I have my university exam of 1 st year of subject physiology These are the important long answer give me answer of this question "Describe the function of basal ganglia, its connections & abnormalities associated with it." and remeber it's a long question and make it easy to memorized
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything I need to write a comprehensive, exam-ready answer. Here is the full answer:
Basal Ganglia - Functions, Connections & Abnormalities
(Long Answer - 1st Year Physiology Exam)
1. INTRODUCTION
The basal ganglia (also called basal nuclei) are a group of deep-seated nuclei of the telencephalon that play a critical role in the control of voluntary movement, cognitive processes, and emotional behavior.
Memory trick: "CAPS + SN" = Caudate, Amygdala, Putamen, (globus pallidus =) Striatum + Nigra
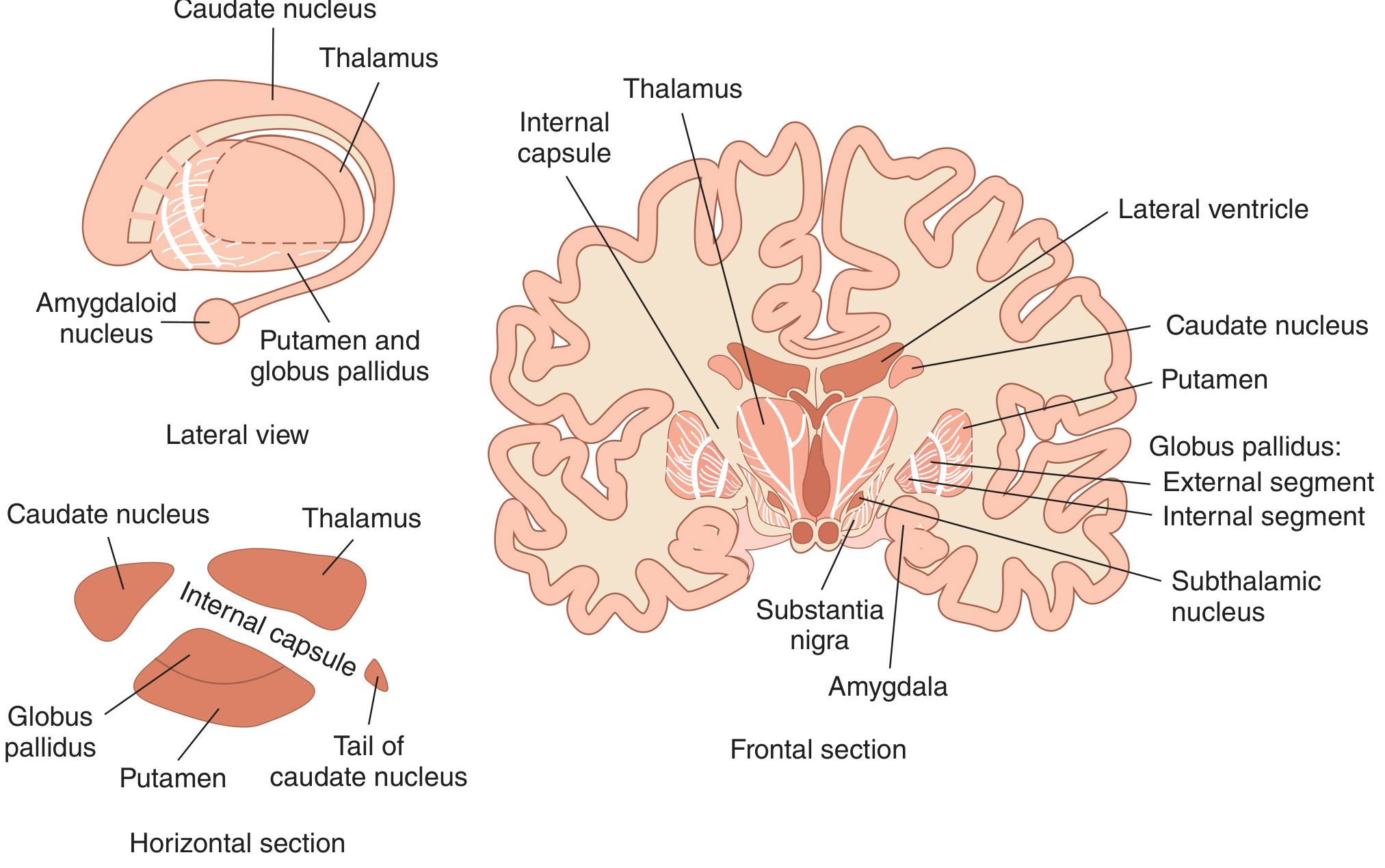
2. COMPONENTS / ANATOMY
The basal ganglia consist of 5 interactive structures on each side:
| Structure | Location | Key subdivision |
|---|---|---|
| Caudate nucleus | Deep in cerebral hemisphere | - |
| Putamen | - | Putamen + Caudate = Striatum |
| Globus pallidus (GP) | Medial to putamen | External (GPe) + Internal (GPi) |
| Subthalamic nucleus | Diencephalon | - |
| Substantia nigra | Midbrain | Pars compacta (SNpc) + Pars reticulata (SNpr) |
- Putamen + Globus pallidus = Lenticular nucleus
- ~95% of striatal neurons = medium spiny neurons (use GABA)
- Remaining = aspiny interneurons (use ACh, somatostatin, GABA)
Anatomical diagram from Ganong's Physiology:
3. CONNECTIONS OF BASAL GANGLIA
INPUTS (Afferents)
Both inputs are excitatory (Glutamate) and terminate in the striatum:
- Corticostriate pathway - from wide areas of cerebral cortex (especially motor cortex)
- Thalamostriatal pathway - from intralaminar nuclei of thalamus
INTERNAL CIRCUITRY - TWO PATHWAYS
There are two opposing internal pathways. Both end with thalamus → motor cortex (excitatory, Glu).
A. DIRECT PATHWAY (Net = EXCITATORY → facilitates movement)
Cortex → Striatum → GPi/SNpr → Thalamus → Motor Cortex
(GABA: inh) (GABA: inh) (Glu: exc)
- Striatum inhibits GPi/SNpr (GABAergic)
- GPi/SNpr would normally inhibit thalamus - this inhibition is now REDUCED
- Thalamus is released from inhibition → excites motor cortex
- Result: Movement is FACILITATED
Memory trick: Direct = D for Dopamine facilitates (D1 receptors), D for Doing movement
B. INDIRECT PATHWAY (Net = INHIBITORY → suppresses movement)
Cortex → Striatum → GPe → Subthalamic nucleus → GPi/SNpr → Thalamus → Motor Cortex
(GABA:inh) (GABA:inh) (Glu: exc) (GABA:inh) (Glu:exc)
- Striatum inhibits GPe (GABA)
- GPe would normally inhibit subthalamic nucleus - this inhibition is now REDUCED
- Subthalamic nucleus excites GPi/SNpr (Glu)
- GPi/SNpr inhibits thalamus (GABA) → motor cortex activity reduced
- Result: Movement is SUPPRESSED
Memory trick: Indirect = Inhibitory = I for Inhibiting movement
C. DOPAMINERGIC PATHWAY (Nigrostriatal pathway)
- SNpc sends dopamine back to striatum
- Dopamine acts on D1 receptors → facilitates direct pathway (excitatory effect)
- Dopamine acts on D2 receptors → inhibits indirect pathway (also facilitates movement)
- Overall: Dopamine promotes movement
Connections diagram from Ganong's Physiology:
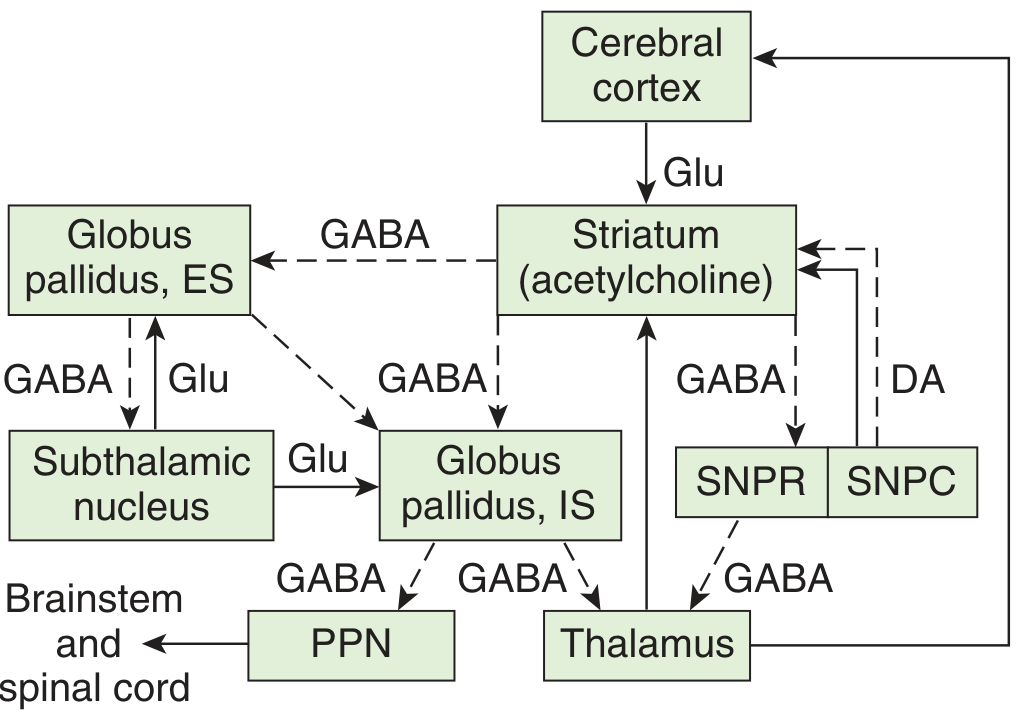
OUTPUTS (Efferents)
Both outputs are inhibitory (GABAergic):
- GPi → Thalamus (via ansa lenticularis & lenticular fasciculus)
- SNpr → Thalamus
- GPi → Brainstem (pedunculopontine nucleus - PPN) → motor neurons in brainstem & spinal cord
SUMMARY TABLE OF NEUROTRANSMITTERS
| Pathway | Neurotransmitter | Effect |
|---|---|---|
| Cortex → Striatum | Glutamate | Excitatory |
| Striatum → GPe / GPi / SNpr | GABA | Inhibitory |
| GPe → Subthalamic nucleus | GABA | Inhibitory |
| Subthalamic nucleus → GPi | Glutamate | Excitatory |
| GPi / SNpr → Thalamus | GABA | Inhibitory |
| Thalamus → Motor cortex | Glutamate | Excitatory |
| SNpc → Striatum (nigrostriatal) | Dopamine | D1: excites direct; D2: inhibits indirect |
4. FUNCTIONS OF BASAL GANGLIA
Memory trick: "PEACE" = Planning, Execution, Affective, Cognitive, Extrapyramidal
- Planning & programming of voluntary movement - neurons discharge even before movement begins
- Execution of smooth, coordinated movement - converts abstract thought into voluntary action
- Maintenance of posture and muscle tone
- Suppression of unwanted movements - via indirect pathway
- Cognitive functions - caudate nucleus connected to prefrontal cortex; involved in object reversal, delayed alternation
- Affective/emotional behavior - via amygdala connections
- Language - lesion of left caudate nucleus → dysarthric aphasia resembling Wernicke's
5. DISEASES / ABNORMALITIES OF BASAL GANGLIA
Three normally balanced biochemical pathways are involved:
- Nigrostriatal dopaminergic system
- Intrastriatal cholinergic system
- GABAergic system (striatum → globus pallidus/SN)
Diseases fall into two broad categories:
A. HYPOKINETIC DISORDERS (decreased movement)
PARKINSON'S DISEASE
- Cause: Degeneration of SNpc → loss of dopamine in striatum
- Effect: Direct pathway under-activated + Indirect pathway over-activated → thalamus excessively inhibited → reduced motor cortex activity
- Features (TRAP):
- Tremor - resting ("pill-rolling") tremor, 4-6 Hz
- Rigidity - cogwheel or lead-pipe rigidity
- Akinesia/Bradykinesia - slowness/poverty of movement
- Postural instability
- Treatment: Levodopa (L-DOPA) - replenishes dopamine
Memory trick: TRAP = Tremor, Rigidity, Akinesia, Postural instability
B. HYPERKINETIC DISORDERS (excessive, abnormal movements)
HUNTINGTON'S DISEASE (Huntington's Chorea)
- Cause: Autosomal dominant, chromosome 4; loss of GABAergic neurons in striatum (especially those projecting via indirect pathway)
- Effect: Indirect pathway is impaired → excessive thalamic excitation → excess movement
- Features:
- Chorea (rapid, involuntary, irregular, dance-like movements)
- Progressive dementia
- Psychiatric disturbances
- Onset: 35-50 years
Memory trick: Huntington's = Hyperkinetic, Hereditary, chromosome 4 (4 letters in "Hunt")
HEMIBALLISMUS
- Cause: Lesion of subthalamic nucleus (e.g., small hemorrhage/infarct)
- Effect: Loss of subthalamic excitation of GPi → GPi under-active → thalamus over-excited → excess movements
- Features: Violent, flinging movements of the contralateral limbs (especially proximal)
- Predominantly affects one side (hemi = one side)
Memory trick: Ballismus = like throwing a ball - violent flinging movement
OTHER HYPERKINETIC CONDITIONS
| Condition | Key Feature | Cause |
|---|---|---|
| Athetosis | Slow, writhing, sinuous movements of distal limbs | Striatal lesions |
| Dystonia | Sustained muscle contractions, abnormal postures | Striatal/GPi lesions |
| Tic disorders | Repetitive, stereotyped movements/vocalizations | Basal ganglia circuit dysfunction |
| Tourette's syndrome | Multiple tics + vocalizations | Striatum involvement |
6. QUICK COMPARISON TABLE (Exam Favorite)
| Feature | Parkinson's Disease | Huntington's Disease | Hemiballismus |
|---|---|---|---|
| Movement | Hypokinetic | Hyperkinetic | Hyperkinetic |
| Site of lesion | SNpc (dopamine loss) | Striatum (GABA loss) | Subthalamic nucleus |
| Pathway affected | Both (dopamine depleted) | Indirect pathway impaired | Indirect pathway impaired |
| Tremor type | Resting tremor | Choreiform movements | Ballistic flinging |
| Inheritance | Sporadic/familial | Autosomal dominant | Usually vascular |
| Treatment | Levodopa | Tetrabenazine (symptomatic) | Haloperidol, surgery |
7. MEMORY SUMMARY DIAGRAM
CORTEX (Glu, excitatory)
↓
STRIATUM
|
|--- DIRECT PATH (D1 receptor, dopamine facilitates)
| ↓ GABA (inhibit GPi)
| GPi inhibited → LESS inhibition of thalamus
| → THALAMUS excited → CORTEX excited → MOVEMENT
|
|--- INDIRECT PATH (D2 receptor, dopamine inhibits)
↓ GABA (inhibit GPe)
GPe inhibited → LESS inhibition of subthalamic nucleus
Subthalamic nucleus (Glu) → excites GPi
GPi MORE active → MORE inhibition of thalamus
→ THALAMUS inhibited → CORTEX inhibited → NO MOVEMENT
SNpc ----[dopamine]---→ STRIATUM (maintains balance)
KEY POINTS TO REMEMBER FOR EXAM
- Basal ganglia = CAPS + SN (Caudate, Amygdala, Putamen, striatum = lenticular nucleus + Nigra)
- Direct pathway = excitatory = facilitates movement (net result)
- Indirect pathway = inhibitory = suppresses movement (net result)
- Dopamine (from SNpc) promotes movement via D1 (direct) and D2 (indirect) receptors
- GABA is the main inhibitory transmitter; Glutamate is excitatory throughout
- Parkinson's = hypokinetic = dopamine LOSS in SNpc → treat with Levodopa
- Huntington's = hyperkinetic = GABA loss in striatum → indirect pathway fails
- Hemiballismus = subthalamic nucleus lesion → violent flinging movements
Sources: Ganong's Review of Medical Physiology, 26th Edition; Costanzo Physiology, 7th Edition
This is a shared conversation. Sign in to Orris to start your own chat.