Internal capsule for ten marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have everything needed for a complete 10-mark answer. Here it is:
Internal Capsule
Definition and General Description
The internal capsule is a compact, V-shaped (or arrowhead-shaped) lamina of white matter located deep within each cerebral hemisphere. It represents the largest projection fiber tract of the brain, containing both afferent and efferent nerve fibers traveling between the cerebral cortex, brainstem, and spinal cord. It continues rostrally with the corona radiata and caudally with the cerebral peduncles.
- Localization in Clinical Neurology, 8e, p. 31
Relations
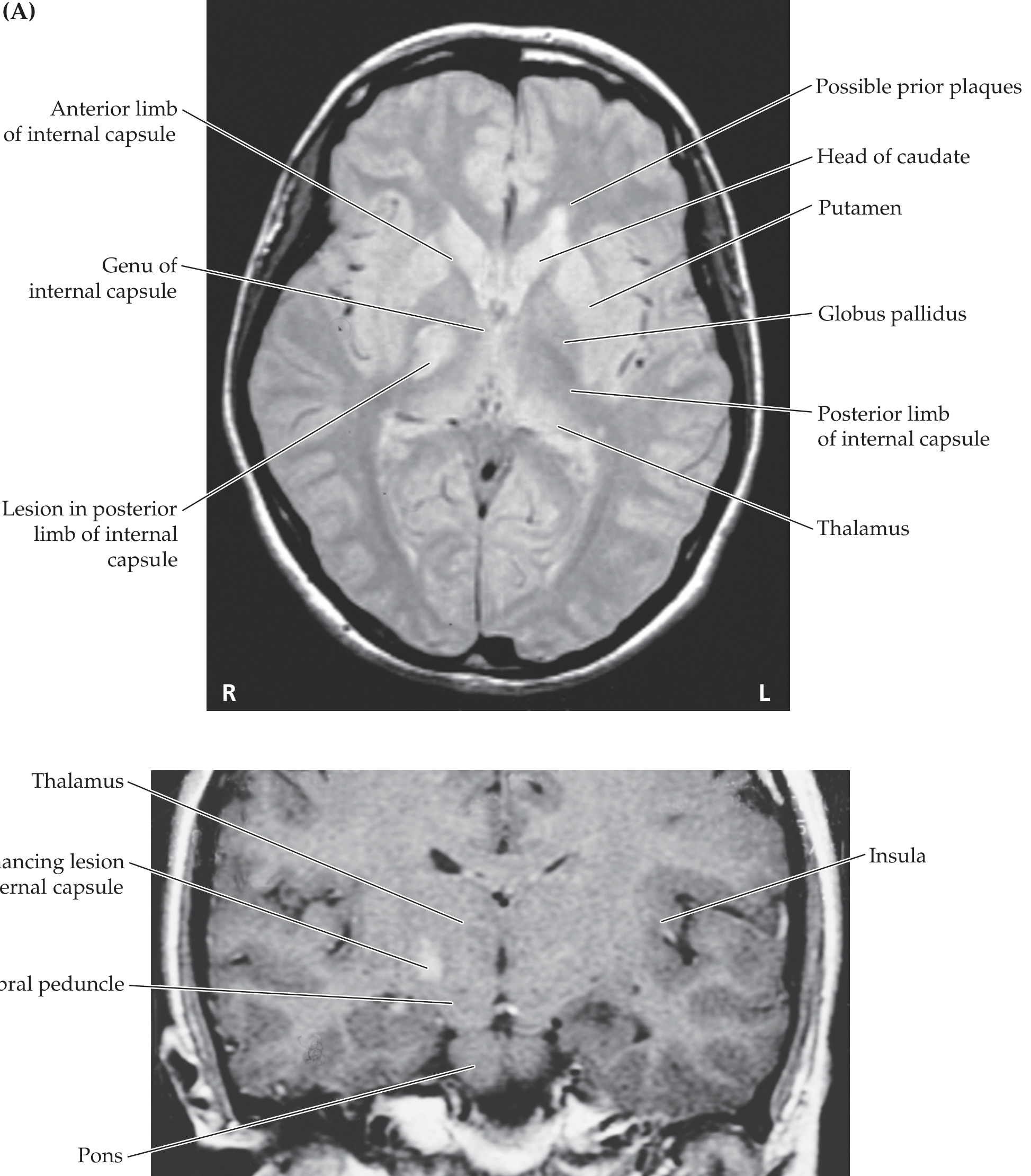
In a horizontal (axial) section, the internal capsule is bounded:
| Side | Structure |
|---|---|
| Medially | Head of caudate nucleus (anteriorly) and thalamus (posteriorly) |
| Laterally | Lentiform nucleus (putamen + globus pallidus) |
Mnemonic: Caudate and Thalamus are always Medial; Lentiform (globus pallidus + putamen) is always Lateral to the internal capsule.
Parts / Segments
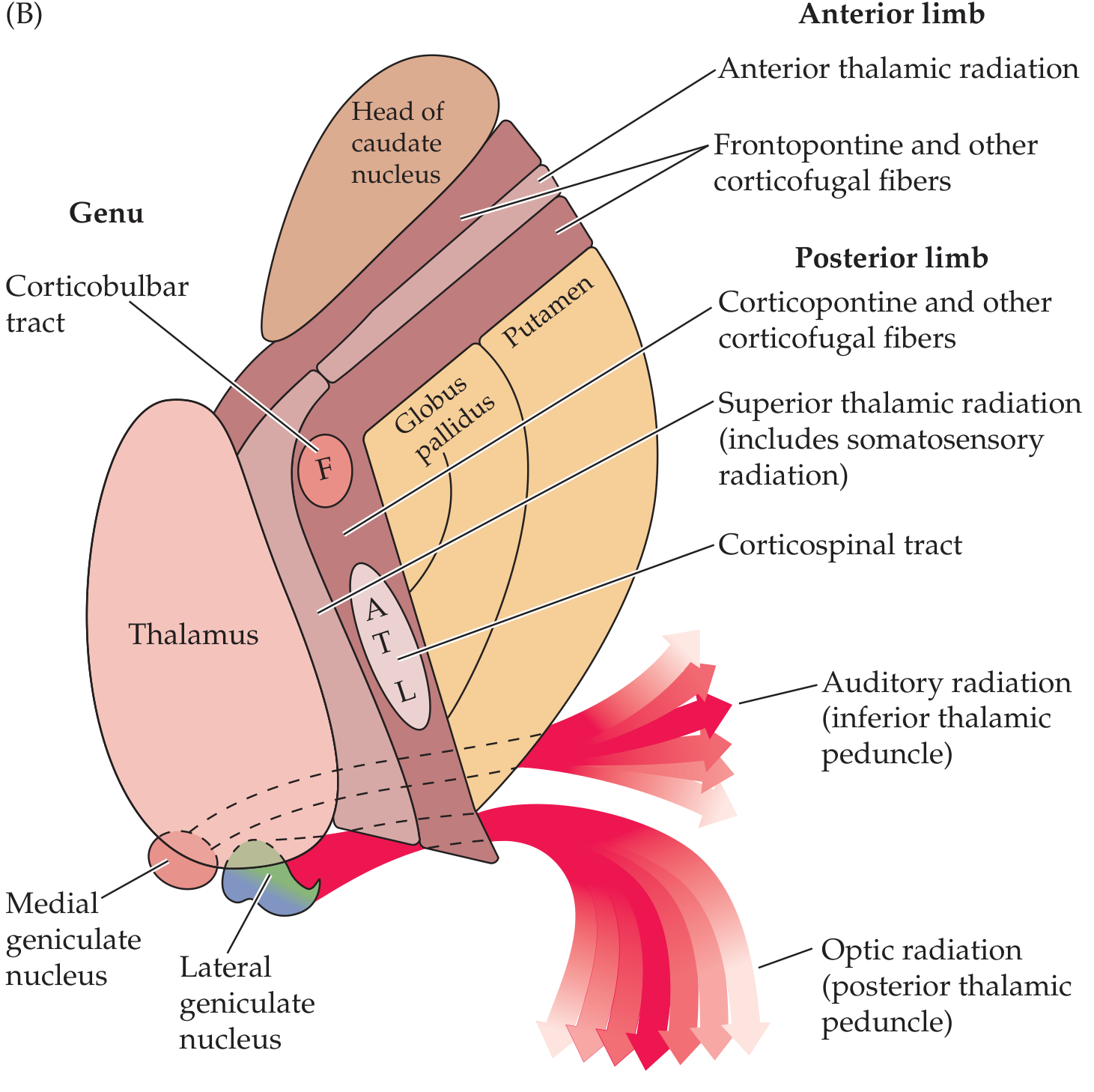
The internal capsule has five segments:
1. Anterior Limb (Lenticulocaudate Segment)
- ~2 cm long
- Separates the lenticular nucleus (lateral) from the head of the caudate nucleus (medial)
Contents:
- Frontopontine fibers (prefrontal cortex → pontine nuclei)
- Anterior thalamic radiation (thalamocortical fibers connecting anterior thalamic nucleus to frontal lobe)
- Caudate-putaminal fibers
- Corticothalamic fibers (reciprocally connecting frontal lobe to thalamus)
2. Genu ("Knee")
- Located at the transition between anterior and posterior limbs, at the level of the foramen of Monro
- Concavity faces the lentiform nucleus
Contents:
- Corticobulbar (corticonuclear) fibers - most prominent content
- Corticoreticular fibers (to brainstem reticular formation, bilaterally)
- Motor corticopontine fibers
Clinical note: Genu lesions produce the "capsular genu syndrome" - facial and lingual hemiparesis with mild limb weakness, because corticobulbar fibers to face and tongue predominate here.
3. Posterior Limb (Lenticulothalamic Segment)
- ~3-4 cm long
- Separates the lenticular nucleus (lateral) from the thalamus (medial)
Contents (anterior to posterior):
- Corticospinal tract (in caudal half) - somatotopically arranged:
- Most anterior: face (F)
- Then: arm (A)
- Then: trunk (T)
- Most posterior: leg (L)
- Superior thalamic radiation (somatosensory fibers from thalamus to parietal cortex)
- Corticorubral fibers
- Corticothalamic fibers
4. Retrolenticular Segment
- Located posterior to the lentiform nucleus
Contents:
- Optic radiation (geniculo-calcarine tract / radiation of Gratiolet) - from lateral geniculate nucleus to primary visual cortex (calcarine cortex)
- Corticotectal fibers
- Corticonigral and corticotegmental fibers
- Parietopontine and occipito-pontine fibers
5. Sublenticular Segment
- Located inferior to the lentiform nucleus
Contents:
- Auditory radiation (inferior thalamic peduncle) - from medial geniculate nucleus to auditory cortex
- Temporopontine fibers
- Some visual radiation fibers
Blood Supply
| Segment | Artery | Source |
|---|---|---|
| Anterior limb | Recurrent artery of Heubner | Anterior cerebral artery (ACA) |
| Genu + middle/inferior posterior limb | Anterior choroidal artery | Internal carotid artery (ICA) |
| Superior anterior and posterior limb | Lenticulostriate arteries | Middle cerebral artery (MCA) |
These are all end-arteries with poor collateral supply, making this region highly vulnerable to ischaemic and haemorrhagic stroke.
- Localization in Clinical Neurology, 8e, p. 31-32
Clinical Significance
Lesions of the Internal Capsule
Because the fibers are extremely compact at this level, even a small lesion (lacunar infarct or haemorrhage) can cause deficits involving the entire contralateral body (face + arm + leg):
| Site of Lesion | Clinical Syndrome |
|---|---|
| Posterior limb | Contralateral pure motor hemiplegia (face, arm, leg) - "Pure Motor Hemiplegia (PMH)" - the most common lacunar syndrome |
| Genu | Capsular genu syndrome - facial/lingual weakness, mild limb weakness |
| Posterior limb (extended) | Mixed sensorimotor hemiplegia (if superior thalamic radiation also involved) |
| Retrolenticular | Contralateral homonymous hemianopia (optic radiation) |
| Sublenticular | Contralateral deafness / auditory radiation involvement |
| Bilateral posterior limb | Paraparesis (rare) |
Internal Capsular Haemorrhage
-
Small hemorrhages in the genu or posterior limb cause PMH or mixed sensorimotor syndrome
-
The small lenticulostriate arteries are especially prone to rupture in hypertension ("Charcot's artery of cerebral haemorrhage")
-
Haemorrhage into the capsule with extension causes decerebrate/decorticate rigidity on the hemiplegic side
-
Neuroanatomy through Clinical Cases 3rd Edition; Localization in Clinical Neurology, 8e; Ganong's Review of Medical Physiology
Summary Table
| Segment | Key Fibers |
|---|---|
| Anterior limb | Frontopontine; anterior thalamic radiation |
| Genu | Corticobulbar (face, tongue) |
| Posterior limb | Corticospinal (F-A-T-L); superior thalamic (somatosensory) radiation |
| Retrolenticular | Optic radiation |
| Sublenticular | Auditory radiation |
The internal capsule is one of the most clinically important white matter structures in the brain. Its dense packing of motor, sensory, and other fibers means that lesions here - typically due to hypertensive lacunar infarcts or haemorrhage - produce dramatic deficits from a small anatomical insult.
This is a shared conversation. Sign in to Orris to start your own chat.