80-100% | More potent, preferred oral |
| Torsemide | 80-100% | Longer duration, preferred oral |
| Ethacrynic acid | Variable | Rarely used; highest ototoxicity risk; used in sulfa allergy |
Source: Lippincott Illustrated Reviews: Pharmacology, Chapter 9 - Diuretics
This is a shared conversation. Sign in to Orris to start your own chat.