Aetiology, pathology and management of chronic duodenal ulcer
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
"duodenal ulcer" AND "Helicobacter pylori" AND management
Loading Image
I now have all the information needed for a comprehensive answer. Here is the full, well-structured response.
Chronic Duodenal Ulcer: Aetiology, Pathology, and Management
1. AETIOLOGY
A chronic duodenal ulcer is an acute or chronic localized wound of the duodenal mucosa caused by acid/peptic injury, in which superficial ulcers involve the submucosa and deeper ulcers penetrate the muscularis propria or serosa. The fundamental principle is that in the absence of acid, peptic ulcers do not occur - Bailey & Love's Short Practice of Surgery, 28th Ed.
A. Helicobacter pylori (Primary Cause)
H. pylori infection is found in up to 90% of duodenal ulcer patients - Current Surgical Therapy, 14th Ed. and is the dominant aetiological factor. Only 5-10% of those infected actually develop ulcers, indicating that host factors and strain variation also play a role (Robbins & Kumar Basic Pathology).
H. pylori causes ulceration by:
- Colonising the gastric antrum and inducing antral-predominant gastritis with preferential G-cell stimulation and gastrin hypersecretion
- Producing urease, which generates ammonia - directly damaging the mucosa and impairing the bicarbonate mucosal defence layer
- Stimulating neutrophilic and lymphocytic infiltration that perpetuates mucosal injury
- Causing hyperacidity by driving parietal cell hyperplasia and excessive secretory responses
- Reducing somatostatin (D-cell) output, removing normal inhibitory control of acid secretion
B. NSAIDs and Aspirin
The second most important aetiological factor. NSAIDs inhibit cyclooxygenase (COX-1 and COX-2), reducing prostaglandin synthesis. Prostaglandins normally stimulate mucus and bicarbonate secretion and maintain mucosal blood flow. Their depletion unmasks the duodenal mucosa to acid injury. In ageing populations with high low-dose aspirin use, NSAIDs are becoming increasingly important as H. pylori rates fall (Robbins).
C. Acid Hypersecretion
- Patients with duodenal and prepyloric ulcers have higher gastric acid levels on average than normal subjects, though overlap is considerable - Bailey & Love
- Zollinger-Ellison syndrome (gastrinoma): causes multiple peptic ulcerations in stomach, duodenum, and even jejunum due to constitutive gastrin production leading to massive acid secretion - a pure acid-driven cause where H. pylori is not the factor
- Parietal cell hyperplasia and excessive secretory responses
D. Other Predisposing and Causative Factors
| Factor | Mechanism |
|---|---|
| Cigarette smoking | Reduces mucosal blood flow and healing; predisposes to ulceration and increases relapse rate |
| Corticosteroids (high dose) | Suppress prostaglandin synthesis, impair healing |
| Chronic renal failure | Hypercalcaemia stimulates gastrin production |
| Hyperparathyroidism | Hypercalcaemia → ↑ gastrin → ↑ acid |
| Alcohol-related cirrhosis | Increased ulcer frequency |
| Chronic obstructive pulmonary disease | Associated with higher ulcer rates |
| Cocaine | Direct mucosal damage |
| Crohn's disease | Granulomatous duodenal involvement |
| Radiation | Direct mucosal injury |
| Stress ulcers | Acute physiological stress (burns, head injury, critical illness) |
| Gastroduodenal dysmotility | Impaired clearance of duodenal acid load |
Sources: Current Surgical Therapy 14e; Robbins & Kumar Basic Pathology; Bailey & Love 28th Ed.
2. PATHOLOGY
A. Macroscopic (Gross) Pathology
Site: Most ulcers occur in the first part of the duodenum (the duodenal cap/bulb). - Bailey & Love
Structure of the ulcer:
- A chronic ulcer penetrates through the mucosa into the muscle coat (muscularis propria), unlike superficial erosions
- Deep ulcers may involve the serosa and can penetrate posteriorly into adjacent structures
Special configurations:
- "Kissing ulcers": Both a posterior and an anterior duodenal ulcer present simultaneously
- Anterior ulcers tend to perforate (freely into the peritoneal cavity)
- Posterior ulcers tend to bleed, sometimes by eroding into the gastroduodenal artery
- Occasionally the entire duodenal cap may be ulcerated and devoid of mucosa - Bailey & Love
Consequences of chronicity:
- Healing is accompanied by fibrosis and scarring
- Repeated cycles of ulceration and scarring cause pyloric/duodenal stenosis (gastric outlet obstruction)
- After healing, a residual scar can be observed in the mucosa
Endoscopic image of duodenal ulcer:
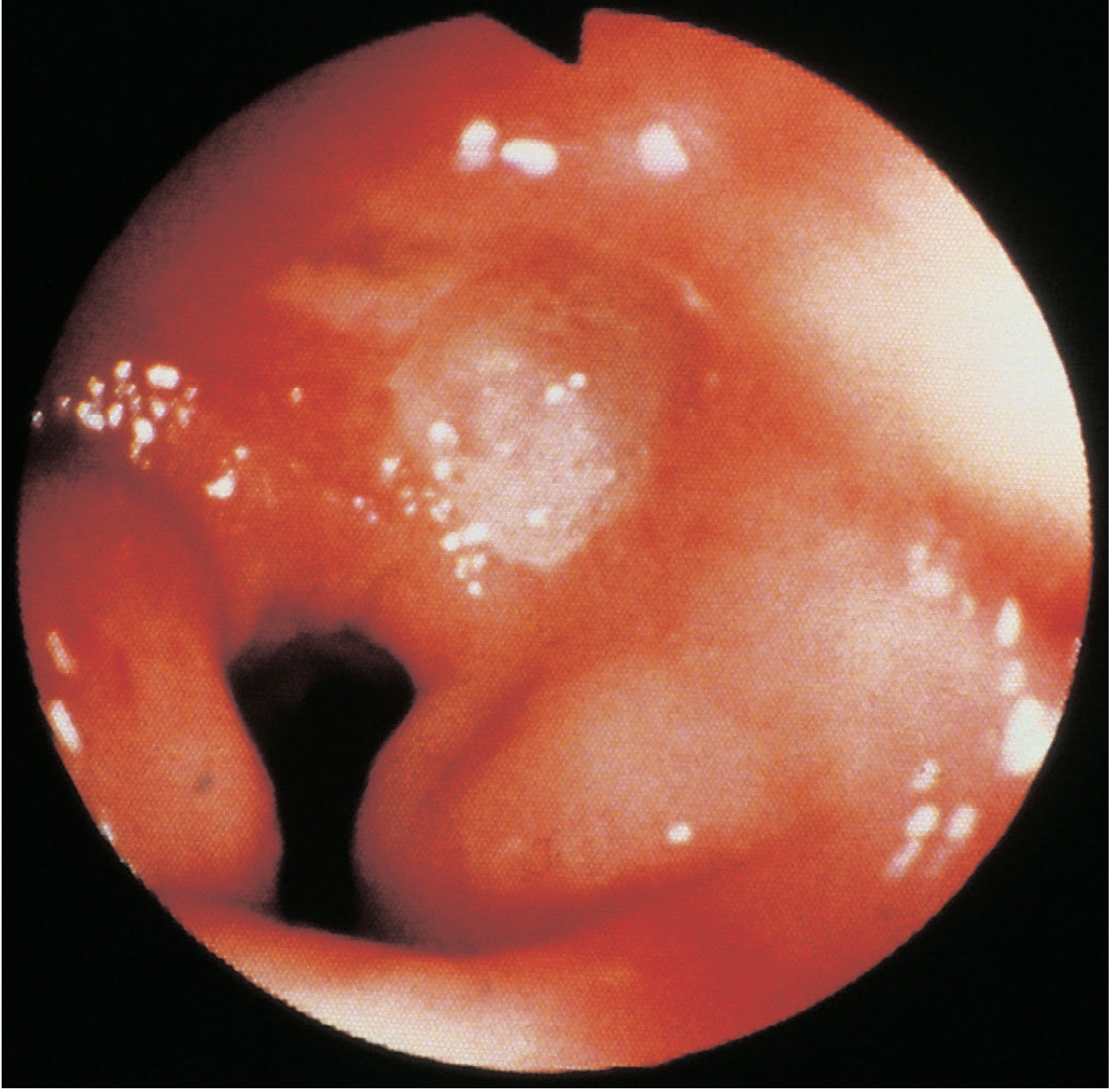
B. Microscopic (Histological) Pathology
The base of a chronic ulcer (from the lumen outward) shows four classical zones:
- Fibrinopurulent exudate - surface layer
- Necrotic tissue - zone of necrosis
- Granulation tissue - vascular proliferation and fibroblasts
- Fibrous scar tissue (endarteritis obliterans) - deepest layer
From Bailey & Love: "Microscopically, the base of the ulcer is covered with granulation tissue and there may be evidence of endarteritis obliterans."
In the healing ulcer, epithelial downgrowth from the edges can be misinterpreted as invasion - an important histological pitfall.
Key distinction from gastric ulcers: Chronic duodenal ulcers are essentially never malignant - this is in stark contrast to gastric ulcers, where malignancy is an important concern requiring mandatory biopsy. Bailey & Love state that even in giant duodenal ulcers, "under normal circumstances surgeons can be confident that they are dealing with benign disease, even though from external palpation it may not appear so."
3. CLINICAL FEATURES
- Epigastric pain: gnawing or burning, often well-localised
- Relieved by food (and antacids) - a characteristic but not pathognomonic feature
- Periodicity: symptoms disappear for weeks to months, then recur (related to spontaneous healing and re-ulceration)
- Radiation to the back: suggests posterior penetration into the pancreas
- Constant pain: suggests deeper penetration
- Nausea and vomiting: present; profuse vomiting with weight loss suggests gastric outlet obstruction
- Anemia may result from chronic blood loss - Sabiston Textbook of Surgery; Bailey & Love
Indications for hospitalisation (in order of frequency):
- Upper GI bleeding
- Perforation
- Gastric outlet obstruction
- Intractability - Current Surgical Therapy 14e
4. DIAGNOSIS
- Esophagogastroduodenoscopy (EGD): method of choice - direct visualisation of ulcer; biopsy of duodenal ulcer is unnecessary (no malignancy risk), but gastric biopsies should be taken to test for H. pylori
- Upper GI barium meal: demonstrates ulcer crater (round/ovoid barium niche); used when endoscopy is unavailable
- H. pylori testing (mandatory in all patients):
- Non-invasive: urea breath test (preferred), faecal antigen test
- Invasive (via endoscopy): rapid urease test, histology, culture, RT-PCR
- Serology - should NOT be used to confirm eradication
- Serum gastrin if ulcer is refractory, recurrent, or requires surgery (to exclude Zollinger-Ellison syndrome)
- Bloods: FBC, LFTs, creatinine, amylase, calcium - Sabiston
5. MANAGEMENT
A. Medical Management
1. Acid suppression:
- Proton pump inhibitors (PPIs) are the mainstay - can render a patient virtually achlorhydric; nearly all benign ulcers heal within 2 weeks; symptom relief within days
- H2-receptor antagonists (e.g. ranitidine): historically useful but largely superseded by PPIs; a minority of patients were refractory
- The major problem with all antisecretory agents: relapse is almost universal following cessation unless the underlying cause (especially H. pylori) is treated - Bailey & Love
2. H. pylori eradication (most important treatment):
Complete eradication cures the disease if H. pylori is the principal aetiological factor. It is more economical and safer than surgery. With appropriate 10-14 day multi-drug regimens (accounting for local antibiotic resistance), eradication is confirmed in approximately 85% of patients - Current Surgical Therapy.
Common eradication regimens (all 10-14 days):
| Regimen | Drugs |
|---|---|
| Clarithromycin triple therapy | PPI + clarithromycin + amoxicillin (or metronidazole) |
| Bismuth quadruple therapy | PPI + bismuth + tetracycline + nitroimidazole |
| Sequential therapy | PPI + amoxicillin × 5-7 days, then PPI + clarithromycin + nitroimidazole × 5-7 days |
| Hybrid therapy | PPI + amoxicillin × 7 days, then add clarithromycin + nitroimidazole |
| Levofloxacin triple therapy | PPI + levofloxacin + amoxicillin |
| Concomitant therapy | PPI + amoxicillin + clarithromycin + nitroimidazole simultaneously |
Test for eradication with urea breath test or faecal antigen test (NOT serology) at least 4 weeks after completion.
3. Elimination of precipitating factors:
- Stop NSAIDs and aspirin if possible
- Smoking cessation
- If NSAIDs/aspirin unavoidable: co-prescribe a PPI indefinitely
4. Long-term PPI:
- Not routinely indicated unless the patient has required hospitalisation for a complication, requires long-term NSAIDs/aspirin/anticoagulants, or compliance with eradication/avoidance of risk factors cannot be assured - Current Surgical Therapy
B. Surgical Management
Surgery for duodenal ulcer is now reserved almost exclusively for complications (perforation, bleeding, obstruction) and very rarely for intractability. The operative 90-day mortality for emergency peptic ulcer surgery is approximately 30% - Current Surgical Therapy.
Indications for surgery:
- Perforation - the most common current indication
- Haemorrhage - refractory to endoscopic therapy
- Obstruction - pyloric/duodenal stenosis
- Intractability - medical failure (now very rare)
Surgical Options and Comparative Outcomes
| Operation | Operative Mortality | Significant Side Effects | Recurrent Ulcer |
|---|---|---|---|
| Gastrectomy | 1-2% | 20-40% | 1-4% |
| Truncal vagotomy + drainage | <1% | 10-20% | 2-7% |
| Selective vagotomy + drainage | <1% | 10-20% | 5-10% |
| Highly selective vagotomy (HSV) | <0.2% | <5% | 2-10% |
| Truncal vagotomy + antrectomy | 1% | 10-20% | 1% |
| Gastroenterostomy alone | <1% | 10-20% | 50% |
Table adapted from Bailey & Love 28th Ed., p. 1183
Specific Surgical Procedures:
1. Highly Selective Vagotomy (HSV) / Proximal Gastric Vagotomy:
- Only the parietal cell mass of the stomach is denervated; the nerves of Latarjet supplying the antrum and pylorus are preserved
- Lowest mortality (<0.2%) and fewest side effects (<5%)
- Elective surgery only; recurrence 2-10%
- No drainage procedure needed as antropyloroduodenal innervation is intact
2. Truncal Vagotomy + Drainage (pyloroplasty or gastrojejunostomy):
- Vagal nerves are cut at the lower oesophagus - reduces maximal acid output by ~50%
- Denervation of the antrum/pylorus causes gastric stasis; hence a drainage procedure (Heineke-Mikulicz pyloroplasty) is mandatory
- Mortality <1%; side effects 10-20% (diarrhoea, dumping)
3. Vagotomy + Antrectomy (Billroth I/II):
- Removes the gastrin-producing antrum combined with acid reduction by vagotomy
- Lowest recurrence (1%) but higher morbidity; Billroth II (Pólya) occasionally needed in emergency complex ulcer disease
4. For Perforation (most common emergency):
- Graham patch (omental patch repair) - the operation of choice in the acute setting; covers the perforation with a flap of omentum
- Laparoscopic repair is now established and preferred in stable patients
- Definitive ulcer surgery at the same sitting is rarely performed today - condition of the patient and peritoneal contamination determine feasibility
5. For Bleeding:
- Endoscopic haemostasis first (injection therapy, thermal coagulation, clips)
- Interventional radiology (angioembolisation) for refractory cases
- Surgical oversewing of the bleeding vessel in the ulcer base (typically the gastroduodenal artery in posterior ulcers) if endoscopic/radiological control fails
- High-dose IV PPIs in the postoperative period to reduce rebleeding risk
6. For Obstruction (Gastric Outlet Obstruction):
- Balloon dilation endoscopically
- Truncal vagotomy + gastrojejunostomy (bypass) if fibrotic obstruction is not amenable to dilation
- Pyloroplasty if the pylorus can be reconstructed
C. Post-operative Principles
To minimise recurrence after any duodenal ulcer surgery, all three of the following must be met - Current Surgical Therapy:
- Eradication of H. pylori infection
- Diligent and permanent avoidance of NSAIDs and aspirin
- Long-lasting abstinence from smoking
If compliance cannot be assured, long-term PPI (e.g. omeprazole 20 mg before breakfast) is appropriate.
Summary
| Aspect | Key Points |
|---|---|
| Primary causes | H. pylori (90% of DU), NSAIDs, acid hypersecretion |
| Site | First part of the duodenum |
| Gross pathology | Mucosal defect to muscularis propria; fibrosis; kissing ulcers; anterior = perforate, posterior = bleed |
| Microscopy | Granulation tissue base, endarteritis obliterans, NO malignancy |
| Medical treatment | PPI + H. pylori eradication (10-14 day triple/quadruple therapy) |
| Surgical indication | Mostly emergency (perforation, bleeding, obstruction) |
| Best elective operation | Highly selective vagotomy (lowest morbidity) |
| Best emergency operation | Graham patch repair ± laparoscopic approach |
Sources: Bailey & Love's Short Practice of Surgery 28th Ed.; Current Surgical Therapy 14e; Sabiston Textbook of Surgery; Robbins & Kumar Basic Pathology; Sleisenger and Fordtran's GI and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.