Upper respiratory tract presentations in opd and emergency separately
Reading File
Finding Sources
Finding Sources
Searching the Web
upper respiratory tract presentations OPD vs emergency clinical approach
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive structured overview of upper respiratory tract (URT) presentations separated by OPD (outpatient) and Emergency settings.
Upper Respiratory Tract Presentations
PART 1 - OPD (Outpatient) Presentations
These are conditions that are generally non-life-threatening, self-limiting, or manageable without urgent airway intervention.
1. Common Cold (Viral URI)
-
Cause: Rhinovirus (most common), coronavirus, RSV, parainfluenza
-
Presentation: Nasal congestion, runny nose, sneezing, mild sore throat, low-grade or no fever, mild myalgia
-
Duration: 7-15 days; airway hyperreactivity may persist up to 8 weeks
-
Management: Symptomatic - decongestants, antihistamines, analgesics. No antibiotics.
-
Key point: Children average 6-8 URIs per year. Elective surgeries requiring airway manipulation should be deferred 4 weeks after active URI.
-
Cummings Otolaryngology, p. 1494-1498
2. Pharyngitis / Tonsillitis
- Cause: Viral (majority) or Group A Streptococcus (S. pyogenes) - the most common bacterial cause (20-40% of pediatric cases, 5-15% of adult cases)
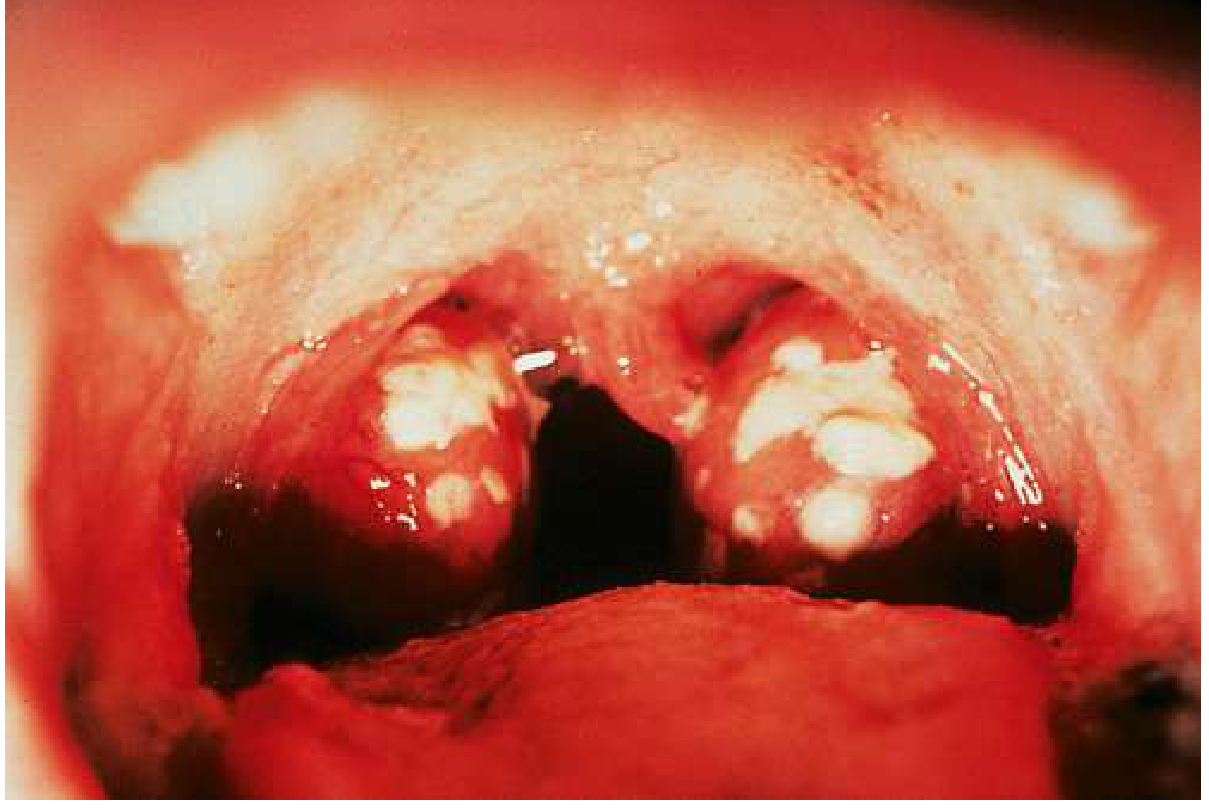
- Presentation: Abrupt onset fever, sore throat, pain on swallowing, submandibular lymphadenopathy. Hypertrophied tonsils, palatal petechiae, confluent tonsillar exudate. Cough and hoarseness are rare with streptococcal infection.
- Other bacterial causes: Diphtheria (thick grey membrane), Gonorrhea (in sexually active patients)
- Other viral causes: EBV (infectious mononucleosis), HSV (stomatitis + pharyngitis), Coxsackie A (herpangina, hand-foot-mouth)
- Diagnosis (Modified Centor Score):
| Criterion | Points |
|---|---|
| Tonsillar exudate | +1 |
| Tender anterior cervical LN | +1 |
| Fever history | +1 |
| Absence of cough | +1 |
| Age 3-14 years | +1 |
| Age 15-44 years | 0 |
| Age >45 years | -1 |
-
Score 0-1: No testing, no antibiotics
-
Score ≥2: Rapid strep test or throat culture
-
Rapid NAAT sensitivity 97.5%, specificity 95% (preferred); antigen test sensitivity only ~85%
-
Gold standard: Throat swab culture
-
Treatment: Penicillin V (10 days) or amoxicillin; prevents rheumatic fever (not glomerulonephritis). Symptomatic: paracetamol 15 mg/kg/dose q4h or ibuprofen 10 mg/kg/dose q6h.
-
Sequelae if untreated: Scarlet fever, rheumatic fever, post-streptococcal GN, bacteremia, peritonsillar abscess
-
Goldman-Cecil Medicine, p. 174-185
3. Acute Rhinosinusitis
- Cause: Viral (majority); bacterial (S. pneumoniae, H. influenzae, M. catarrhalis) in <2% of cases
- Presentation: Nasal congestion, purulent nasal discharge, facial pain/pressure, headache, anosmia, post-nasal drip
- Acute: <4 weeks; Subacute: 4-12 weeks; Chronic: >12 weeks
- Management: Viral - symptomatic (nasal saline irrigation, decongestants). Bacterial - amoxicillin/clavulanate if persistent >10 days, worsening, or severe symptoms. Nasal corticosteroids for recurrent/chronic disease.
- Red flags (refer/escalate): Periorbital swelling, proptosis, diplopia (orbital extension), severe headache, neck stiffness, altered consciousness (intracranial extension)
4. Allergic Rhinitis
- Presentation: Sneezing, bilateral watery rhinorrhoea, nasal pruritus, itchy watery eyes, nasal congestion. Seasonal (pollens) or perennial (dust mites, mold, pet dander).
- Signs: Pale/bluish swollen turbinates, clear discharge, "allergic salute," allergic shiners, Dennie-Morgan lines
- Management: Allergen avoidance, intranasal corticosteroids (first line), oral/intranasal antihistamines, leukotriene receptor antagonists, allergen immunotherapy for refractory cases.
5. Laryngitis (Hoarseness in OPD)
- Acute: Viral infection, voice overuse. Hoarseness, aphonia, mild throat discomfort, dry cough. Self-limiting in 1-3 weeks. Voice rest.
- Chronic: GERD (reflux laryngitis), smoking, vocal cord nodules, polyps, or early malignancy - requires laryngoscopy.
6. Infectious Mononucleosis (EBV)
-
Presentation: Sore throat (exudative pharyngitis), fever, severe fatigue, posterior cervical lymphadenopathy, splenomegaly (50%), hepatomegaly
-
Diagnosis: Heterophile antibody (Monospot) - positive in 60-90% by weeks 2-3; EBV IgM (>90% sensitive, preferred in children <4 years)
-
OPD management: Supportive, rest, analgesics. Avoid contact sports (spleen rupture risk). Do NOT give amoxicillin/ampicillin (causes maculopapular rash in >90% of EBV patients).
-
Caution: Massive tonsillar enlargement can cause URT obstruction - monitor carefully. Glucocorticoids should be used with caution and avoided in children <14 years (may delay lymphoid malignancy diagnosis).
-
Rosen's Emergency Medicine, p. 3685
PART 2 - Emergency Department Presentations
These are conditions with potential for rapid airway compromise or life-threatening progression.
1. Epiglottitis (Supraglottitis) - ⚠️ AIRWAY EMERGENCY
-
Cause: Post-Hib vaccine era: now more common in adults. Causes include S. aureus, S. pyogenes, S. pneumoniae, H. influenzae type b (still in unvaccinated), thermal/chemical injury.
-
Presentation (Classic triad + more):
- 3 Ds: Drooling, Dysphagia, Distress
- High fever, rapidly progressive severe sore throat, muffled/"hot potato" voice, restlessness, lethargy
- Tripod/sniffing position (leaning forward to open airway)
- Stridor (inspiratory), signs of air hunger
- Sore throat disproportionate to pharyngeal findings - key clue
- Adults: more subtle and insidious onset; anterior neck tenderness
- Mortality in adults: 6-7% if mismanaged
-
Lateral neck X-ray: "Thumbprint sign" (enlarged epiglottis) - diagnostic but do NOT delay airway management for imaging
-
Management:
- Do NOT agitate the patient; do NOT examine throat with a tongue depressor in children (may precipitate complete obstruction)
- Secure airway first - OR/ICU setting with ENT/anesthesia standby
- IV antibiotics: ceftriaxone + add vancomycin for MRSA concern
- Heliox, nebulized epinephrine as temporizing measures
-
Textbook of Family Medicine, p. 47-65; Rosen's Emergency Medicine, p. 3533-3537
2. Croup (Laryngotracheobronchitis) - Common Pediatric Emergency
-
Cause: Parainfluenza virus type 1 (most common), also RSV, influenza. Most common URT infection causing airway obstruction in young children (6 months - 3 years).
-
Presentation:
- Barking (seal-like) cough, hoarseness, inspiratory stridor
- Low-grade fever, preceded by viral prodrome (1-2 days)
- Worse at night, worse with agitation
- Mild: barking cough, no resting stridor; Moderate: resting stridor ± retractions; Severe: resting stridor + significant retractions + agitation/altered consciousness
-
X-ray: AP neck - "Steeple sign" (subglottic narrowing)
-
Westley Croup Score used for severity grading
-
Management:
- Mild: single oral dose dexamethasone 0.15-0.6 mg/kg - reduces symptoms, hospitalizations, ED length of stay
- Moderate-severe: dexamethasone + nebulized epinephrine (L-epinephrine 5 mL of 1:1000, or racemic epinephrine)
- Observe for 2-4 hours post-epinephrine before discharge (rebound effect)
- Discharge when free of resting stridor and distress
-
Rosen's Emergency Medicine, p. 3540-3546
3. Bacterial Tracheitis - ⚠️ Critical Emergency
-
Cause: S. aureus (most common, including MRSA), also S. pneumoniae, H. influenzae. Secondary bacterial infection on viral croup.
-
Presentation:
- Croup-like illness that suddenly deteriorates
- High fever, toxic appearance, marked respiratory distress, stridor
- Does NOT respond to croup treatment (nebulized epinephrine)
- Can progress rapidly to complete airway obstruction
-
Imaging: Subglottic membrane or irregularity on lateral neck X-ray
-
Diagnosis and treatment: Bronchoscopy is both diagnostic (pseudomembrane in trachea) and therapeutic
-
Antibiotics: Cephalosporin + MRSA coverage (vancomycin or clindamycin)
-
Usually requires ICU admission and often intubation
-
Rosen's Emergency Medicine, p. 3549-3553
4. Peritonsillar Abscess (PTA) - Emergency/Urgent
-
Definition: Most common deep neck space infection. Collection between the tonsil capsule and the superior pharyngeal constrictor muscle.
-
Age group: Older children, teenagers, young adults
-
Presentation:
- Severe unilateral throat pain, odynophagia, trismus (2/3 of patients)
- Muffled "hot potato" voice, drooling
- Uvula displaced away from the abscess (50%)
- Peritonsillar bulge, asymmetric tonsillar swelling
- Otalgia (referred pain)
- Severe respiratory distress is unusual (differentiates from epiglottitis)
-
Microbiology: Polymicrobial - S. pyogenes, S. aureus (including MRSA), anaerobes
-
Investigation: Posterior pharynx ultrasound (confirms abscess, guides aspiration); CT if deep neck extension suspected (carotid artery lies 25 mm posterolateral to tonsillar pillar)
-
Treatment:
- Needle aspiration or incision and drainage (antibiotics alone insufficient for formed abscess; adequate for phlegmon/cellulitis)
- IV antibiotics: ampicillin-sulbactam or clindamycin
- Tonsillectomy ("quinsy tonsillectomy") for recurrent cases (10-20% recurrence)
-
Rosen's Emergency Medicine, p. 3676-3680
5. Retropharyngeal Abscess (RPA) - ⚠️ Airway Emergency
-
Age group: Primarily children <4 years (retropharyngeal nodes regress with age); occasionally adults post-trauma/instrumentation
-
Presentation:
- High fever, neck pain, dysphagia, refusal to eat, neck stiffness
- Posterior pharyngeal wall bulging (subtle, may be missed)
- Stridor and respiratory distress if airway compressed
- Torticollis, drooling
- Potentially life-threatening: Risk of airway obstruction, mediastinitis, aspiration (abscess rupture), carotid artery erosion (Lemierre's syndrome)
-
Imaging: Lateral neck X-ray (increased prevertebral soft tissue >7mm at C2, >14mm at C6 in children); CT neck with contrast is preferred to define extent
-
Treatment: IV antibiotics + surgical drainage in OR. Do NOT examine pharynx vigorously - may rupture the abscess.
-
Rosen's Emergency Medicine, p. 3690
6. Airway Foreign Body - ⚠️ Emergency
-
Age group: Children 6 months - 4 years (most common), also elderly
-
Presentation:
- Sudden onset choking, coughing in a previously well child (classic history)
- Stridor (upper airway), wheeze (lower airway)
- Unilateral decreased breath sounds
- In adults: history of eating + sudden choking episode
- Esophageal FB: drooling, refusal to eat, no stridor
-
Imaging: Plain films often negative (radiolucent food material); asymmetric hyperinflation or atelectasis on CXR. X-rays must not delay bronchoscopy if strongly suspected.
-
Treatment:
- Complete obstruction: Heimlich maneuver (adults/older children), back blows + chest thrusts (infants)
- Bronchoscopy: diagnostic and therapeutic
- Emergency cricothyroidotomy if cannot intubate/ventilate (needle cricothyroidotomy preferred in infants)
-
Textbook of Family Medicine, p. 69-73; Rosen's Emergency Medicine, p. 3556-3562
7. Epistaxis (Severe) - Emergency
-
Common cause (OPD): Anterior nasal bleeding from Kiesselbach's plexus (Little's area) - nasal dryness, digital trauma, anticoagulants
-
Emergency causes: Posterior epistaxis, hypertension, coagulopathy, sinonasal tumors
-
Risk factors: Nasal sicca, trauma, hypertension, coagulopathy (often therapeutic/iatrogenic), sinonasal neoplasia. Adolescent boys with recurrent epistaxis: consider juvenile nasopharyngeal angiofibroma.
-
Life-threatening if: Posterior bleed, patient on anticoagulants, underlying coagulopathy - can cause respiratory compromise or hypovolemic shock
-
Management:
- Direct pressure (anterior)
- Silver nitrate cautery
- Anterior packing (Vaseline gauze, Merocel) - can cause hypoxemia, especially in cardiopulmonary disease
- Posterior packing or balloon (Foley catheter)
- Nasal packing complication: toxic shock syndrome
- Interventional radiology embolization or ENT ligation for refractory cases
-
Textbook of Family Medicine, p. 75-86
Quick Reference Summary Table
| Presentation | Setting | Key Feature | Immediate Concern |
|---|---|---|---|
| Common cold | OPD | Rhinorrhea, congestion | None |
| Pharyngitis (viral) | OPD | Sore throat, no exudate | Nil |
| Strep pharyngitis | OPD | Exudate, fever, no cough | Rheumatic fever |
| Allergic rhinitis | OPD | Sneezing, watery discharge | Nil |
| Laryngitis | OPD | Hoarseness | Malignancy if chronic |
| Mononucleosis | OPD/ED | Fatigue, exudate, splenomegaly | Airway, splenic rupture |
| Croup | ED | Barking cough, steeple sign | Airway obstruction |
| Epiglottitis | ED - URGENT | Tripod, drooling, disproportionate sore throat | Complete airway loss |
| Bacterial tracheitis | ED - URGENT | Toxic, croup unresponsive to Rx | Complete airway loss |
| Peritonsillar abscess | ED | Trismus, uvula deviation | Deep neck spread |
| Retropharyngeal abscess | ED - URGENT | Neck stiffness, prevertebral swelling | Mediastinitis, airway |
| Airway foreign body | ED - URGENT | Sudden choking, well child | Complete obstruction |
| Severe epistaxis | ED | Posterior bleed, hemodynamic compromise | Hemorrhagic shock |
Sources:
- Rosen's Emergency Medicine: Concepts and Clinical Practice - URT Emergency presentations
- Goldman-Cecil Medicine - Pharyngitis, Streptococcal disease
- Textbook of Family Medicine (9e) - Epiglottitis, Key URT points
- Cummings Otolaryngology Head and Neck Surgery - URI in clinical context
Chronic Granulomatous conditions of Nasal cavity - differential diagnoses and management
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
chronic granulomatous conditions nasal cavity differential diagnosis management ENT
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full structured answer.
Chronic Granulomatous Conditions of the Nasal Cavity
Overview
Chronic granulomatous conditions of the nasal cavity share a common imaging signature: nasal septal perforation and midline sinonasal destruction (septum, turbinates, hard palate). The differential is broad, spanning autoimmune vasculitis, infectious, and neoplastic-mimicking conditions. Tissue biopsy is nearly always required for diagnosis.
The differential must also include non-granulomatous causes of midline destruction: squamous cell carcinoma, cocaine misuse, and syphilis.
- Scott-Brown's Otorhinolaryngology Vol. 1, p. 5392-5404
Classification of Chronic Nasal Granulomata
A. AUTOIMMUNE / VASCULITIC
1. Granulomatosis with Polyangiitis (GPA) - formerly Wegener's Granulomatosis
The most common granulomatous condition to involve the nasal cavity and paranasal sinuses.
Epidemiology:
- Mean age at diagnosis: 40-50 years; equal sex distribution
- Incidence: 10-15 per million per year; predominantly Caucasian (>90%)
- Prevalence up to 5 per 100,000 in Europe
Pathology:
- Classic triad: necrotizing granulomatous inflammation of the upper and lower airways + systemic necrotizing vasculitis of small-to-medium vessels + focal/proliferative glomerulonephritis
- Autoimmune: ANCA (anti-neutrophil cytoplasmic antibody) activates neutrophils causing vascular endothelial damage
- Association with chronic nasal S. aureus carriage (associated with relapses)
Nasal Manifestations (presenting site in up to 95%):
- Chronic nasal obstruction, purulent or bloody nasal discharge, nasal crusting, epistaxis, malodorous discharge
- Mucosal cobblestoning of septum and lateral nasal wall (endoscopic appearance)
- Septal perforation and saddle nose deformity from ischemic cartilage necrosis
- Subglottic stenosis in ~20% (life-threatening)

Endoscopic appearance of GPA - cobblestoning of septum and lateral nasal wall (Cummings Otolaryngology)
Systemic features:
- Upper airway: 90-95% | Lungs: 54-85% (nodules, cavitation, alveolar hemorrhage) | Kidneys: 51-80% (GN) | Eyes: 35-52% (conjunctivitis, episcleritis, proptosis, visual loss)
- Oral: gingival hyperplasia ("strawberry gums"), oropharyngeal ulcers
- Skin: ulcers, nodules | Neuro: meningitis, mononeuritis multiplex, cranial nerve neuropathy
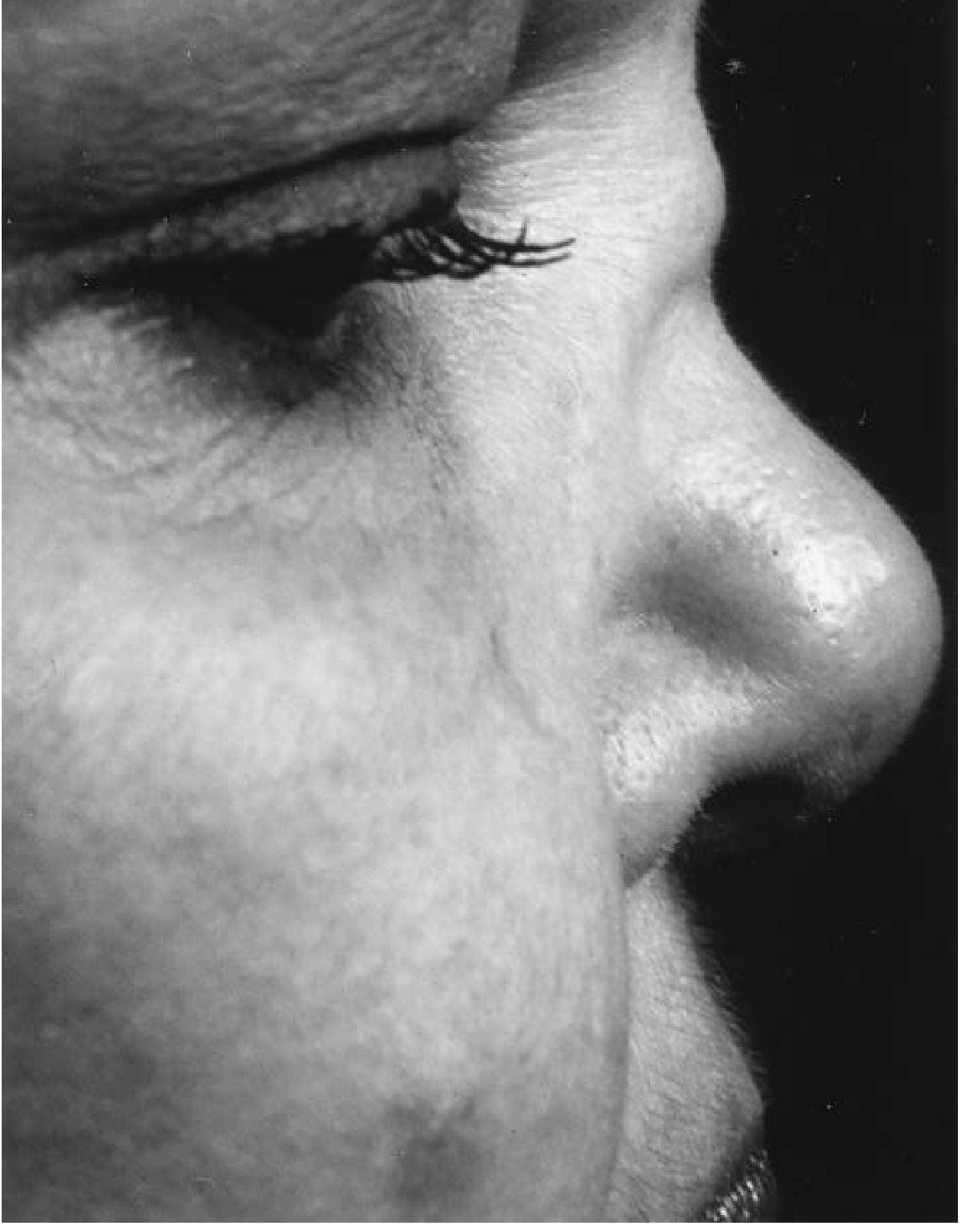
Saddle nose deformity of GPA:
Diagnosis:
- c-ANCA (PR3-ANCA): Sensitivity 91%, specificity 99% in generalized active disease; positive in >90% of active generalized disease; falls to 60% in localized disease; 10-20% may be ANCA-negative (30% in localized disease)
- False-positive c-ANCA: cocaine abuse
- 1990 ACR Classification Criteria (2 of 4):
- Nasal/oral inflammation (painful oral ulcers, purulent/bloody nasal discharge)
- Abnormal CXR (nodules, infiltrates, cavities)
- Abnormal urinary sediment (microscopic hematuria ± red cell casts)
- Granulomatous inflammation on biopsy
- ESR, CRP, serum creatinine, urea, urinalysis, chest X-ray
- Biopsy: Histology shows granulomatous inflammation + vasculitis + necrosis. Paranasal sinus biopsies more diagnostic than nasal specimens. Non-diagnostic in up to 50% of head and neck specimens.
- CT/MRI: Mucosal thickening early; bone destruction (62%) + neo-osteogenesis (78%) later. CT: combination of bone destruction + new bone formation is virtually diagnostic. MRI: 'tramlining' (fat signal from sclerotic sinus wall on T2); orbital involvement in 37%.

Coronal CT: nasal septal destruction, neo-osteogenesis, sinus opacification, and orbital infiltration in GPA (Scott-Brown's)
Treatment:
-
Untreated: fatal - mean survival 5 months
-
Steroids alone: 50% mortality
-
Remission induction: High-dose corticosteroids + cyclophosphamide (2 mg/kg/day, max 200 mg/day) - remission rate 93%
-
Alternative to cyclophosphamide: Methotrexate (effective in limited/less severe GPA); Rituximab (anti-CD20, as effective as cyclophosphamide - proven in RAVE trial)
-
Maintenance: Azathioprine or methotrexate (to reduce cyclophosphamide toxicity)
-
Cyclophosphamide toxicities: alopecia, hemorrhagic cystitis, opportunistic infections; 11x risk of leukemia/lymphoma, 33x risk of bladder cancer
-
Nasal surgery should be avoided - instrumentation exacerbates disease; treat superinfection of sinuses for local symptoms
-
Over half of patients relapse at least once; monitored by c-ANCA titers
-
Scott-Brown's Otorhinolaryngology Vol. 1, p. 7879-8100; Cummings Otolaryngology, p. 1354-1363; Fishman's Pulmonary Diseases, p. 2709-2713
2. Eosinophilic Granulomatosis with Polyangiitis (EGPA) - Churg-Strauss Syndrome
- Nasal involvement: 50-60% (vs 90-95% for GPA)
- Triad: asthma, eosinophilia, necrotizing vasculitis
- p-ANCA (MPO) positive
- Nasal: allergic rhinitis, nasal polyposis
- Systemic: eosinophilic pneumonia, cardiac disease, mononeuritis multiplex
- Treatment: corticosteroids ± cyclophosphamide
B. GRANULOMATOUS DISEASE OF UNKNOWN ETIOLOGY
3. Sarcoidosis
Epidemiology: Multisystem granulomatous disease; nasal involvement in 0.7-6% of all sarcoid cases; 9% of sarcoid patients present with head and neck manifestations.
Nasal Manifestations (Symptoms in nasal sarcoid):
| Symptom | Incidence |
|---|---|
| Nasal stuffiness/obstruction | 88% |
| Crusting | 63% |
| Blood-stained discharge | 37% |
| Purulent discharge | 30% |
| Facial pain | 22% |
| Anosmia | 4% |
- Tiny pale granulomas on hypertrophic erythematous friable mucosa; ulceration, crusting, adhesions
- Anterior nasal septum most often affected - may perforate (especially after surgery)
- Lupus pernio (purplish thickening of overlying nasal skin) = cutaneous marker of chronic systemic sarcoid
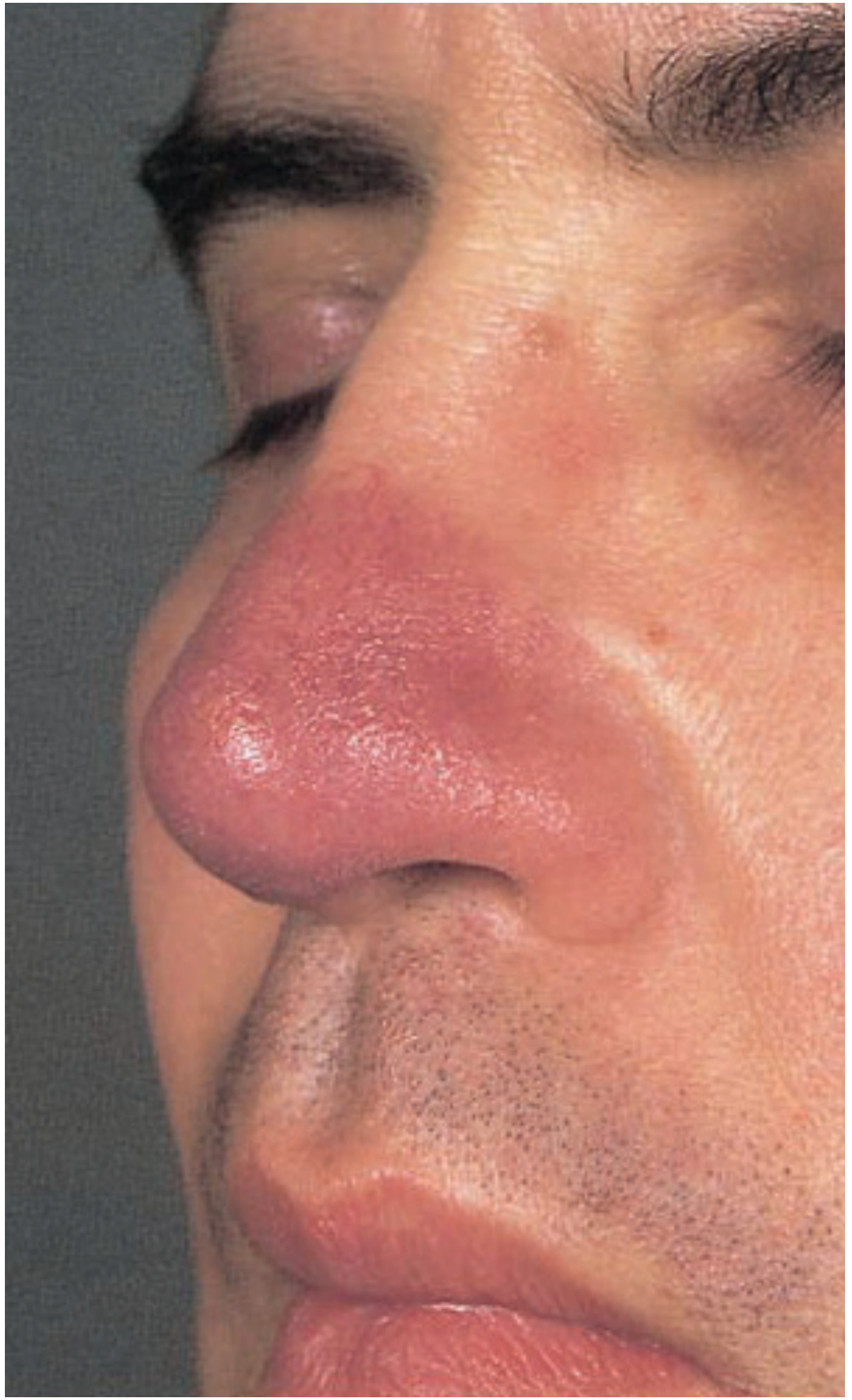
Nasal lupus pernio - characteristic cutaneous sign of sinonasal sarcoidosis (Scott-Brown's)
- Nasal bone: rarefaction, punctate osteolysis (up to 25%); soft tissue mass/expansion of nasal bridge
- Uveoparotid fever (Heerfordt's syndrome): salivary gland enlargement + uveitis + facial palsy (5-10%)
- Laryngeal involvement (1-5%): most commonly supraglottis
Diagnosis:
- No pathognomonic test; diagnosis by exclusion + combination of clinical features, imaging, histology, biochemistry
- Biopsy of abnormal nasal mucosa: >90% positive if mucosa looks abnormal; random biopsy of normal mucosa: 92% negative
- Serum ACE: Elevated in up to 85% during active disease (non-specific; also elevated in TB, leprosy, primary biliary cirrhosis)
- Serum and urinary calcium elevated in ~15%
- CXR/CT chest for staging: Stage I = bilateral hilar LN; II = hilar LN + pulmonary infiltrates; III = infiltrates alone; IV = pulmonary fibrosis
- CT nasal: soft tissue nodules on septum/turbinates (characteristic); sclerosis and osteolysis
- MRI brain: granulomatous basal meningeal involvement
Treatment:
-
Variable course: 2/3 spontaneously remit (usually stage I and II)
-
10-30% follow chronic course despite therapy
-
Topical nasal: Intranasal steroids, glucose/glycerine drops, nasal douching
-
Systemic: Oral corticosteroids for life-threatening disease or critical organ involvement (steroid-sparing: methotrexate, azathioprine)
-
Hydroxychloroquine for cutaneous/sinonasal disease (<50% response; risk of ocular toxicity)
-
TNF-alpha inhibitors (infliximab, etanercept) for refractory disease
-
Intra-lesional steroid injections for focal lesions; lupus pernio may respond dramatically
-
Endoscopic sinus surgery: limited role - only for obstructing lesions or secondary infection in selected cases; avoid septal surgery (increased perforation risk); surgery should be avoided in active disease
-
Scott-Brown's Otorhinolaryngology Vol. 1, p. 7743-7877; Cummings Otolaryngology, p. 1364-1365
C. INFECTIOUS GRANULOMATA
4. Rhinoscleroma (Scleroma)
Organism: Klebsiella rhinoscleromatis (gram-negative rod)
Epidemiology:
- Endemic: Central America, Chile, Central Africa, India, Indonesia, Middle East
- More common in females (13:1 female:male ratio); 2nd-3rd decade
- Crowded, rural areas with poor hygiene and nutrition
- Contracted by direct inhalation; begins at areas of epithelial transition (nasal vestibule)
Affected sites: Nasal cavity primarily; may also involve larynx, nasopharynx, paranasal sinuses, trachea/bronchi, oropharynx (absent uvula)
Symptoms: Nasal obstruction, rhinorrhea, anosmia, epistaxis, nasal deformity; airway narrowing in late stages
Three Stages:
| Stage | Features |
|---|---|
| 1. Catarrhal/Rhinitic | Persistent purulent rhinorrhea, nasal honeycomb-colored crusting |
| 2. Granulomatous/Florid | Painless granulomatous masses in nose + upper respiratory tract, septal destruction, thickened soft palate |
| 3. Sclerotic/Cicatricial | Dense fibrotic scarring, nasal passage narrowing, anosmia, dysphonia, stridor |
Histopathology (pathognomonic features):
- Mikulicz cells: Large macrophages with clear cytoplasm containing bacilli (Klebsiella)
- Russell bodies: Bloated plasma cells with birefringent eosinophilic inclusions
- Pseudoepitheliomatous hyperplasia
Diagnosis: Histology (above) + culture of organism
Treatment:
-
Long-term antibiotics: tetracycline, fluoroquinolones (ciprofloxacin), aminoglycosides, cephalosporins
-
Biopsy + debridement of lesions
-
K.J. Lee's Essential Otolaryngology, p. 8099-8127; Scott-Brown's Vol. 2, p. 4277-4289
5. Rhinosporidiosis
Organism: Rhinosporidium seeberii (aquatic protistan parasite - at animal-fungus boundary; not a true fungus)
Epidemiology:
- Endemic: Africa, Pakistan, Sri Lanka, India
- Transmission: Exposure to spores in contaminated dust, soil, or stagnant water (public bathing)
Affected sites: Nasal cavity and external eye most common; palpebral conjunctivae
Symptoms: Nasal obstruction, epistaxis, rhinorrhea, foreign body sensation
Examination: Friable, polypoid, exophytic mass with submucosal budding and white spores on erythematous surface - classic "strawberry" appearance
Histopathology: Pseudoepitheliomatous hyperplasia + presence of R. seeberii sporangia
Treatment:
-
Surgical excision (primary treatment - infection not highly responsive to medical therapy alone)
-
Long-term dapsone therapy (especially for multisite disease)
-
K.J. Lee's Essential Otolaryngology, p. 8132-8146; Cummings Otolaryngology, p. 1683-1687
6. Nasal Tuberculosis (TB) / Lupus Vulgaris
Nasal TB is rare; most common form is lupus vulgaris (low-grade cutaneous TB)
Nasal features:
- Lupus vulgaris: nodular, ulcerative, scarring lesions in nasal cavities; apple-jelly nodules on diascopy
- Secondary TB pharyngitis: multiple painful shallow ulcers - only with massive cavitating pulmonary TB
- Resurgence parallels HIV epidemic; extrapulmonary TB increased in HIV-infected individuals
Diagnosis:
- Ziehl-Neelsen stain (acid-fast bacilli) / phenol auramine stain (more sensitive)
- Culture (gold standard); PCR; ELISA for antigens
- Association with pulmonary disease on CXR/CT
- Serum ACE may be elevated (non-specific)
Treatment:
-
First-line anti-TB therapy: isoniazid + rifampicin + pyrazinamide (triple therapy) - nasal/pharyngeal TB resolves with pulmonary treatment
-
All cases managed with a TB specialist; monitor for drug resistance (MDR-TB)
-
Scott-Brown's Vol. 2, p. 4457-4507
7. Leprosy (Leprous Rhinitis)
- Mycobacterium leprae; nasal involvement is an early feature of lepromatous leprosy
- Nasal mucosa: congestion, crusting, epistaxis; may lead to collapse of nasal bridge (saddle nose)
- Histology: foamy macrophages (Virchow cells) containing bacilli; non-caseating granulomata in tuberculoid leprosy
- Diagnosis: slit-skin smear, biopsy (Wade-Fite stain for acid-fast bacilli), lepromin test
- Treatment: Multi-drug therapy (MDT) - dapsone + rifampicin ± clofazimine (WHO regimen)
8. Syphilitic Rhinitis (Tertiary Syphilis)
- Treponema pallidum; nasal involvement in tertiary/congenital syphilis
- Gummata (granulomatous lesions) in the nose: perforation of hard palate and nasal septum, saddle nose deformity
- Diagnosis: RPR, VDRL, FTA-ABS, TPHA; biopsy (obliterative endarteritis)
- Treatment: Penicillin G (benzathine penicillin); doxycycline if penicillin-allergic
9. Fungal Granulomata
Invasive fungal rhinosinusitis (immunocompromised patients):
- Organisms: Aspergillus spp., Mucor, Rhizopus (mucormycosis), Histoplasma, Blastomyces, Coccidioides
- Nasal: crusting, epistaxis, facial pain, black necrotic eschar (mucormycosis)
- Diagnosis: nasal endoscopy + biopsy (histopathology + fungal culture); CT/MRI for extent
- Treatment: Amphotericin B (mucormycosis/aspergillus) + urgent surgical debridement; voriconazole (aspergillosis); correct underlying immunosuppression
Non-invasive fungal granuloma (immunocompetent):
- Aspergillus mycetoma (fungus ball) in paranasal sinuses: unilateral opacification with metallic flecks on CT
- Treatment: Functional endoscopic sinus surgery (FESS) + clearance of fungal debris
D. NEOPLASTIC MIMIC (IMPORTANT DDx)
10. NK/T-Cell Lymphoma (Lethal Midline Granuloma - historical term)
-
EBV-associated; previously misclassified as "lethal midline granuloma" or "idiopathic midline destructive disease"
-
Nasal: destructive midline lesion spreading as a thin sheet enveloping turbinates and septum; may extend into nasopharynx or sinuses. Usually unilateral presentation initially. Nodal involvement unusual.
-
CT/MRI: cannot be distinguished from true granulomatous disease without biopsy
-
Diagnosis: Biopsy with immunohistochemistry (CD56+, CD3+, EBV in situ hybridization - EBER positive)
-
Treatment: Radiotherapy ± chemotherapy (CHOP-like regimens)
-
Scott-Brown's Vol. 1, p. 5435-5439
E. COCAINE-INDUCED MIDLINE DESTRUCTIVE LESION (CIMDL)
-
Mimics GPA on imaging and clinically; can give false-positive c-ANCA
-
Typically unilateral initially; extent of mid-face destruction often greater than GPA at presentation (due to delayed presentation)
-
CT: mucosal thickening + destruction of inferior/middle turbinate; septum may be spared initially
-
Diagnosis of exclusion; detailed social/drug history essential
-
Management: cessation of cocaine use; no immunosuppression
-
Scott-Brown's Vol. 1, p. 5425-5428; Fishman's Pulmonary Diseases, p. 2613-2629
Diagnostic Approach - Key Investigations
| Investigation | Purpose |
|---|---|
| Nasal endoscopy + biopsy | Essential - histology, culture |
| c-ANCA (PR3-ANCA) | GPA (91% sensitivity, generalized) |
| p-ANCA (MPO-ANCA) | MPA, EGPA |
| Serum ACE | Sarcoidosis (elevated in 85%; non-specific) |
| ESR, CRP | Inflammation marker |
| FBC, serum creatinine, urinalysis | Renal involvement (GPA) |
| Serum/urine calcium | Sarcoidosis (elevated ~15%) |
| CXR / CT chest | Sarcoid staging; GPA lung nodules/cavities; TB |
| CT sinuses | Bone destruction, neo-osteogenesis pattern |
| MRI sinuses | Granulomatous tissue characterization; tramlining (GPA) |
| ZN stain / AFB culture | TB, leprosy |
| Slit-skin smear | Leprosy |
| RPR/VDRL/FTA-ABS | Syphilis |
| Fungal culture + KOH prep | Fungal granuloma |
| EBV EBER ISH (biopsy) | NK/T-cell lymphoma |
| Drug history | Cocaine (CIMDL) |
Summary Differential Diagnosis Table
| Condition | Key Feature | Biopsy Finding | First-line Treatment |
|---|---|---|---|
| GPA (Wegener's) | c-ANCA+, saddle nose, renal disease | Necrotizing granuloma + vasculitis | Steroids + cyclophosphamide / rituximab |
| Sarcoidosis | Lupus pernio, elevated ACE, hilar LN | Non-caseating granuloma (no necrosis) | Oral corticosteroids; methotrexate |
| Rhinoscleroma | Endemic area, stages, crusting | Mikulicz cells + Russell bodies | Long-term tetracycline/fluoroquinolone |
| Rhinosporidiosis | Strawberry polypoid mass | R. seeberii sporangia | Surgical excision + dapsone |
| Nasal TB / Lupus vulgaris | AFB+, pulmonary TB | Caseating granuloma, AFB | Anti-TB triple therapy |
| Leprosy | Nasal collapse, endemic area | Virchow cells / non-caseating (tuberculoid) | WHO MDT (dapsone + rifampicin ± clofazimine) |
| Syphilis | Gumma, serological+, congenital | Obliterative endarteritis | Benzathine penicillin G |
| Fungal granuloma | Immunocompromised, black eschar | Hyphae on PAS/GMS stain | Amphotericin B + surgical debridement |
| NK/T-cell lymphoma | Unilateral, EBV+, CD56+ | CD56+ T-cell lymphoma | Radiotherapy ± chemotherapy |
| CIMDL (cocaine) | False +c-ANCA, drug history | No vasculitis or necrosis | Stop cocaine; no immunosuppression |
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1 - Sarcoidosis, GPA, granulomatous imaging
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2 - Rhinoscleroma, TB
- K.J. Lee's Essential Otolaryngology - Rhinoscleroma, Rhinosporidiosis
- Cummings Otolaryngology Head & Neck Surgery - GPA, Sarcoidosis (sinonasal)
- Fishman's Pulmonary Diseases and Disorders - GPA systemic features, CIMDL
This is a shared conversation. Sign in to Orris to start your own chat.