Rheumatoid arthritis etiopathogenesis in orthopaedics with flow chart and images
Reading File
Finding Sources
Searching the Web
rheumatoid arthritis etiopathogenesis orthopaedics mechanism pathogenesis
Searching PubMed
"rheumatoid arthritis"[MeSH Terms] AND "pathogenesis"[MeSH Terms]
Finding Sources
Loading Image
Loading Image
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive information to provide a detailed, well-illustrated answer. Let me compile the complete response.
Rheumatoid Arthritis: Etiopathogenesis in Orthopaedics
Definition
Rheumatoid arthritis (RA) is a chronic, systemic, inflammatory autoimmune disease primarily affecting synovial joints in a bilateral, symmetric pattern. It affects 1-2% of the world population with a female-to-male ratio of 2.5:1, peak onset in the 3rd-4th decade. The exact cause remains unknown, but significant advances have been made in understanding its immunopathogenesis.
- Campbell's Operative Orthopaedics 15th Ed 2026
- Miller's Review of Orthopaedics 9th Ed
Etiology (Risk Factors)
| Category | Factors |
|---|---|
| Genetic | HLA-DRB1 (shared epitope), HLA-DR4, HLA-DR1, PTPN22, STAT4, PADI4 gene polymorphisms |
| Environmental | Cigarette smoking (strongest modifiable risk factor), periodontal disease (Porphyromonas gingivalis), gut microbiome dysbiosis, viral infections (EBV, Parvovirus B19) |
| Hormonal | Female sex hormones - oestrogen promotes disease; testosterone protective; RA improves in pregnancy (high progesterone) |
| Immune dysregulation | Molecular mimicry, loss of self-tolerance, anti-citrullinated protein antibodies (ACPA/anti-CCP) |
Etiopathogenesis Flow Chart
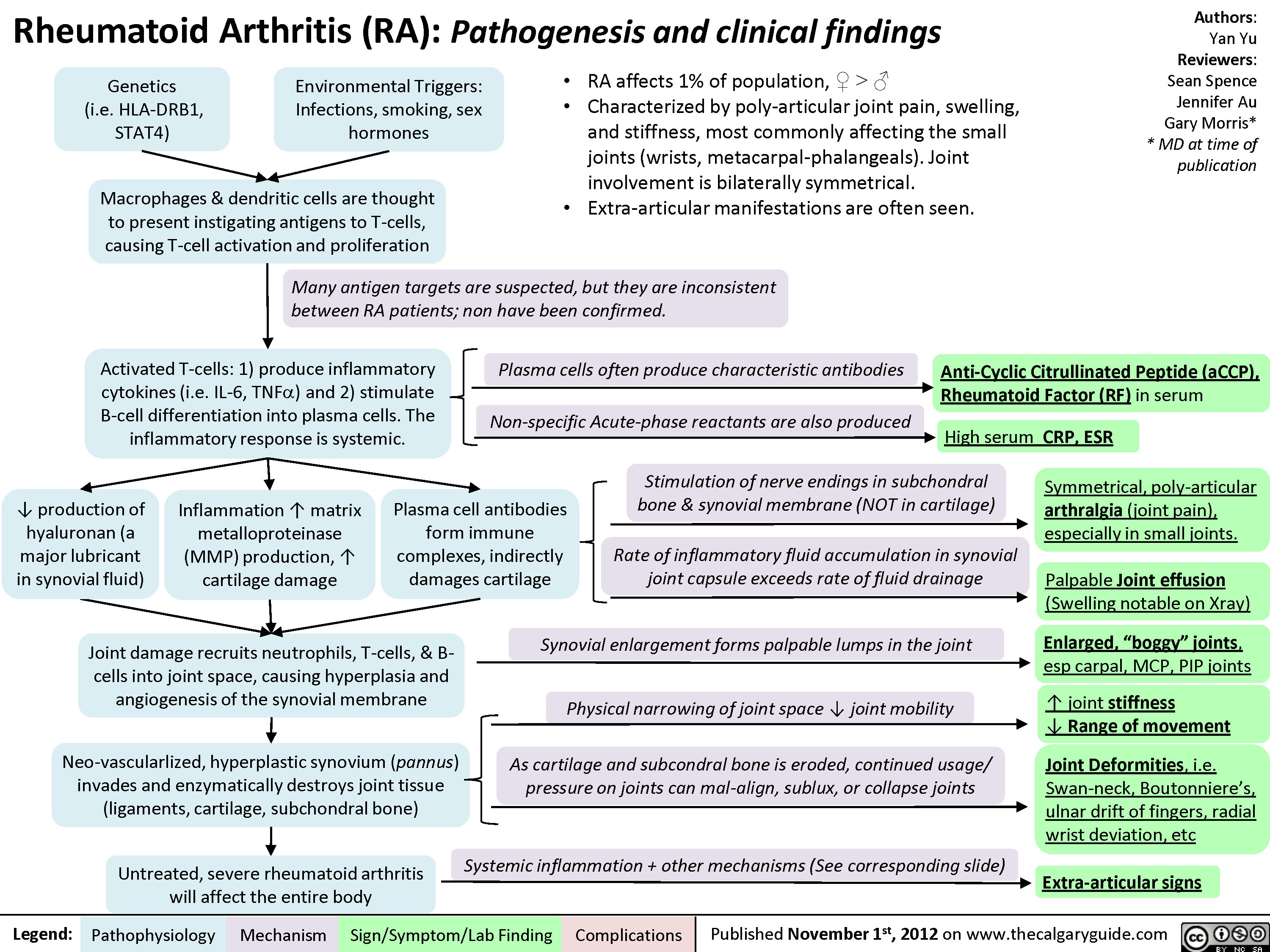
Comprehensive flow chart of RA pathogenesis from genetic/environmental triggers to clinical deformities. (The Calgary Guide to Understanding Disease)
Step-by-Step Pathogenetic Mechanism
PHASE 1: Triggering of Autoimmunity (Pre-clinical RA)
Environmental trigger (smoking, infection, periodontitis)
+
Genetic susceptibility (HLA-DRB1, PTPN22)
↓
Peptidylarginine deiminase (PAD) enzymes activated
↓
Citrullination of self-proteins:
(fibrin, vimentin, fibronectin, collagen type I/II, α-enolase)
↓
Citrullinated proteins recognized as "non-self"
↓
Production of Anti-Citrullinated Protein Antibodies (ACPA/anti-CCP)
+ Rheumatoid Factor (RF = IgM/IgG anti-Fc of IgG)
This phase can exist for years before clinical symptoms appear (pre-RA phase).
PHASE 2: Antigen Presentation and Lymphocyte Activation
Macrophages + Dendritic Cells (DCs) present citrullinated antigens
↓
via MHC Class II (HLA-DR) → CD4+ T-helper cells activated
↓
T-cells differentiate:
• Th1 cells → produce IFN-γ, TNF-α
• Th17 cells → produce IL-17 (critical for neutrophil recruitment)
↓
T-cells stimulate B-cells → Plasma cells
↓
Plasma cells produce RF and ACPA/anti-CCP
(detectable in serum before synovitis begins)
PHASE 3: Synovial Inflammation (Synovitis)
Immune complexes (RF + IgG; ACPA + citrullinated proteins)
↓
Deposit in synovial membrane and joint space
↓
Activate complement cascade (C3a, C5a)
+ Fc receptor activation on macrophages
↓
Release of proinflammatory cytokines:
• TNF-α → master cytokine (drives all downstream inflammation)
• IL-1β → cartilage destruction, fever
• IL-6 → systemic manifestations, acute-phase reactants (CRP, ESR ↑)
• IL-15 → recruits and activates more T-cells
• IL-17 → neutrophil recruitment
• GM-CSF → myeloid cell activation
↓
SYNOVIAL LINING CELL HYPERPLASIA
(lining normally 1-2 cell layers → expands to 6-10 layers)
↓
Fibroblast-like synoviocytes (FLS) become activated
+ Macrophage-like synoviocytes proliferate
PHASE 4: Pannus Formation (The Hallmark of RA)
Activated synovial cells (FLS + macrophages)
↓
Undergo neo-vascularization (angiogenesis - VEGF driven)
↓
Form "PANNUS" = hyperplastic, invasive synovial tissue
(granulation-like tissue overlying cartilage)
↓
Pannus invades articular cartilage and subchondral bone
↓
Releases destructive enzymes:
• Matrix metalloproteinases (MMP-1, 3, 13) - degrade collagen
• Aggrecanases (ADAMTS) - degrade proteoglycans
• Cathepsins - lysosomal enzymes
• Plasminogen activator → activates latent collagenase
↓
Cartilage erosion → joint space narrowing
PHASE 5: Bone Erosion (Periarticular Osteoporosis and Marginal Erosions)
TNF-α + IL-1β + IL-17 → Upregulate RANKL expression
(on FLS, osteoblasts, activated T-cells)
↓
RANKL binds RANK on osteoclast precursors
↓
Osteoclast differentiation and activation
(OPG = osteoprotegerin is the decoy receptor that normally inhibits this)
↓
In RA: RANKL/OPG ratio ↑ → osteoclast activity predominates
↓
Periarticular bone erosions (marginal erosions first)
+ Subchondral bone destruction
+ Periarticular osteoporosis
+ Systemic osteoporosis (IL-6 mediated)
Comprehensive Pathogenesis Diagram (Cellular Level)
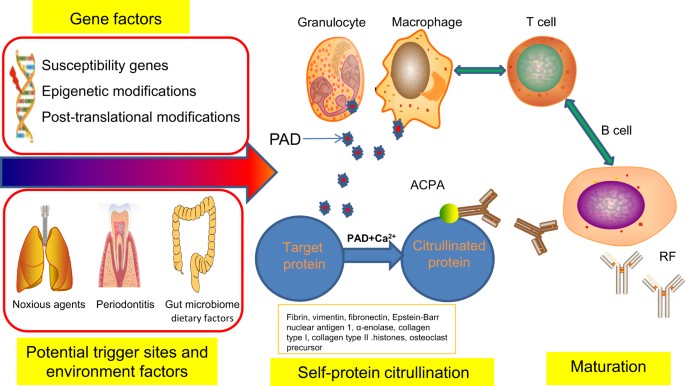
Cellular mechanisms: Gene factors + environmental triggers → PAD-mediated citrullination → ACPA production → T-cell and B-cell activation → RF maturation. (Bone Research, Springer Nature)
Histopathology of the RA Joint
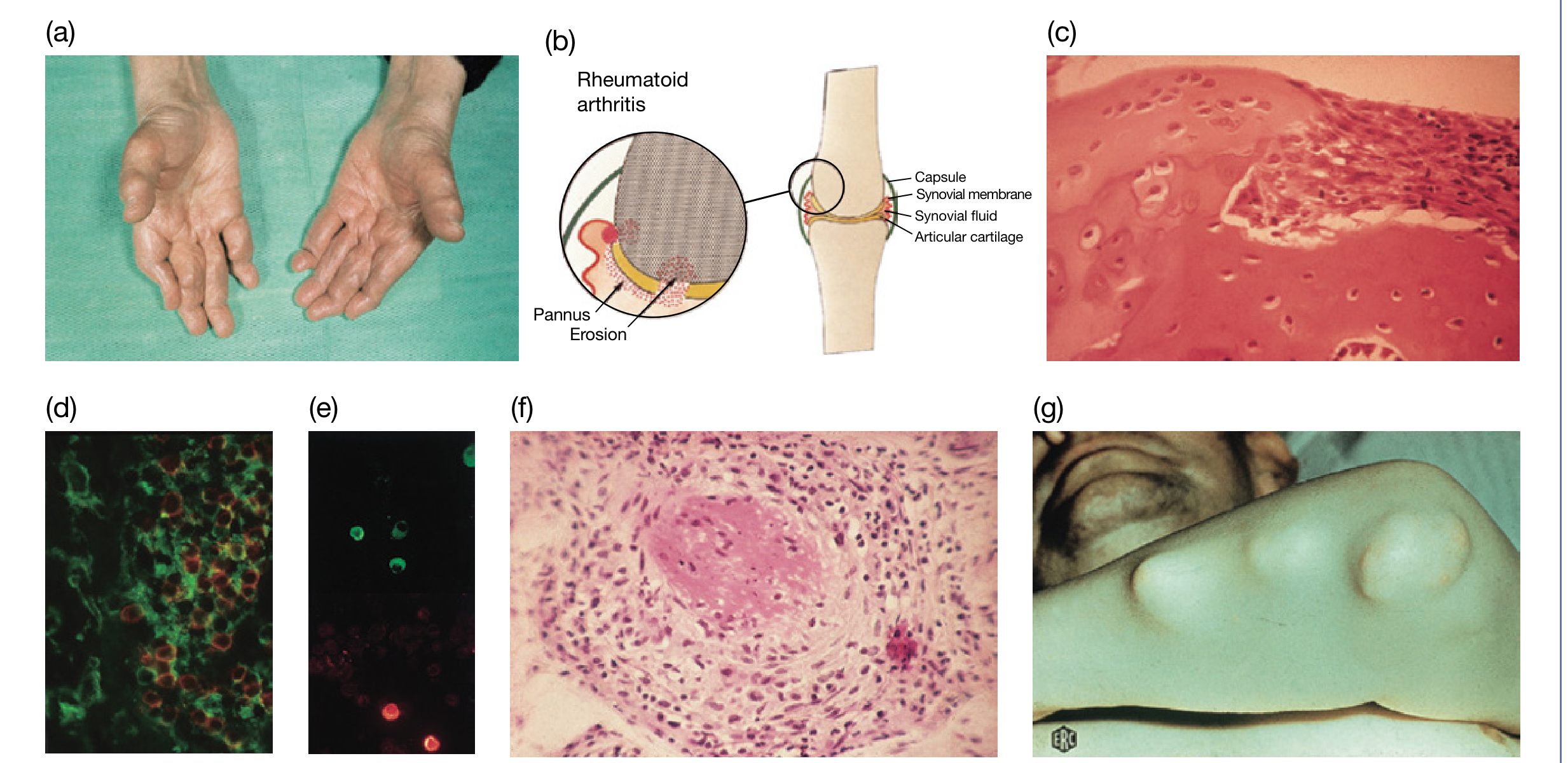
From Roitt's Essential Immunology: (a) RA hands, (b) Pannus overlying and eroding cartilage/bone diagram, (c) Histology of pannus eroding cartilage, (d) Class II-positive APCs in contact with CD4+ T-cells, (e) Plasma cells producing rheumatoid factor, (f-g) Rheumatoid nodule - granulomatous appearance with central necrosis.
Key histological features:
- Synovial lining hyperplasia (villous proliferation)
- Dense lymphocytic infiltrate - CD4+ T-cells with macrophages and dendritic cells
- Plasma cells producing RF (often forming secondary follicles with germinal centers)
- Pannus tissue - fibrovascular granulation tissue at cartilage-pannus junction
- Neovascularization throughout inflamed synovium
- Rheumatoid nodules - central fibrinoid necrosis surrounded by palisading macrophages
Roitt's Essential Immunology, p. 538-539
Cytokine Pathways (Inflammation Cascade)
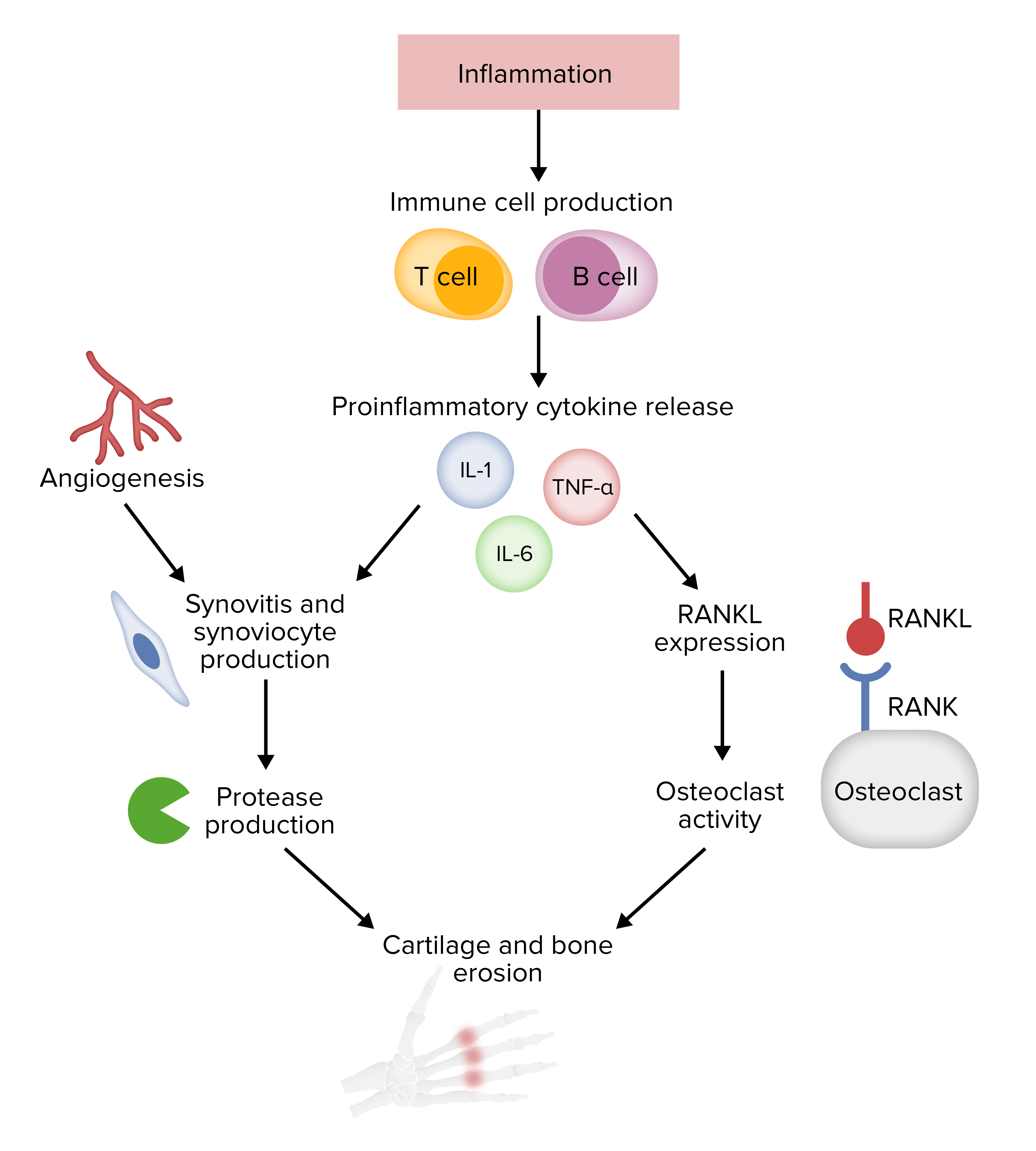
Key cytokine pathways linking immune activation to joint destruction.
Orthopaedic Consequences of Pathogenesis
The synovitis-driven pathogenesis produces predictable joint destruction patterns:
| Mechanism | Orthopaedic Consequence |
|---|---|
| Synovitis + capsular laxity | Joint instability, subluxation |
| Pannus + MMP release | Cartilage loss, joint space narrowing |
| RANKL-driven osteoclastogenesis | Marginal erosions, subchondral cysts, periarticular osteoporosis |
| Tendon sheath synovitis | Tendon rupture (extensor > flexor in hand) |
| Ligament attenuation | Ulnar drift (MCP), swan-neck, boutonniere deformity |
| Cervical synovitis (C1-C2) | Atlantoaxial instability (life-threatening) |
| Foot forefoot synovitis | MTP subluxation, hallux valgus, claw toes |
Miller's Review of Orthopaedics 9th Edition; Campbell's Operative Orthopaedics 15th Ed 2026
IgG Rheumatoid Factor and Immune Complex Formation
A unique feature of RA: IgG rheumatoid factors are both antigen and antibody simultaneously, allowing self-association into IgG aggregates. These:
- Deposit in synovial tissues and joint fluid
- Are stabilized by IgM-RF and C1q (polyvalent Fcγ-binding)
- Attract neutrophils → release reactive oxygen intermediates (ROIs) + lysosomal enzymes (neutral proteases, collagenase)
- When adherent to cartilage, cause "frustrated phagocytosis" → extracellular hydrolase release
Roitt's Essential Immunology, p. 538
Summary: Etiopathogenesis in One Schematic
GENETIC SUSCEPTIBILITY (HLA-DRB1, PTPN22)
+
ENVIRONMENTAL TRIGGER (smoking, infection, PAD activation)
↓
PROTEIN CITRULLINATION → ACPA + RF production
↓
ANTIGEN PRESENTATION (DCs, macrophages via MHC II)
↓
CD4+ T-CELL ACTIVATION → Th1 / Th17 differentiation
↓
B-CELL ACTIVATION → PLASMA CELLS → RF + ACPA
↓
IMMUNE COMPLEX FORMATION in synovium
↓
COMPLEMENT ACTIVATION + Fc receptor stimulation
↓
CYTOKINE STORM: TNF-α, IL-1β, IL-6, IL-15, IL-17
↓
SYNOVIAL HYPERPLASIA + ANGIOGENESIS
↓
PANNUS FORMATION (invasive hyperplastic synovium)
↓
MMP + Cathepsin release ──→ CARTILAGE EROSION
↓
RANKL upregulation ──→ OSTEOCLAST ACTIVATION → BONE EROSION
↓
JOINT DEFORMITY + FUNCTIONAL DISABILITY
Key Biomarkers in Pathogenesis
| Marker | Sensitivity | Specificity | Significance |
|---|---|---|---|
| RF (IgM) | 70-80% | 85% | Formed early; immune complex formation |
| Anti-CCP (ACPA) | 67% | 95%+ | Most specific; precedes symptoms by years |
| CRP / ESR | Non-specific | Non-specific | Acute-phase response driven by IL-6 |
| Anti-MCV | ~70% | ~90% | Anti-mutated citrullinated vimentin |
Therapeutic Targets Based on Pathogenesis
Understanding etiopathogenesis directly informs orthopaedic pharmacological management:
- TNF-α inhibitors (etanercept, infliximab, adalimumab) - must be discontinued perioperatively due to infection risk
- IL-6 receptor antagonists (tocilizumab)
- T-cell costimulation blockers (abatacept - blocks CD28/B7 interaction)
- B-cell depletion (rituximab - anti-CD20)
- JAK inhibitors (tofacitinib, baricitinib) - block cytokine signalling
- Methotrexate, hydroxychloroquine, prednisone - can generally be continued perioperatively
- Anti-RANKL (denosumab) - targets the RANKL/RANK/OPG pathway directly
Miller's Review of Orthopaedics 9th Ed; Campbell's Operative Orthopaedics 15th Ed 2026
This is a shared conversation. Sign in to Orris to start your own chat.