Brief Explanation of Sleep Apnea with clinical treatment, Etiology
Reading File
Finding Sources
Searching PubMed
"sleep apnea"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Sleep Apnea: Explanation, Etiology, and Clinical Treatment
Definition and Types
Sleep apnea is a disorder characterized by repetitive episodes of absent (apnea) or attenuated (hypopnea) upper airway airflow lasting at least 10 seconds during sleep, resulting in progressive asphyxia, sleep fragmentation, and a wide range of systemic consequences. Episodes may occur 300-500 times per night in severe cases.
There are three recognized types:
| Type | Mechanism |
|---|---|
| Obstructive (OSA) | Upper airway collapse with continued (often forceful) ventilatory effort |
| Central (CSA) | Transient cessation of the neural drive to respiratory muscles - no ventilatory effort |
| Mixed | Combination of both; accounts for ~15% of all cases |
Etiology and Risk Factors
Obstructive Sleep Apnea (OSA)
The pharyngeal musculature normally maintains airway patency during sleep, but in susceptible individuals, relaxation during sleep causes complete or partial obstruction. Contributing factors include:
- Obesity - excess fat deposition in pharyngeal soft tissues or compression from cervical fat masses; reduction in tongue fat volume accounts for part of the association between weight loss and decreased apnea-hypopnea index (AHI)
- Anatomic abnormalities - retrognathia, micrognathia, enlarged tonsils/adenoids, a large tongue, redundant soft palate, or nasal obstruction
- Age - upper airway muscle tone declines with age
- Male sex - disproportionate pharyngeal fat distribution
- Craniofacial variants - certain palate shapes that increase airway resistance
- Central obesity - mechanically restricts chest wall and triggers reflex upper airway narrowing
- Alcohol, sedatives, opioids - relax upper airway musculature, worsen obstruction
In obesity, chest wall movement is restricted, causing mechanical and reflex upper airway narrowing, increased upper airway compliance, ventilatory instability, and an impaired ability to compensate for increased upper airway resistance. During REM sleep, erratic neural drive and descending inhibition of accessory ventilatory muscles lead to severe alveolar hypoventilation.
(Goldman-Cecil Medicine, p. 3906-3907; Guyton and Hall Textbook of Medical Physiology, p. 539)
Central Sleep Apnea (CSA)
- Cheyne-Stokes breathing variant is common in heart failure - driven by changes in lung volume, circulatory delay, and an augmented ventilatory response to blood gas changes, creating oscillation between apnea and hyperpnea
- Idiopathic - unknown cause; instability of CO2/H+ chemosensitivity
- Neurologic injury - strokes or brainstem lesions impairing respiratory center responsiveness
- Medication-induced - opioids, sedatives, and CNS depressants blunt CO2 drive
- Treatment-emergent CSA ("complex sleep apnea") - emerges after initiating CPAP for OSA
(Goldman-Cecil Medicine, p. 3907)
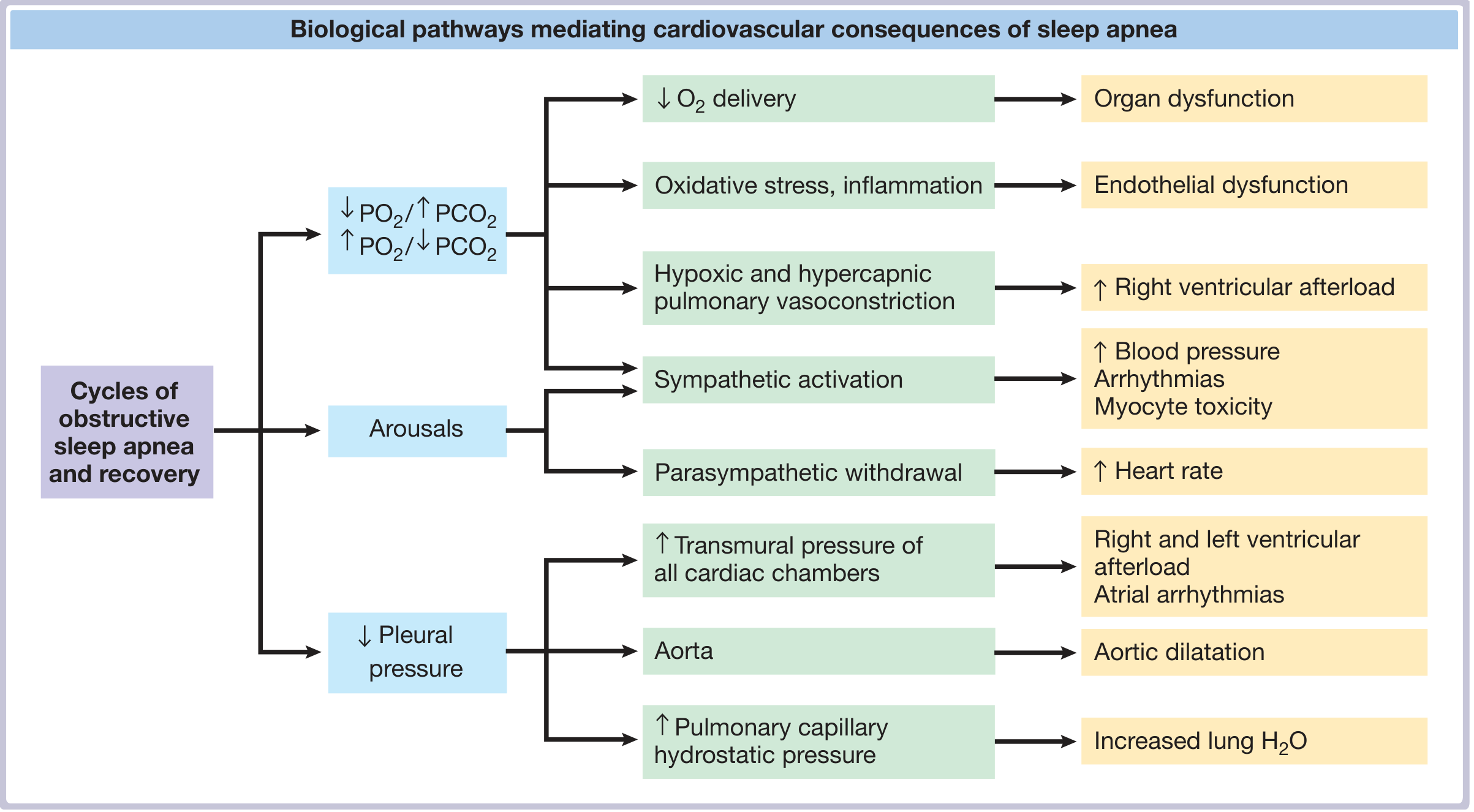
Pathophysiology
With each obstructive event:
- Progressive asphyxia occurs (↓ PO2, ↑ PCO2)
- Increasingly negative intrathoracic pressure is generated as the patient struggles against the obstructed airway
- Autonomic arousal terminates the event - causing peripheral vasoconstriction, tachycardia, and a spike in systemic blood pressure
- Acute cardiac effects include: increased left and right ventricular afterload, decreased left ventricular compliance, increased pulmonary artery pressure, decreased coronary artery blood flow, and increased myocardial O2 demand
Repetitive nightly cycling of hypoxia-reoxygenation creates chronic sympathetic activation, oxidative stress, and endothelial dysfunction - the mechanistic bridge to cardiovascular disease.
Clinical Manifestations
Symptoms (OSA):
- Loud, chronic snoring
- Witnessed apneas, choking, or gasping during sleep
- Excessive daytime somnolence (present in ~50% of OSA patients)
- Morning headache and dry mouth
- Mood disturbances - depression, irritability
- Impaired working memory and visual memory
- Nocturia (mediated via atrial natriuretic peptide)
- Night sweats, restless sleep
- Insomnia (from repetitive arousals)
- Confusional parasomnias (sleepwalking, sleep talking) from arousals during N3
Associated conditions:
- Systemic and pulmonary hypertension
- Cardiac arrhythmias (including atrial fibrillation)
- Coronary artery disease and increased sudden death risk
- Type 2 diabetes / metabolic syndrome
- Stroke
(Goldman-Cecil Medicine, p. 3907-3908)
Diagnosis: Polysomnography (PSG) remains the gold standard. The Apnea-Hypopnea Index (AHI) grades severity:
- Mild: AHI 5-14
- Moderate: AHI 15-29
- Severe: AHI ≥ 30
The Epworth Sleepiness Scale quantifies daytime somnolence (score >10 is abnormal). The STOP-Bang questionnaire is used for perioperative screening.
Clinical Treatment
1. Positive Airway Pressure (PAP) - First-Line for Moderate-Severe OSA
- CPAP (Continuous Positive Airway Pressure) - pneumatically splints the upper airway open; the most effective and widely used treatment. Reliably reduces AHI, improves oxygenation, reduces daytime sleepiness, and lowers blood pressure.
- BiPAP (Bilevel PAP) - provides different inspiratory and expiratory pressures; useful in patients who cannot tolerate CPAP, those with hypoventilation syndromes, or in CSA
- Autotitrating CPAP (APAP) - automatically adjusts pressure in response to airflow changes; at high altitude, adding acetazolamide to APAP has been shown to decrease central apneas and improve nocturnal oxygenation
2. Oral Appliances (Mandibular Advancement Devices)
- Reposition the mandible and tongue forward, increasing upper airway caliber
- Appropriate for mild-moderate OSA or CPAP-intolerant patients
- Less effective than CPAP for severe OSA but better tolerated
3. Hypoglossal Nerve Stimulation
- Implantable device that electrically stimulates the hypoglossal nerve (CN XII) during inspiration, protracting the tongue and opening the airway
- FDA-approved for moderate-severe OSA in CPAP-intolerant patients
4. Positional Therapy
- For positional OSA (supine-dependent), avoiding the supine position with positional devices or alarms can significantly reduce AHI
- First-line adjunct for positional cases
5. Weight Loss
- Reductions in pharyngeal fat (especially tongue fat) directly reduce AHI
- Can achieve remission of OSA in obese patients; bariatric surgery is highly effective in severe obesity
6. Exercise
- Independent of weight loss, regular exercise reduces AHI and daytime sleepiness via effects on upper airway muscle tone and fluid redistribution
7. Surgical Options
- Uvulopalatopharyngoplasty (UPPP) - removes excess soft palate tissue, tonsils, and uvula; success rates variable
- Tonsillectomy/adenoidectomy - highly effective in children with OSA
- Tracheostomy - bypasses the obstructed upper airway entirely; reserved for life-threatening refractory cases
8. Avoidance of Aggravating Factors
- Alcohol, smoking, phosphodiesterase-5 inhibitors (e.g., sildenafil), and opioids all worsen OSA and should be avoided, especially in the evening
9. Treatment of Edema
- Fluid redistribution to the neck during recumbency (from peripheral edema) worsens pharyngeal narrowing; diuretics and compression stockings can reduce this
Treatment of Central Sleep Apnea
- CPAP/BiPAP - first step, especially in heart failure-related CSA
- Adaptive Servo-Ventilation (ASV) - actively adjusts inspiratory pressure to counteract ventilatory instability; effective for Cheyne-Stokes breathing, but contraindicated in heart failure with EF < 45% due to increased mortality (SERVE-HF trial)
- Phrenic nerve stimulation - implanted device (Remedē System) that stimulates the phrenic nerve transvenously to trigger diaphragmatic contractions
- Cardiac resynchronization therapy (CRT) - in heart failure patients, CRT can reduce central apneas by improving cardiac output and reducing pulmonary congestion
- Drug therapy - acetazolamide (stimulates respiration via metabolic acidosis), theophylline, and low-dose oxygen have been used but evidence is limited
(Fuster & Hurst's The Heart, 15th Ed., p. 1793-1799; Goldman-Cecil Medicine; Guyton & Hall Medical Physiology, p. 539-540)
Summary Table
| Category | Key Points |
|---|---|
| Definition | Recurrent apneas/hypopneas ≥10 sec during sleep |
| Types | Obstructive (most common), Central, Mixed |
| Main risk factors | Obesity, male sex, age, craniofacial anatomy, alcohol/opioids |
| Cardinal symptoms | Snoring, witnessed apneas, excessive daytime sleepiness |
| Diagnosis | Polysomnography, AHI grading |
| First-line treatment | CPAP for moderate-severe OSA |
| Adjuncts | Oral appliance, weight loss, positional therapy, surgery |
| CSA treatment | BiPAP, ASV (with caution), phrenic nerve stimulation |
| Cardiovascular risk | HTN, arrhythmias, CAD, heart failure, stroke |
Sources:
- Goldman-Cecil Medicine, International Edition (2-Vol Set), pp. 3906-3910
- Guyton and Hall Textbook of Medical Physiology, pp. 539-540
- Fuster and Hurst's The Heart, 15th Edition, pp. 1787-1799
- Murray & Nadel's Textbook of Respiratory Medicine
- Miller's Anesthesia, 10th Edition
This is a shared conversation. Sign in to Orris to start your own chat.