My working diagnosis is panic disorder. The patient is a 34-year-old woman with three ED visits for palpitations, sweating, and a feeling of doom. Don't confirm it- challenge it. Which findings would argue against panic disorder, and where might I be anchoring?
panic disorder misdiagnosis cardiac arrhythmia
panic disorder mimics cardiac endocrine diagnosis
panic disorder misdiagnosis pheochromocytoma hyperthyroidism
SVT supraventricular tachycardia panic disorder anxiety diagnosis delay
PMID: 40066143
Challenging "Panic Disorder" - Where Your Anchor May Be Wrong
Why the pattern looks like panic disorder (and why that's the trap)
Findings That Should Make You Uncomfortable
1. She Has NOT Had a Documented Attack During Monitoring
2. Supraventricular Tachycardia (SVT) - The Most Dangerous Mimic
- SVT has the same abrupt onset, palpitations, dyspnea, chest discomfort, and fear
- Episodes are self-terminating, so by the time the ED records an ECG, the rhythm has reverted
- The feeling of doom in SVT is real - it is not cognitive distortion, it is hemodynamic
- Red flags for SVT over panic: sudden onset with an equally sudden termination (not a gradual fade), palpitations that feel regular and very fast, near-syncope or frank syncope, episodes triggered by positional change or exertion, or relief with Valsalva
3. Pheochromocytoma - Rare But Catastrophic to Miss
- "The triad of palpitations, headache, and profuse sweating is the most sensitive and specific for pheochromocytoma" - Kaplan & Sadock's Comprehensive Textbook of Psychiatry
- "Paroxysmal attacks of headache, hypertension, sweating, and palpitations" - Morgan & Mikhail's Clinical Anesthesiology 7e
4. Hyperthyroidism
5. Carcinoid Syndrome
6. Hypoglycemia
Anchoring Biases at Play Here
| Bias | How it applies |
|---|---|
| Anchoring | The first clinician in ED #1 labeled it anxiety; every subsequent note confirmed that frame rather than re-evaluating it |
| Frequency bias | Panic disorder is common, pheo is rare - your prior pulls you toward panic even when the likelihood ratio for individual features hasn't been calculated |
| Demographic bias | "34-year-old woman with episodic anxiety" is a highly pattern-matched archetype; male patients with identical presentations get faster cardiac workups |
| Confirmation bias | Three visits and still no "dangerous" finding feels like confirmation, not like a gap in the workup |
| Premature closure | The diagnosis was reached before ruling out medical causes, not after |
What Should Already Be Done (and Often Isn't)
"When the history is nonspecific, physical examination and focused laboratory testing must be used to rule out anxiety states resulting from medical disorders such as pheochromocytoma, thyrotoxicosis, or hypoglycemia. ECG and echocardiogram may detect cardiovascular conditions." - Harrison's 22E, p. 3701
- ECG during a symptomatic episode - if none captured, arrange event/loop monitor or Holter
- TSH, free T4
- Fasting glucose or glucose during episode
- Plasma free metanephrines (or 24-hour urine catecholamines)
- Echocardiogram - to rule out MVP, structural disease
- Blood pressure during an attack - paroxysmal hypertension points toward pheo or SVT
The Question to Ask Yourself
Patient with fever, night sweats, and a mediastinal mass on CXR. Rank the differential by likelihood — then flag the one I can't afford to miss even if it's uncommon.
mediastinal mass fever lymphoma diagnosis
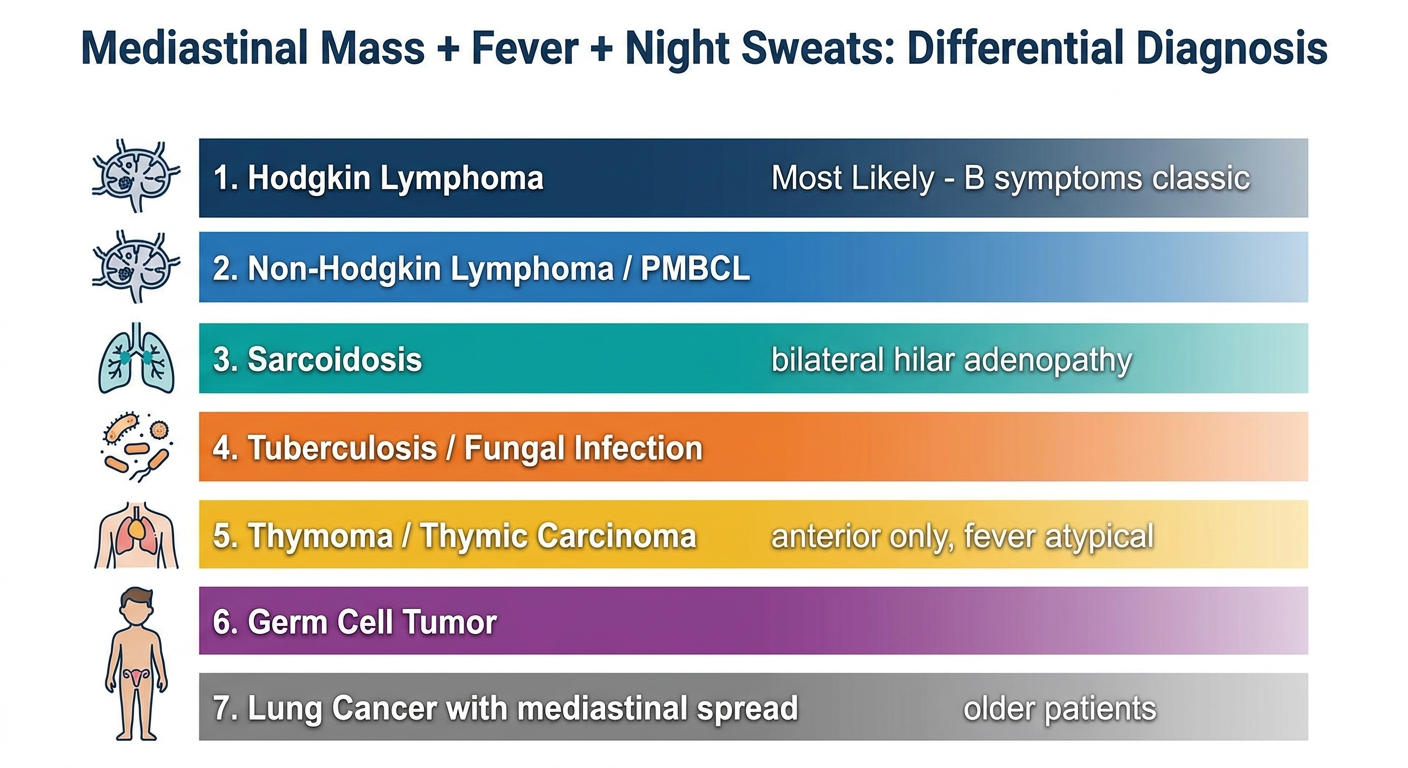
Mediastinal Mass + Fever + Night Sweats: Ranked Differential
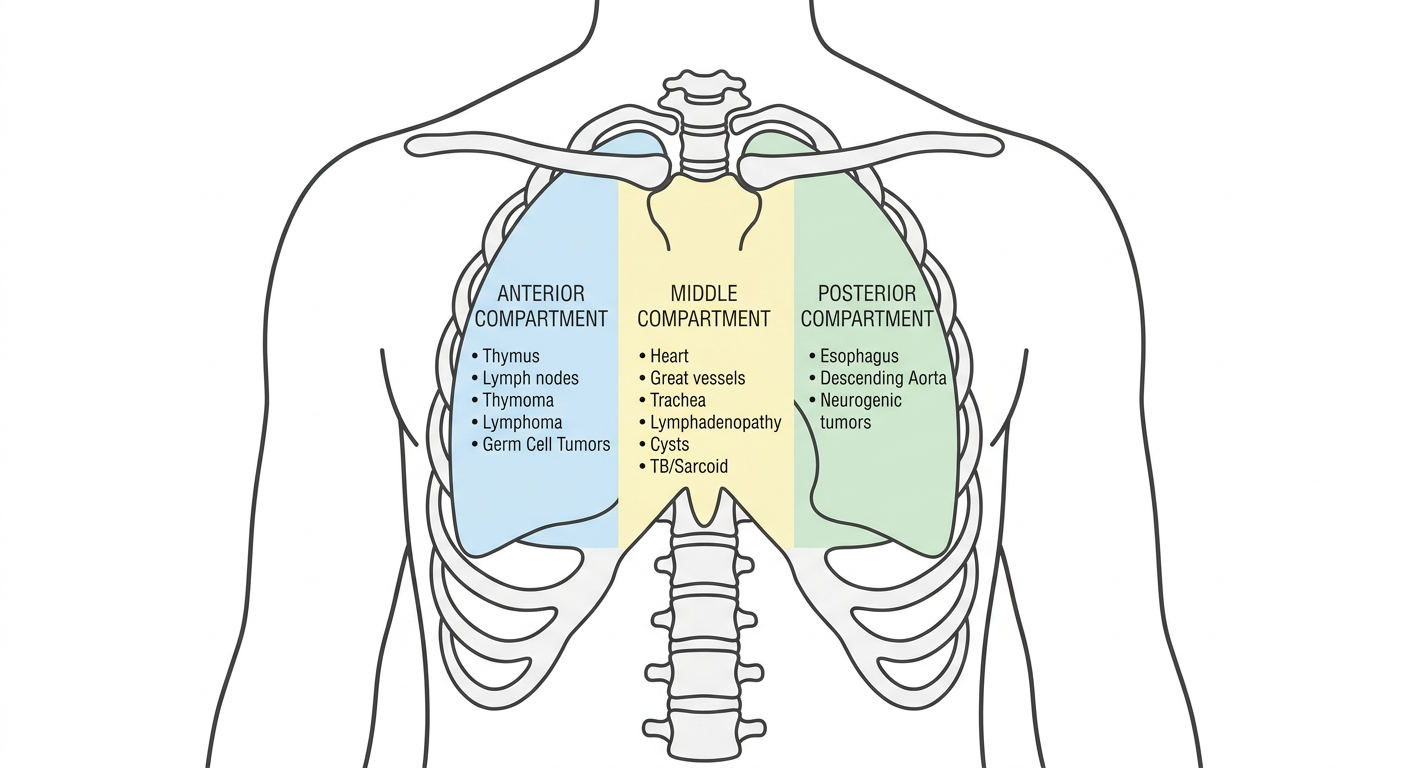
Step 0: Localize the Mass First
| Compartment | Anatomic boundaries | Most common masses |
|---|---|---|
| Anterior | Sternum/manubrium → pericardium/aorta | Thymoma, lymphoma, germ cell tumors, thyroid/parathyroid masses |
| Middle | Central vascular/bronchogenic structures | Lymphadenopathy (lymphoma, TB, sarcoid, metastatic), bronchogenic/pericardial cysts |
| Posterior | Pericardium/trachea → vertebral column | Neurogenic tumors, esophageal lesions, meningocele |
Ranked Differential (Anterior/Middle Predominance)
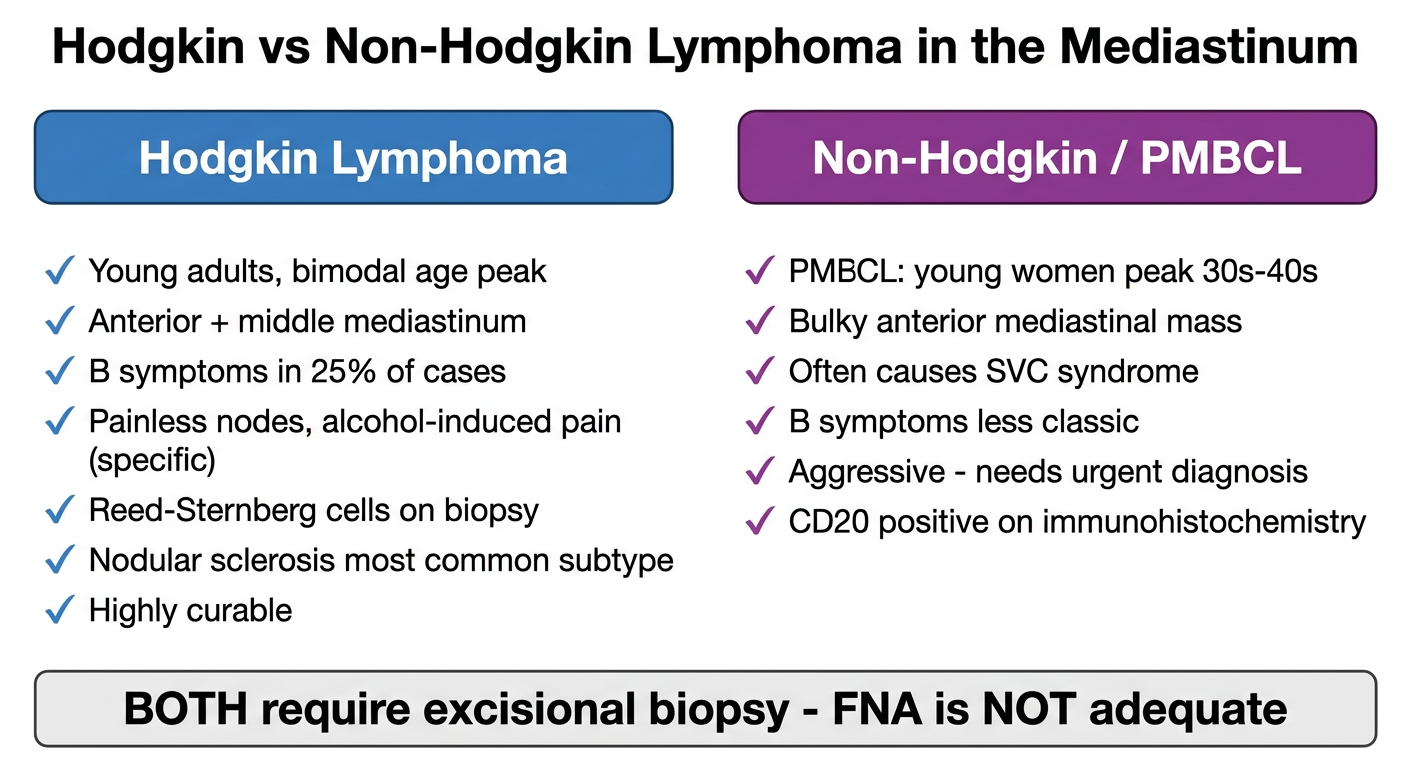
1. Hodgkin Lymphoma - Most Likely
2. Non-Hodgkin Lymphoma (including Primary Mediastinal Large B-Cell Lymphoma) - Very Likely
3. Sarcoidosis - Common, Often with Fever
4. Infectious Lymphadenitis - Tuberculosis / Endemic Fungi
- TB: Primary or reactivation can produce mediastinal/hilar adenopathy, fever, and drenching night sweats - the classic TB "B symptom" constellation. Risk factors: immigration history, HIV, exposure.
- Histoplasma capsulatum and Coccidioides: produce granulomatous mediastinal adenopathy with constitutional symptoms; geography matters (Ohio/Mississippi River valleys for histoplasma, Southwest US for cocci).
- Middle compartment mass is the common location.
5. Thymoma / Thymic Carcinoma - Less Common, Anterior Only
6. Mediastinal Germ Cell Tumor (GCT) - Young Men, Anterior
7. Lung Cancer with Mediastinal Involvement - Consider in Older Patients
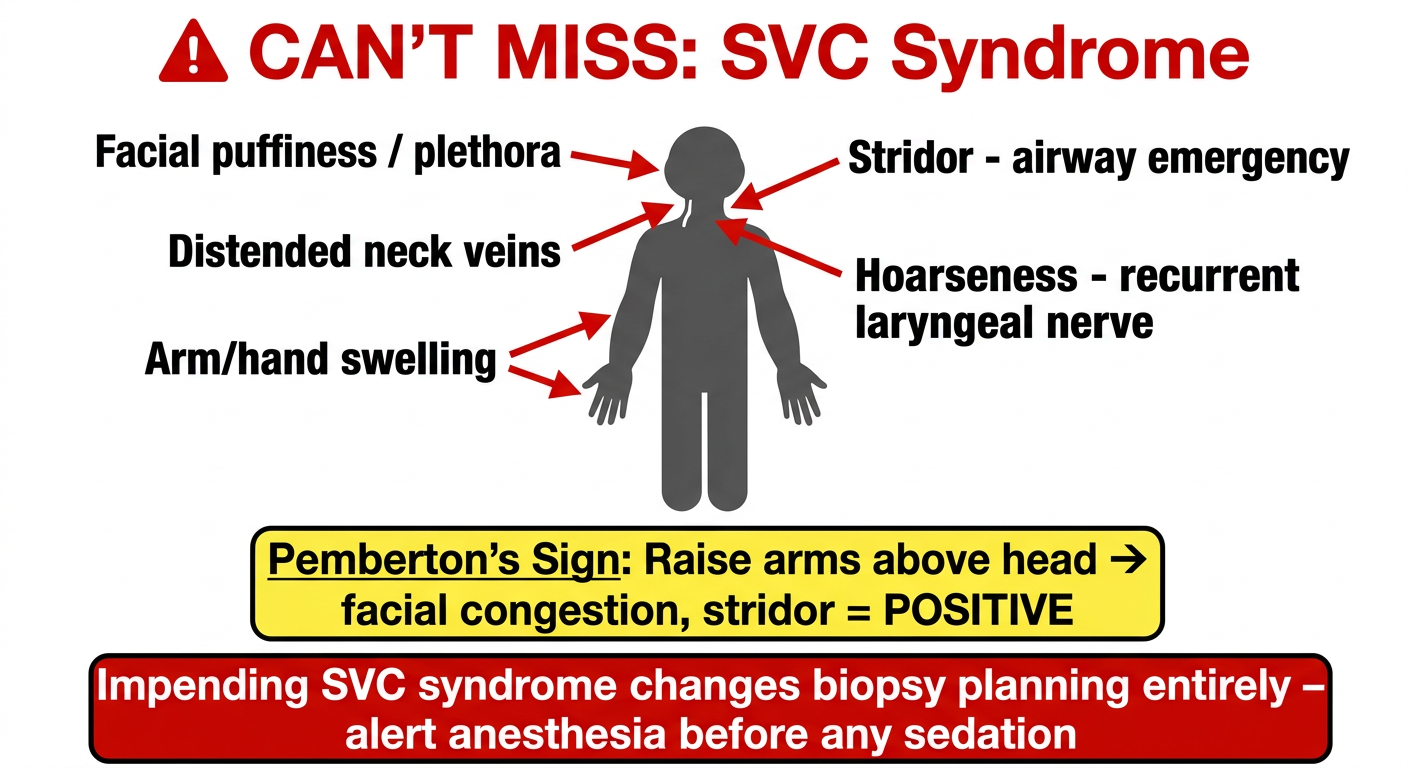
The One You Cannot Afford to Miss
⚠ Superior Vena Cava (SVC) Syndrome - Impending Emergency
- The mediastinal mass that looks stable on CXR may already be compressing or partially occluding the SVC
- Airway edema from SVC obstruction can cause acute respiratory failure
- Tracheal compression from a bulky anterior mediastinal mass (especially in lymphoma or GCT) can cause acute stridor - a surgical/airway emergency
- Laying the patient supine for biopsy or procedures can precipitate acute airway collapse
- Facial plethora or puffiness (worse in the morning)
- Dilated neck veins that do not collapse on sitting up
- Upper extremity venous distension or arm/hand edema
- Pemberton's sign (raising arms above head produces facial congestion, stridor, or presyncope)
- Hoarseness (recurrent laryngeal nerve compression)
- Stridor (tracheal/bronchial compression)
Workup Summary
| Step | Test | Target |
|---|---|---|
| CT chest with contrast | Characterize compartment, size, SVC patency, airway | All |
| CBC, LDH, ESR, uric acid | Lymphoma markers | HL/NHL |
| AFP, beta-hCG | Germ cell tumor | GCT (young male) |
| ACE, calcium, serum protein electrophoresis | Sarcoid, myeloma | Middle compartment |
| Sputum AFB, Quantiferon-TB, urine histoplasma antigen | Infectious | If geographic/clinical risk |
| Excisional biopsy (not FNA) | Definitive tissue diagnosis | Lymphoma |
| Pemberton's sign / assess for stridor | SVC syndrome / airway compromise | Immediate safety screen |
generate simple and easy to understand images and graphics for the same
Simple clean medical education diagram showing the three mediastinal compartments on a front-view chest outline. Label the anterior compartment (left side of chest) with its contents: Thymus, Lymph nodes, Thymoma, Lymphoma, Germ Cell Tumors. Label the middle compartment (center) with: Heart, Great vessels, Trachea, Lymphadenopathy, Cysts, TB/Sarcoid. Label the posterior compartment (right side) with: Esophagus, Descending Aorta, Neurogenic tumors. Use distinct soft colors for each compartment - light blue for anterior, light yellow for middle, light green for posterior. Include a simple lung outline and spine. Clean white background, minimal text, easy to read font.
Simple ranked list infographic for medical education. Title: "Mediastinal Mass + Fever + Night Sweats: Differential Diagnosis". Show a vertical ranked list from most to least likely with bold numbered labels and simple icons next to each: 1. Hodgkin Lymphoma - lymph node icon, dark blue bar, labeled "Most Likely - B symptoms classic". 2. Non-Hodgkin Lymphoma / PMBCL - similar node icon, blue bar. 3. Sarcoidosis - lung icon, teal bar, "bilateral hilar adenopathy". 4. Tuberculosis / Fungal Infection - bacteria icon, orange bar. 5. Thymoma / Thymic Carcinoma - chest icon, yellow bar, "anterior only, fever atypical". 6. Germ Cell Tumor - young male icon, purple bar. 7. Lung Cancer with mediastinal spread - gray bar, "older patients". Clean white background, simple horizontal bars showing probability gradient from high to low, easy to read.
Simple medical education warning card graphic. Title at top in bold red: "⚠ CAN'T MISS: SVC Syndrome". Show a simple front-body silhouette with arrows pointing to warning signs labeled around the figure: "Facial puffiness / plethora" pointing to face, "Distended neck veins" pointing to neck, "Arm/hand swelling" pointing to arms, "Stridor - airway emergency" pointing to throat, "Hoarseness - recurrent laryngeal nerve" pointing to neck side. Below the figure, a yellow warning box with bold text: "Pemberton's Sign: Raise arms above head → facial congestion, stridor = POSITIVE". Bottom red box: "Impending SVC syndrome changes biopsy planning entirely - alert anesthesia before any sedation". Clean white background, clear bold fonts, red and yellow warning colors, simple stick figure or silhouette style.
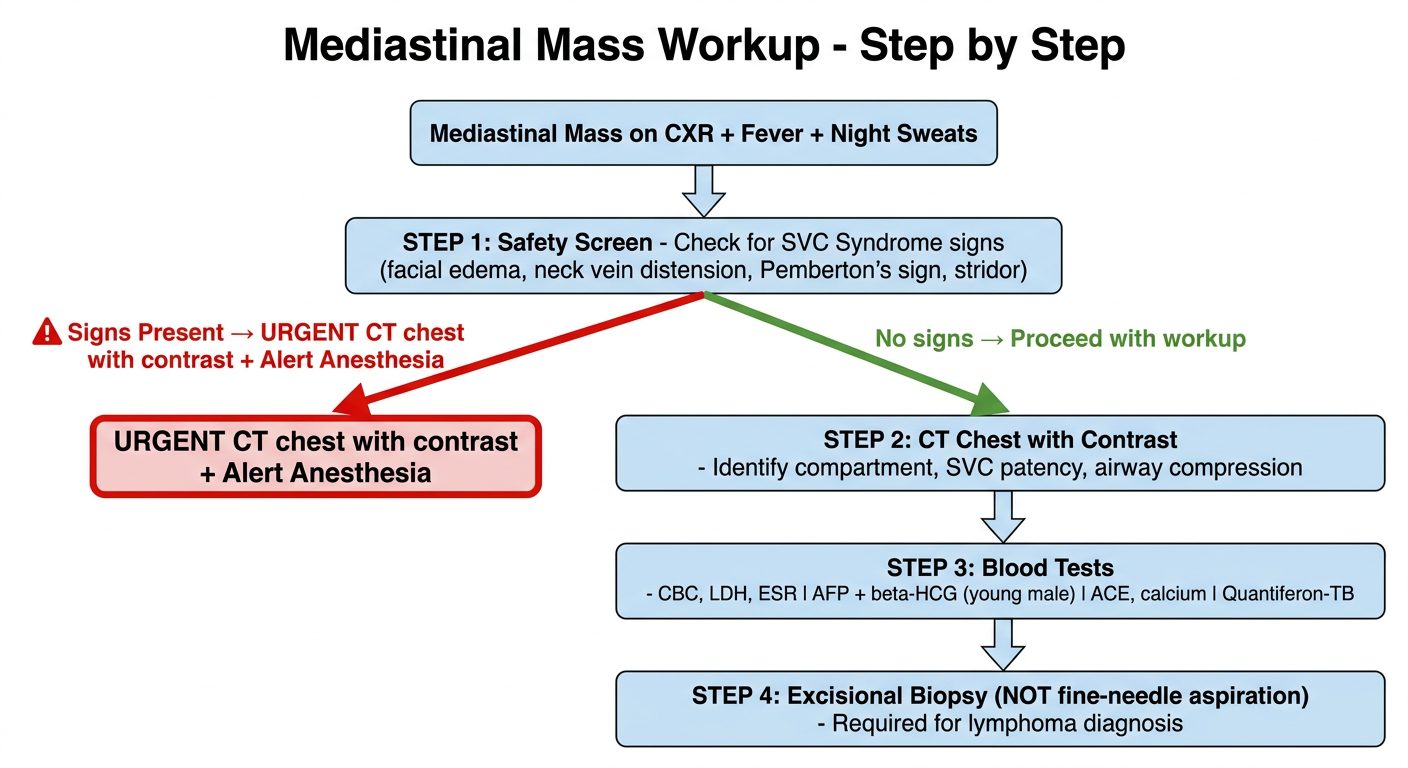
Clean medical education flowchart diagram. Title: "Mediastinal Mass Workup - Step by Step". Start with a box at the top: "Mediastinal Mass on CXR + Fever + Night Sweats". Arrow down to: "STEP 1: Safety Screen - Check for SVC Syndrome signs (facial edema, neck vein distension, Pemberton's sign, stridor)". Two arrows from this box - one red arrow labeled "Signs Present → URGENT CT chest with contrast + Alert Anesthesia" and one green arrow labeled "No signs → Proceed with workup". Arrow down to: "STEP 2: CT Chest with Contrast - Identify compartment, SVC patency, airway compression". Arrow down to: "STEP 3: Blood Tests - CBC, LDH, ESR | AFP + beta-HCG (young male) | ACE, calcium | Quantiferon-TB". Arrow down to: "STEP 4: Excisional Biopsy (NOT fine-needle aspiration) - Required for lymphoma diagnosis". Clean white background, light blue boxes, red warning box for SVC, simple arrows, easy to read.
Simple medical education comparison card. Title: "Hodgkin vs Non-Hodgkin Lymphoma in the Mediastinum". Two columns side by side. Left column header "Hodgkin Lymphoma" in blue box: checkmark list - "Young adults, bimodal age peak", "Anterior + middle mediastinum", "B symptoms in 25% of cases", "Painless nodes, alcohol-induced pain (specific)", "Reed-Sternberg cells on biopsy", "Nodular sclerosis most common subtype", "Highly curable". Right column header "Non-Hodgkin / PMBCL" in purple box: checkmark list - "PMBCL: young women peak 30s-40s", "Bulky anterior mediastinal mass", "Often causes SVC syndrome", "B symptoms less classic", "Aggressive - needs urgent diagnosis", "CD20 positive on immunohistochemistry". Bottom row: shared box "BOTH require excisional biopsy - FNA is NOT adequate". Clean white background, simple two-column layout, clear fonts.
1. Mediastinal Compartments - Anatomy Map
2. Ranked Differential - Probability Ladder
3. The "Can't Miss" - SVC Syndrome Warning Card
4. Step-by-Step Workup Flowchart
5. Hodgkin vs. Non-Hodgkin Comparison