Anti tubercular drugs
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching PubMed
tuberculosis treatment regimen drug resistant
I now have all the information needed for a comprehensive, well-sourced answer. Let me compose it.
Anti-Tubercular Drugs
Anti-tubercular drugs (ATDs) are divided into first-line and second-line agents. Effective treatment always requires a combination of drugs to prevent resistance and achieve sterilization of both rapidly dividing and dormant ("persister") mycobacteria.
Standard Treatment Regimen
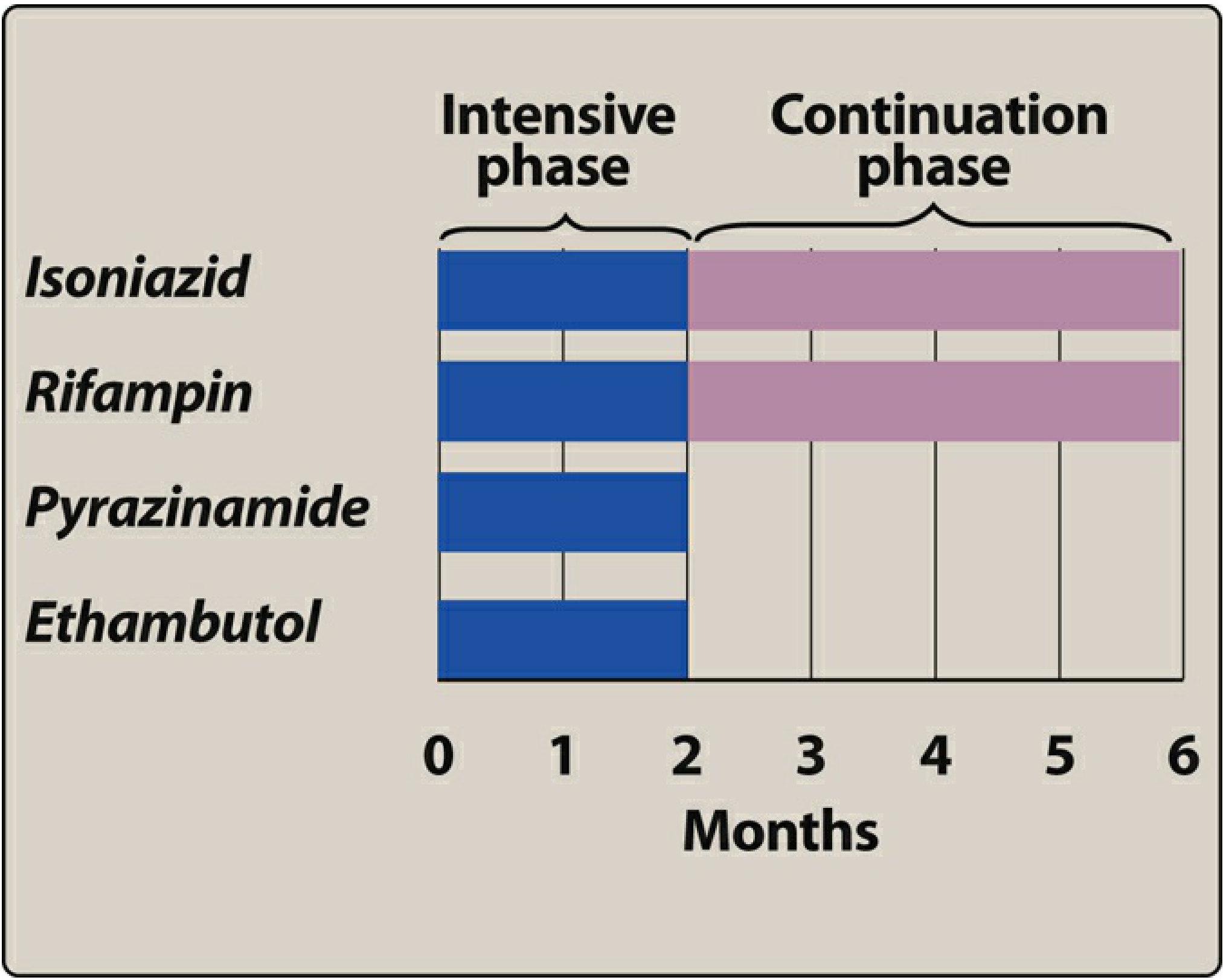
The traditional regimen consists of two phases:
- Intensive phase (2 months): Isoniazid (H) + Rifampin (R) + Pyrazinamide (Z) + Ethambutol (E) - mnemonic: HRZE
- Continuation phase (4 months): Isoniazid + Rifampin - mnemonic: HR
A newer 4-month regimen (rifapentine + moxifloxacin + isoniazid + pyrazinamide) has shown non-inferiority to standard therapy for drug-susceptible pulmonary TB. (Katzung's Basic and Clinical Pharmacology, 16th Ed.)
First-Line Drugs
1. Isoniazid (INH / H)
| Property | Detail |
|---|---|
| Mechanism | Prodrug activated by mycobacterial KatG catalase-peroxidase. Activated form inhibits InhA (ketoenoyl-reductase) and KasA (β-ketoacyl-ACP synthase), blocking mycolic acid synthesis. Also releases bactericidal free radicals (including nitric oxide). |
| Spectrum | Highly specific for M. tuberculosis; M. kansasii may be susceptible at higher concentrations. Active against both rapidly dividing and intracellular organisms. |
| Dose | 5 mg/kg/day in adults (max 300 mg/day); 10-15 mg/kg/day in children |
| Pharmacokinetics | Oral bioavailability high; distributes well into all body fluids including CSF. Metabolized by NAT2 (N-acetyltransferase 2) - fast vs slow acetylator phenotypes affect levels and toxicity. Bimodal half-life: ~90 min (fast) vs 3-4 hours (slow). |
| Adverse effects | Peripheral neuropathy (prevented by pyridoxine 25-50 mg/day), hepatotoxicity (most serious; idiosyncratic, more common in slow acetylators and older patients), drug-induced lupus, CNS toxicity (seizures, psychosis) |
| Drug interactions | Inhibits CYP450; raises levels of phenytoin, carbamazepine, warfarin, benzodiazepines |
| Resistance | Mutation/deletion of KatG; mutations in InhA; overexpression of InhA. Cross-resistance with ethionamide. |
(Harrison's Principles of Internal Medicine 22E; Lippincott Illustrated Reviews: Pharmacology)
2. Rifampin (Rifampicin / R)
| Property | Detail |
|---|---|
| Mechanism | Blocks bacterial RNA transcription by binding to the beta-subunit of RNA polymerase (rpoB gene product). Bactericidal against rapidly dividing and dormant bacteria. |
| Spectrum | Broad - M. tuberculosis, M. leprae, MAC, Staphylococcus, Neisseria meningitidis (prophylaxis). |
| Dose | 600 mg/day (10 mg/kg/day, max 600 mg) |
| Pharmacokinetics | Well-absorbed orally; widely distributed including CNS and macrophages. Strong CYP450 inducer. Hepatic metabolism; excreted primarily in bile/feces. Turns body fluids (urine, tears, sweat) orange-red. |
| Adverse effects | Flu-like syndrome (especially with intermittent dosing), hepatotoxicity, thrombocytopenia, orange discoloration of body fluids, GI disturbance |
| Drug interactions | Major CYP450 inducer - reduces levels of antiretrovirals (HIV drugs), oral contraceptives, warfarin, methadone, cyclosporin, and many others |
| Resistance | Single-step mutations in rpoB. Resistance to rifampin alone is uncommon but signals MDR-TB when combined with INH resistance. |
Rifampin must never be used as monotherapy for active TB due to rapid resistance development.
3. Pyrazinamide (PZA / Z)
| Property | Detail |
|---|---|
| Mechanism | Prodrug converted to pyrazinoic acid (POA) by mycobacterial pyrazinamidase. POA accumulates in acidic environment (within macrophage phagolysosomes), disrupting membrane energy and fatty acid synthesis. Bactericidal against slowly replicating, intracellular organisms. |
| Spectrum | Essentially limited to M. tuberculosis. Active in acidic pH (found inside macrophages and in caseous lesions). |
| Dose | 25 mg/kg/day (max ~2 g/day) |
| Pharmacokinetics | Well-absorbed orally; good CSF penetration. Hepatic metabolism. |
| Adverse effects | Hepatotoxicity (dose-dependent), hyperuricemia (inhibits urate excretion - can precipitate gout), arthralgia, GI disturbance. |
| Special note | Its inclusion in the intensive phase allows total treatment duration to be shortened from 9 to 6 months. Not routinely recommended in pregnancy in the USA (inadequate teratogenicity data). |
| Resistance | Mutations in pncA gene (pyrazinamidase enzyme). |
4. Ethambutol (EMB / E)
| Property | Detail |
|---|---|
| Mechanism | Bacteriostatic. Inhibits arabinosyltransferases, blocking the formation of arabinogalactan and lipoarabinomannan in the mycobacterial cell wall. |
| Spectrum | M. tuberculosis, M. kansasii, M. marinum, MAC. Least potent first-line drug. |
| Dose | 15-25 mg/kg/day |
| Pharmacokinetics | 75-80% oral absorption; poor CSF penetration (25 mg/kg needed). Excreted by kidneys - dose reduction required in renal insufficiency. |
| Adverse effects | Optic neuritis (most serious - dose-dependent; presents as reduced visual acuity, central scotoma, loss of red-green color discrimination). Risk increases with high dose and renal impairment. Usually reversible if caught early. |
| Monitoring | Baseline and monthly visual acuity, color vision testing required. Avoid routine use in young children (cannot report visual changes). |
| Role | Fourth drug added in case organism is INH or RIF resistant; can be dropped once susceptibility is confirmed. |
5. Rifapentine
A long-acting rifamycin used in the newer 4-month regimen (with moxifloxacin, isoniazid, pyrazinamide) and in 3-month weekly LTBI (latent TB) treatment. Dose: 1200 mg once daily. (Katzung)
Second-Line Drugs
Used when first-line agents fail, cause severe toxicity, or organisms are resistant (MDR-TB/XDR-TB).
| Drug | Class | Key Mechanism | Notable Adverse Effects |
|---|---|---|---|
| Bedaquiline | Diarylquinoline | Inhibits mycobacterial ATP synthase (F0 subunit) - novel mechanism | QTc prolongation, hepatotoxicity |
| Linezolid | Oxazolidinone | Inhibits 23S rRNA (50S ribosomal subunit), blocks protein synthesis | Peripheral neuropathy, optic neuropathy, myelosuppression |
| Moxifloxacin / Levofloxacin | Fluoroquinolones | Inhibit DNA gyrase (topoisomerase II) | QTc prolongation, tendinopathy |
| Pretomanid | Nitroimidazole | Inhibits mycolic acid synthesis; bactericidal under both aerobic and anaerobic conditions | Hepatotoxicity, peripheral neuropathy |
| Cycloserine | Amino acid analogue | Inhibits D-alanine racemase and D-Ala-D-Ala ligase (cell wall synthesis) | CNS toxicity (psychosis, seizures, depression) |
| Ethionamide / Prothionamide | Thioamide | Structural analogue of INH; blocks InhA (mycolic acid synthesis) | GI intolerance, hepatotoxicity, peripheral neuropathy |
| Amikacin / Kanamycin | Aminoglycosides | Bind 30S ribosomal subunit; disrupt protein synthesis | Nephrotoxicity, ototoxicity |
| Capreomycin | Polypeptide | Inhibits translation at 70S ribosome | Nephrotoxicity, ototoxicity |
| Aminosalicylic acid (PAS) | PABA analogue | Inhibits folate synthesis in mycobacteria; also inhibits salicylate biosynthesis | GI intolerance, hepatotoxicity |
| Rifabutin | Rifamycin | Same as rifampin (RNA polymerase inhibition) | Less CYP induction than rifampin - preferred with HIV antiretrovirals |
| Clofazimine | Phenazine | Binds DNA; generates cytotoxic oxygen radicals | Skin/GI discoloration (pink to brownish-black), enteritis |
| Streptomycin | Aminoglycoside | Binds 16S rRNA on 30S ribosome; bactericidal | Ototoxicity (vestibular > cochlear), nephrotoxicity |
(Katzung 16th Ed., Harrison's 22E)
MDR-TB and XDR-TB Regimens
- MDR-TB (resistant to INH + Rifampin): WHO now recommends the BPaL or BPaLM regimen - Bedaquiline + Pretomanid + Linezolid (± Moxifloxacin) for 6 months. A 2025 systematic review (PMID 39813501) confirms BPaLM achieves high treatment success rates with acceptable safety.
- XDR-TB (MDR + fluoroquinolone + injectable resistance): BPaL regimen (bedaquiline + pretomanid + linezolid).
Summary Mnemonic - First-Line Drugs
RIPE (or HRZE):
- R - Rifampin
- I - Isoniazid
- P - Pyrazinamide
- E - Ethambutol
Key adverse effect mnemonics:
- H (INH): Hepatitis, Hypersensitivity, Hyperreflexia/neuropathy (B6 deficient)
- R (Rifampin): Red-orange secretions, Rashes, enzyme inducer
- Z (PZA): Zap the uric acid (hyperuricemia), hepatotoxicity
- E (Ethambutol): Eye toxicity (optic neuritis)
Sources: Harrison's Principles of Internal Medicine 22E, p. 1462-1470 | Lippincott Illustrated Reviews: Pharmacology, pp. 1054-1066 | Katzung's Basic and Clinical Pharmacology, 16th Ed., pp. 1312-1325
This is a shared conversation. Sign in to Orris to start your own chat.