Trichilemmal cyst
Reading File
Finding Sources
Finding Sources
Searching PubMed
trichilemmal cyst
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a comprehensive overview of the trichilemmal (pilar) cyst synthesized from Fitzpatrick's Dermatology, Andrews' Diseases of the Skin, and Dermatology (2-Volume Set, 5e):
Trichilemmal Cyst (Pilar Cyst)
Synonyms: Pilar cyst, wen, isthmus-catagen cyst
Origin and Pathogenesis
Trichilemmal cysts arise from the outer root sheath of the hair follicle at the isthmus (the region between the sebaceous gland orifice and the arrector pili muscle insertion). This epithelium undergoes a distinctive pattern of keratinization - cells become swollen and pale as they approach the cyst cavity, then abruptly keratinize without forming a granular cell layer (trichilemmal keratinization). This absence of a granular layer is the histological hallmark of the lesion.
- Fitzpatrick's Dermatology, Vol. 1-2
- Andrews' Diseases of the Skin
Epidemiology
- Prevalence: 5-10% of the population
- Predominantly affects middle-aged to older women (women over 60 especially in Andrews')
- ~90% of lesions occur on the scalp
- Lesions are frequently multiple (most patients have more than one); 10% of patients have >10 lesions
- Hereditary form (autosomal dominant) - linked to the short arm of chromosome 3 (not to β-catenin or MLH1); germline variant in PLCD1 (phospholipase C delta 1α) has been identified
Clinical Features
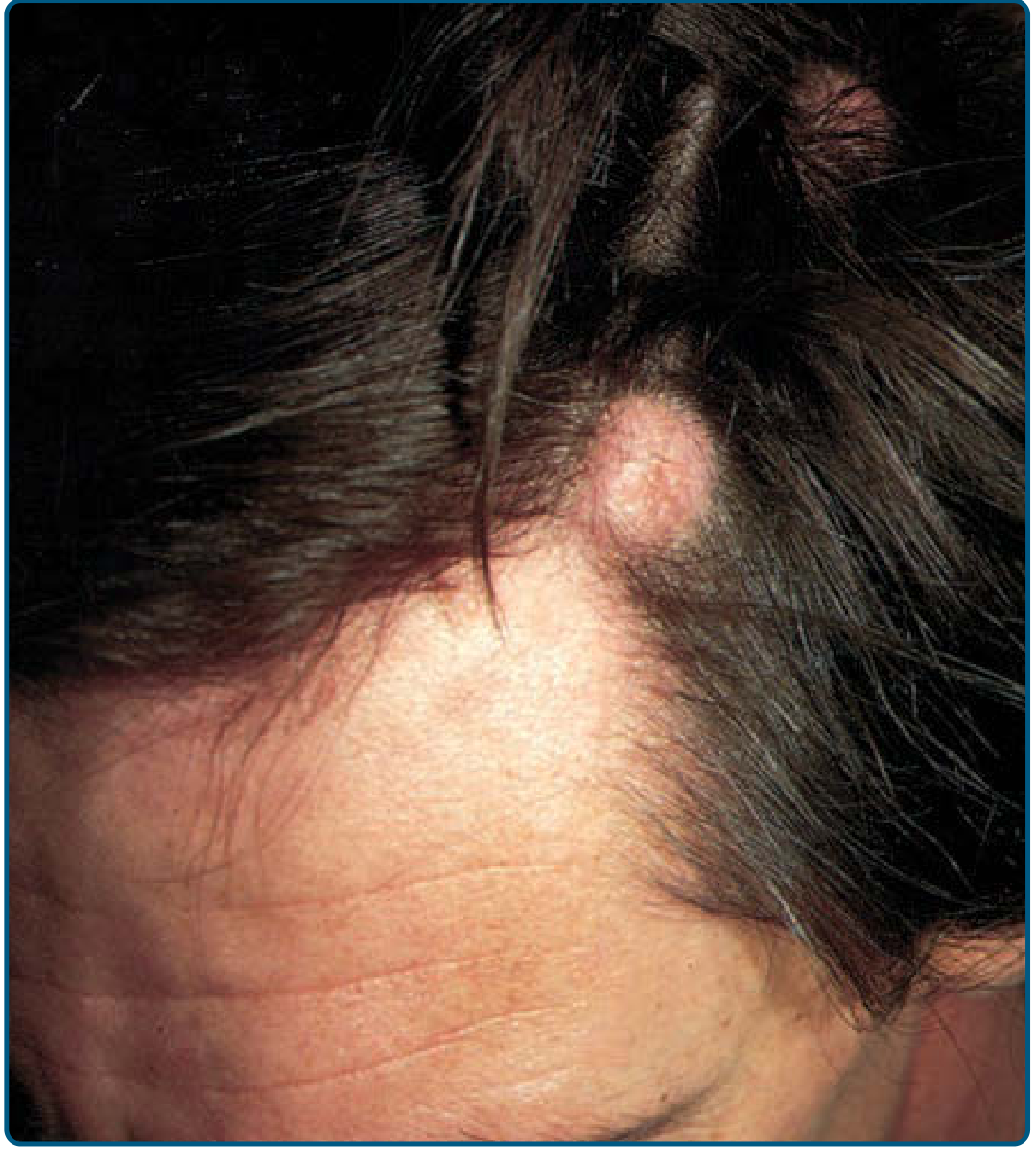
- Mobile, firm, well-circumscribed dermal/subcutaneous nodule
- No overlying punctum (distinguishes it from epidermoid cyst)
- Firmer and more mobile than epidermoid cysts
- Overwhelmingly located on the scalp; rarely on face, trunk, extremities
- Usually asymptomatic, but rupture and secondary infection can occur
- Rapid growth is abnormal - raises suspicion for infection or malignant transformation
Histopathology
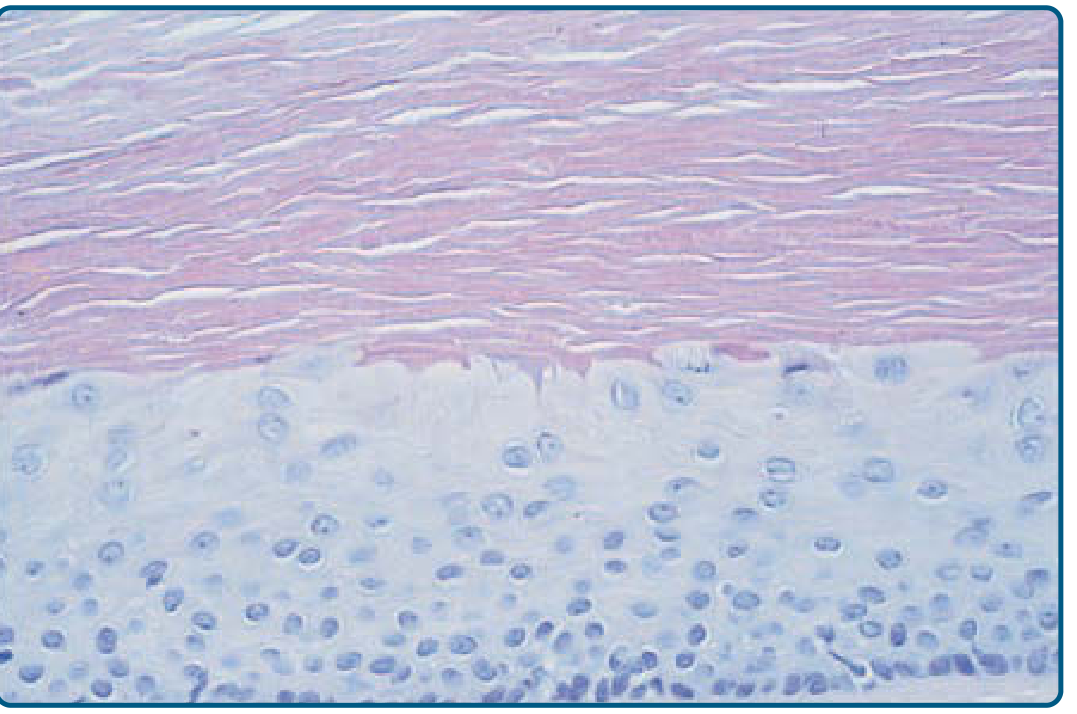
Key histological features:
| Feature | Trichilemmal Cyst | Epidermoid Cyst |
|---|---|---|
| Granular layer | Absent | Present |
| Keratinization | Abrupt (trichilemmal) | Laminated, basket-weave |
| Cyst contents | Homogeneous eosinophilic keratin | Laminated keratinous material |
| Calcification | Common | Rare |
| Punctum | Absent | Usually present |
| Origin | Outer root sheath | Follicular infundibulum |
Cyst contents consist of homogeneous, compact eosinophilic material that frequently calcifies and rarely ossifies. Hybrid cysts with features of both epidermoid and pilar cysts can occur.
- Andrews' Diseases of the Skin; Dermatology 5e
Differential Diagnosis
- Epidermoid (infundibular) cyst - most common mimic; epidermoid cysts have a granular layer and laminated keratin
- Steatocystoma - contains sebaceous material
- Alopecic and aseptic nodules of the scalp (if ruptured)
- Dermoid cyst
- Lymph node (if deep and firm)
Clinically, trichilemmal cysts are 4-5 times less common than epidermoid cysts. At the time of excision, the distinction is often apparent because trichilemmal cysts "deliver" themselves through a small incision more readily without rupture.
Treatment
- Surgical excision is the treatment of choice
- Because the cyst wall is less adherent to surrounding stroma than in epidermoid cysts, it can often be extracted through a small punch biopsy trephine incision
- Pilar cysts are much more easily enucleated - more limited incision is required
Proliferating Trichilemmal Cyst / Proliferating Pilar Tumor

This represents a spectrum ranging from typical pilar cysts with focal proliferation to frankly malignant squamous cell carcinoma-like lesions:
Benign proliferating pilar tumor:
- Large (up to 25 cm), exophytic neoplasm - almost exclusively on the scalp and back of neck
- ~5x more common in women; mean age 65 years
- Gradually enlarges, may ulcerate
- Histology: squamous cell proliferations with trichilemmal differentiation, scroll-like structures; focal atypia, mitoses, and necrosis do not necessarily predict aggressive behavior if an invasive pattern is absent
- Vast majority cured by local excision
Malignant proliferating pilar tumor (malignant trichilemmal cyst):
- Focal areas of frank SCC: increased cellularity, atypia, frequent mitoses, and stromal invasion
- May behave aggressively with metastases
- Red flags for aggressive behavior:
- Non-scalp location
- Recent rapid growth
- Size >5 cm
- Infiltrative growth pattern (clinical and histological)
- Special context: in KID syndrome (keratosis, ichthyosis, deafness), malignant proliferating pilar tumor may develop in young adulthood and can be fatal
Histological distinction between proliferating pilar tumor and SCC relies on identification of squamous eddies, trichilemmal keratinization, or remnant of a pilar cyst. Immunohistochemistry can also assist.
- Andrews' Diseases of the Skin; Fitzpatrick's Dermatology
A 2025 systematic review (PMID 39539041) specifically characterized the clinical and genomic profile of malignant proliferating trichilemmal tumors, confirming its rarity and aggressive potential when frank malignant transformation occurs.
Key Points Summary
- Origin: Outer root sheath, isthmus of hair follicle
- Site: 90% scalp, predominantly women
- Hallmark histology: No granular layer + abrupt trichilemmal keratinization + homogeneous eosinophilic contents ± calcification
- No punctum (unlike epidermoid cysts)
- Genetics: AD inheritance linked to PLCD1 / chromosome 3p
- Treatment: Surgical excision - easy enucleation through small incision
- Malignant potential: Rare but real - watch for rapid growth, large size, ulceration, non-scalp location
This is a shared conversation. Sign in to Orris to start your own chat.