I am a postgraduate build a 10 marks answer about central retinal vein occlusion
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed. Here is the comprehensive postgraduate-level 10-mark answer:
Central Retinal Vein Occlusion (CRVO)
[Postgraduate Answer - 10 Marks]
Definition and Epidemiology
Central retinal vein occlusion (CRVO) is obstruction of the central retinal vein at or posterior to the lamina cribrosa, resulting in retinal venous stasis, haemorrhage, and oedema. It is the second most common retinal vascular disease after diabetic retinopathy, affecting approximately 5 in 1000 people in the industrialised world. Over 50% of cases occur in patients older than 65 years.
Pathogenesis
The central retinal vein and artery share a common adventitial sheath at the level of the optic nerve. Atherosclerotic thickening and rigidity of the artery compresses the adjacent vein at crossing points posterior to the lamina cribrosa, predisposing to:
- Endothelial cell loss and turbulent flow
- Thrombus formation within the vein
- Venous and capillary pressure elevation → retinal hypoxia
- Capillary endothelial damage, extravasation of blood constituents
- Liberation of VEGF and other angiogenic mediators
Haematological pro-thrombotic factors amplify this atherosclerotic anatomical predisposition in a minority of patients.
(Kanski's Clinical Ophthalmology, 10th ed.)
Risk Factors
| Category | Factors |
|---|---|
| Systemic | Hypertension (2/3 of patients >50 yrs), diabetes mellitus (~15%), hyperlipidaemia (~1/3), obesity |
| Ocular | Glaucoma and ocular hypertension (important independent risk factors for CRVO specifically) |
| Haematological | Myeloproliferative disorders (polycythaemia, myeloma), thrombophilia (hyperhomocysteinaemia, antiphospholipid antibody syndrome, Factor V Leiden mutation), dehydration |
| Inflammatory | Behcet syndrome, sarcoidosis, Wegener granulomatosis (periphlebitis) |
| Other | OCP use (especially younger women), smoking, chronic renal failure, orbital tumours/thyroid disease |
Classification
CRVO is classified based on the degree of retinal ischaemia:
| Feature | Non-ischaemic (Venous Stasis) | Ischaemic |
|---|---|---|
| Prevalence | More common | Less common |
| VA | Variable, often better than 6/60 | Usually CF or worse |
| RAPD | Absent or mild | Present |
| Haemorrhages | Mild-moderate, all 4 quadrants | Extensive, flame + deep blot |
| Cotton-wool spots | Mild | Prominent |
| FA capillary perfusion | Relatively preserved | >10 disc areas non-perfusion |
| NVI/NVG risk | Low | ~50% develop rubeosis (NVI) |
| Prognosis | ~50% recover near-normal vision | Generally very poor |
Classic Fundus Appearance
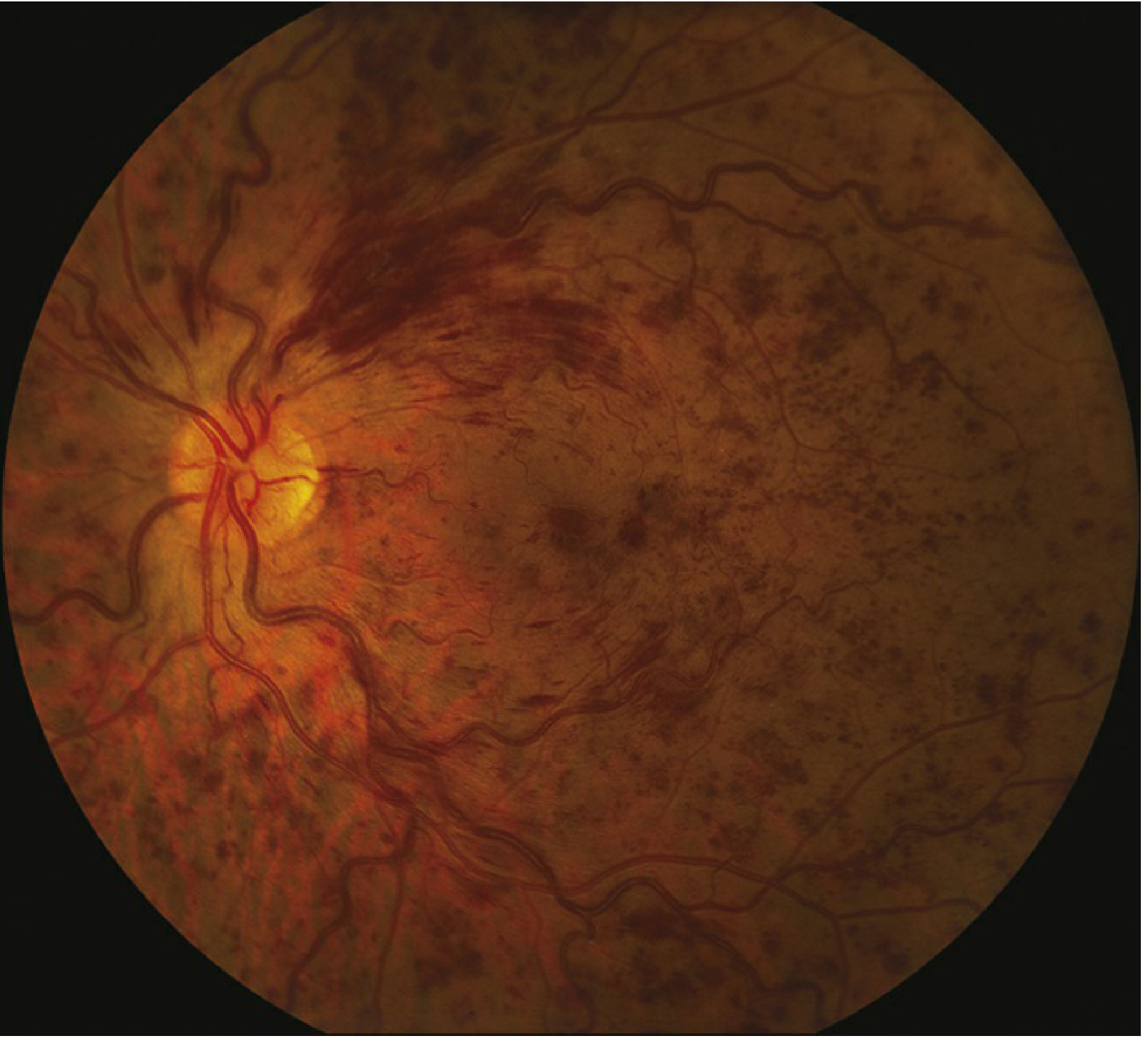
Fundus photograph showing CRVO: diffuse retinal haemorrhages in all four quadrants, markedly dilated and tortuous retinal veins, and disc oedema - the classic "blood and thunder" fundus. (Wills Eye Manual)
Critical signs:
- Diffuse retinal haemorrhages in all four quadrants (dot, blot, and flame-shaped)
- Marked dilatation and tortuosity of all branches of the CRV
- Disc oedema and hyperaemia
- Cotton-wool spots (ischaemic CRVO)
- Macular oedema
Late/sequelae findings: Disc collaterals (optociliary shunts), venous sclerosis and sheathing, epiretinal membrane, macular atrophy, retinal neovascularization (NVE, NVD).
Tip: A VA of <6/60 with a present RAPD strongly indicates significant ischaemia and a poor visual prognosis.
Investigations
- OCT - quantifies macular oedema (cystoid macular oedema, CMO); essential for treatment planning
- Fluorescein Angiography (FA) - key investigation:
- Non-ischaemic: delayed AV transit, masking by haemorrhage, good capillary perfusion, late leakage
- Ischaemic: extensive capillary non-perfusion (>10 disc areas), vessel wall staining, marked transit delay
- ERG - b-wave reduction indicates ischaemia; used to assess neovascular risk
- Gonioscopy - to detect angle neovascularization before pupil dilation at each visit
Systemic work-up (all patients):
- Blood pressure, FBC, ESR/plasma viscosity, random blood glucose, fasting lipids, plasma protein electrophoresis (to exclude myeloma), renal function (U&E, creatinine)
- In patients <50 years or bilateral/recurrent cases: thrombophilia screen (antiphospholipid antibodies, homocysteine, Factor V Leiden), vasculitis screen, autoimmune profile
Treatment
1. Systemic Management
- Treat hypertension, diabetes, hyperlipidaemia aggressively
- Discontinue OCP in women of reproductive age
2. Treatment of Macular Oedema
Treatment is indicated for VA worse than 6/9 and/or significant central macular thickening on OCT.
First-line: Intravitreal Anti-VEGF agents
- Ranibizumab (CRUISE trial) and aflibercept are approved; bevacizumab is used off-label
- Treatment regime: monthly injections for at least 6 months, then PRN or treat-and-extend
Second-line: Intravitreal Steroids
- Dexamethasone implant (Ozurdex) - sustained-release; effective for CMO; risk of IOP elevation and cataract
- Intravitreal triamcinolone - SCORE study showed >25% of patients gained 3+ lines at 1 year with 1 mg preservative-free preparation; higher IOP risk with 4 mg dose; generally reserved for pseudophakic eyes or when anti-VEGF is not feasible
Laser: Grid macular laser is NOT beneficial for visual outcome in CRVO (unlike BRVO) and is not recommended as primary treatment.
3. Treatment of Neovascularization (Ischaemic CRVO)
- Panretinal photocoagulation (PRP) is indicated promptly upon development of NVI or angle neovascularization - NOT before
- Initial: 1500-2000 burns (0.05-0.1 s, one burn width apart, moderate reaction)
- Adjunctive intravitreal anti-VEGF every 6 weeks until stabilization - promotes more rapid NV regression and reduces CMO
- Neovascular glaucoma (NVG) management: cyclodiode laser, aqueous suppressants, glaucoma drainage surgery
- Vitreous haemorrhage: intravitreal anti-VEGF as temporizing; definitive treatment = vitrectomy + endolaser
Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| Ocular ischaemic syndrome | Veins dilated but NOT tortuous; midperipheral haemorrhages; low IOP; may have orbital pain or amaurosis fugax |
| Diabetic retinopathy | Haemorrhages/microaneurysms concentrated at posterior pole; typically bilateral; FA differentiates |
| Papilledema | Bilateral disc swelling; haemorrhages peripapillary only; not diffuse all-quadrant haemorrhages |
| Hyperviscosity retinopathy | Bilateral; peripheral haemorrhages; check FBC and serum protein |
| Radiation retinopathy | History of irradiation; CWS-predominant |
Complications
- Chronic macular oedema - the principal cause of permanent visual loss
- Macular atrophy and RPE changes - from prolonged ischaemia
- Neovascular glaucoma ("100-day glaucoma") - NVI develops in ~50% of ischaemic CRVO eyes, classically at 2-4 months post-occlusion
- Retinal neovascularization - NVE occurs in ~5% (less common than in BRVO)
- Vitreous haemorrhage and tractional retinal detachment
- Epiretinal membrane formation
Prognosis
- Non-ischaemic CRVO: ~50% recover near-normal vision; ~1/3 progress to ischaemic form within months - close monitoring is essential
- Ischaemic CRVO: Poor visual prognosis due to macular ischaemia; aggressive treatment of complications required
Review schedule:
- Ischaemic: monthly for 6 months, then 3-monthly for 2-3 years
- Non-ischaemic: review at 3 months initially; follow for 18-24 months; patient instructed to report any deterioration (especially pain/redness suggesting NVG)
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed. | Wills Eye Manual, 8th ed. | Tintinalli's Emergency Medicine | Robbins & Cotran Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.