Chloroquine resistant malaria pharmacotherapy management
Reading File
Finding Sources
Finding Sources
Searching PubMed
"chloroquine resistant malaria" AND treatment
Reading File
Reading File
Reading File
Searching PubMed
"malaria" AND "artemisinin" AND treatment
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, authoritative data from Goodman & Gilman, Katzung, Lippincott, and Red Book to compose a thorough answer. Let me write the complete response.
Chloroquine-Resistant Malaria: Pharmacotherapy Management
Background and Resistance Epidemiology
Chloroquine-resistant strains of Plasmodium falciparum are now the rule, not the exception in most malaria-endemic regions. Resistance is driven by mutations in the pfcrt gene (chloroquine resistance transporter). Multidrug-resistant P. falciparum is especially prevalent and severe in Southeast Asia and Oceania, where infections may not even respond adequately to mefloquine or quinine. Chloroquine-resistant P. vivax (CRPV) has been well documented in Papua New Guinea and Indonesia, with rare case reports from Myanmar, India, and parts of the Americas.
Chloroquine remains effective only against: P. ovale, P. malariae, P. knowlesi, most strains of P. vivax (outside the above endemic regions), and chloroquine-sensitive P. falciparum.
Diagnostic Algorithm
The treatment algorithm shown below (from Goodman & Gilman) guides the management decision:
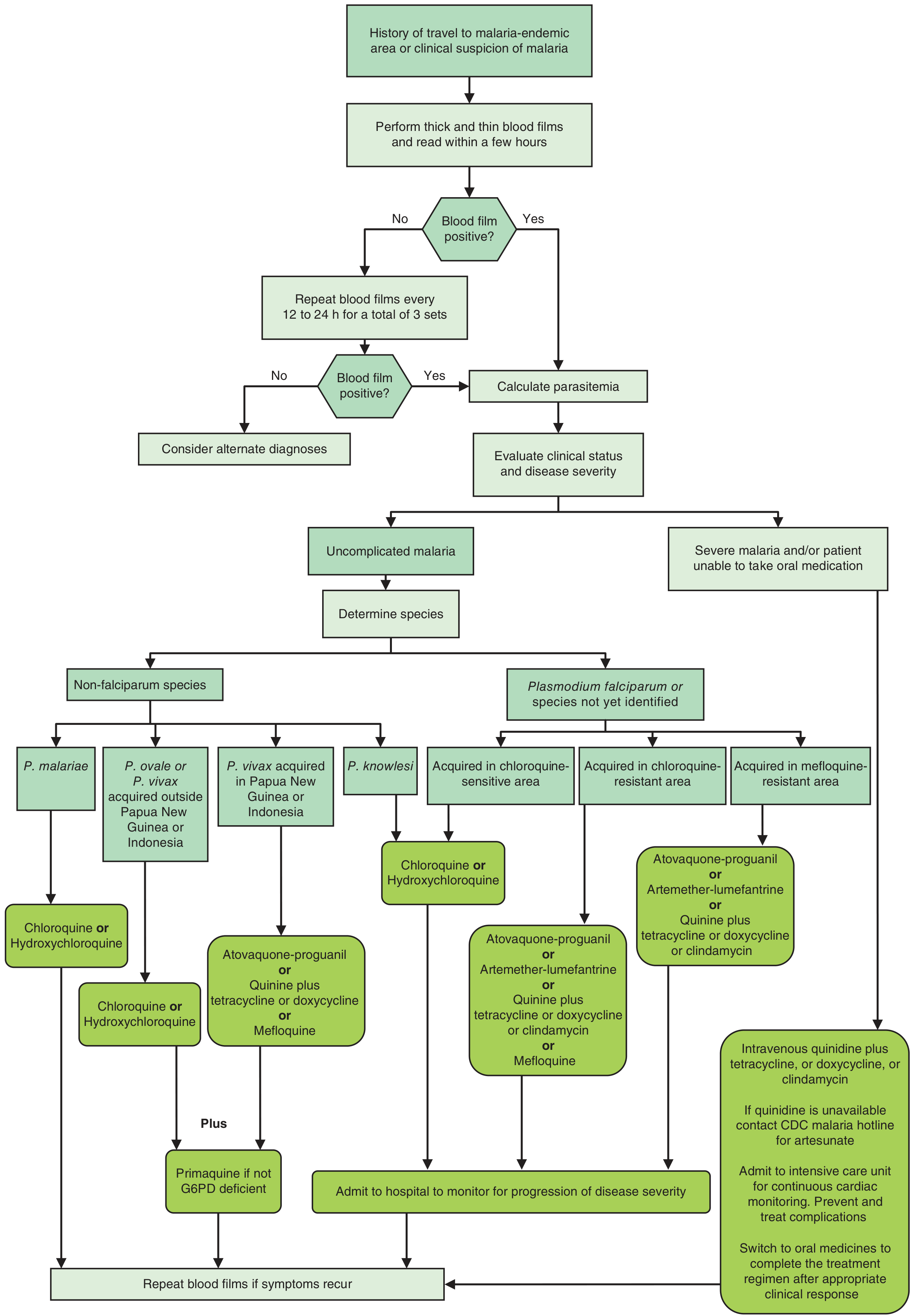
Decision algorithm for the treatment of malaria - Goodman & Gilman's The Pharmacological Basis of Therapeutics
I. Uncomplicated Chloroquine-Resistant P. falciparum (Oral Therapy)
First-Line: Artemisinin-Based Combination Therapies (ACTs)
ACTs are the cornerstone of treatment. The artemisinin component acts as a rapid-acting blood schizonticide; the partner drug provides sustained parasite clearance. Partner drugs are chosen for potency and a t½ that substantially exceeds that of the artemisinin component to prevent resistance.
1. Artemether-Lumefantrine (Coartem) - FDA-approved first choice in the US
| Parameter | Details |
|---|---|
| Tablet | 20 mg artemether / 120 mg lumefantrine |
| Adult dose | 4 tablets/dose: Day 1 - two doses 8 h apart; then one dose twice daily x 2 more days (6 doses total) |
| Pediatric dose | 5-15 kg: 1 tablet/dose; 15-25 kg: 2 tablets/dose; 25-<35 kg: 3 tablets/dose; >35 kg: 4 tablets/dose (same 3-day schedule) |
| Key note | Take with food or whole milk (fat significantly increases lumefantrine absorption). If vomiting within 30 min, repeat dose. |
| Adverse effects | Headache, anorexia, dizziness, arthralgia, myalgia; in children: fever, cough, vomiting |
| Contraindication | Avoid in first trimester of pregnancy |
Artemether-lumefantrine is the most widely used first-line antimalarial across Africa, with high efficacy and a favorable safety profile. - Goodman & Gilman's The Pharmacological Basis of Therapeutics, p. 1321
2. Atovaquone-Proguanil (Malarone)
| Parameter | Details |
|---|---|
| Adult tablet | 250 mg atovaquone / 100 mg proguanil |
| Adult dose | 4 adult tablets once daily x 3 days |
| Pediatric dose | Pediatric tablet (62.5 mg/25 mg): 5-8 kg: 2 ped tabs; 8-10 kg: 3 ped tabs; 10-20 kg: 1 adult tab; 20-30 kg: 2 adult tabs; 30-40 kg: 3 adult tabs; >40 kg: 4 adult tabs - all x 3 days |
| Mechanism | Atovaquone inhibits mitochondrial electron transport (cytochrome bc1 complex); proguanil inhibits DHFR |
| Adverse effects | Abdominal pain, nausea, vomiting, diarrhea, headache, elevated LFTs |
| Contraindications | CrCl <30 mL/min (severe renal impairment); not generally recommended in pregnancy; must be taken with food |
3. Quinine Sulfate + Partner Drug
Quinine alone is not recommended because resistance develops rapidly; it is paired with a second agent to shorten the course and limit toxicity.
| Partner Drug | Regimen | Note |
|---|---|---|
| Quinine + Doxycycline | Quinine 650 mg TID x 3 days (SE Asia: x 7 days) + Doxycycline 100 mg BID x 7 days | Not in children <8 yr or pregnancy |
| Quinine + Tetracycline | Quinine 650 mg TID + Tetracycline 250 mg QID x 7 days | Same restrictions as doxycycline |
| Quinine + Clindamycin | Quinine 650 mg TID x 7 days + Clindamycin 20 mg/kg/day divided TID x 7 days | Preferred in children <8 yr and in pregnancy |
Cinchonism (tinnitus, headache, nausea, dizziness, visual disturbances) is common with quinine. Severe toxicity includes hypoglycemia (stimulates insulin), QT prolongation, hemolysis in G6PD deficiency, and blackwater fever. Quinine IV/IM preparations are not available in the USA (availability ended 2019). - Katzung's Basic and Clinical Pharmacology, 16th Ed.
4. Mefloquine (Monotherapy or Alternative)
- Dose: 750 mg orally, then 500 mg 6-12 h later (total 1250 mg in adults); 25 mg/kg split over 24 h in children
- Effective for chloroquine-resistant strains but not recommended for infections acquired in Southeast Asia due to high mefloquine resistance
- Neuropsychiatric adverse effects (anxiety, vivid dreams, psychosis, seizures) limit use; contraindicated with concurrent quinine
II. Uncomplicated Chloroquine-Resistant P. vivax (CRPV)
Three options are recommended equally:
- Atovaquone-proguanil (as above dosing)
- Artemether-lumefantrine (as above dosing)
- Mefloquine (as above dosing; use if no other option in children <8 yr)
Plus radical cure with: Primaquine 30 mg base/day x 14 days (or 15 mg/day x 14 days for mild CRPV) after G6PD testing, to eliminate hypnozoites and prevent relapse. Tafenoquine (300 mg single dose) is an alternative for radical cure in adults (also requires G6PD testing).
For patients acquiring P. vivax outside Papua New Guinea or Indonesia: start with chloroquine; if the patient does not respond, switch to a CRPV regimen and notify the CDC. - Red Book 2021, p. 1400
III. Severe/Complicated Malaria (Parenteral Therapy)
Severe malaria = high parasitemia, cerebral malaria, renal failure, severe anemia, respiratory distress, hypoglycemia, or inability to take oral medication.
Preferred: Intravenous Artesunate
IV Artesunate is now the treatment of choice for severe falciparum malaria, having replaced quinidine.
| Parameter | Details |
|---|---|
| Dose | 2.4 mg/kg IV at 0, 12, and 24 h, then reassess |
| Follow-on oral therapy | Once tolerating oral meds: Artemether-lumefantrine OR Atovaquone-proguanil OR Quinine + doxycycline OR Mefloquine |
| Access | Obtain via CDC Malaria Hotline: 770-488-7100 (8 AM-5 PM ET) or 855-856-4713 (after hours) |
Adverse effects: Thrombocytopenia, hemolytic anemia, elevated liver enzymes, hyperbilirubinemia. Delayed hemolysis occurs in ~13% of cases, typically 2-3 weeks post-treatment, with ~73% of cases requiring transfusion. - Katzung, p. 1438
Alternative if Artesunate Unavailable: IV Quinidine Gluconate (historical)
Quinidine was used before artesunate availability; requires ICU admission with continuous cardiac monitoring due to QT prolongation risk.
IV. Other ACT Regimens (WHO-endorsed, widely used outside US)
| ACT | Partner Drug t½ | Notable Use |
|---|---|---|
| Artesunate-Amodiaquine | 9-18 days (monodesethyl-amodiaquine) | First-line in many African countries |
| Artesunate-Mefloquine | ~21 days | Used in Southeast Asia |
| Artesunate-Pyronaridine | - | Approved in Africa, Asia |
| Dihydroartemisinin-Piperaquine (DHA-PPQ) | 5 weeks (longest of all) | Effective in Africa; resistance emerging in Cambodia due to pfpm2 amplification |
- Goodman & Gilman's, p. 1321
V. Special Populations
Pregnancy
| Trimester | Uncomplicated CR-Falciparum | Severe Malaria |
|---|---|---|
| 1st trimester | Quinine + clindamycin (preferred); ACTs may be used if benefits outweigh risks | IV artesunate |
| 2nd-3rd trimester | Artemether-lumefantrine (recommended) | IV artesunate |
- Atovaquone-proguanil: not generally recommended in pregnancy (limited safety data)
- Doxycycline/tetracycline: avoid in pregnancy unless no other option
- Do NOT use primaquine or tafenoquine (risk of hemolysis in G6PD-unknown fetus)
- Maintain chloroquine prophylaxis through pregnancy for P. vivax/ovale; treat hypnozoites postpartum
Children <8 years
- Atovaquone-proguanil (>5 kg): safe, preferred
- Artemether-lumefantrine (>5 kg): safe, preferred
- Mefloquine: if no other option available
- Doxycycline/tetracycline: avoid except in emergency
- Clindamycin replaces doxycycline as quinine partner in this age group
G6PD Deficiency
- Avoid primaquine and tafenoquine in G6PD-deficient patients (risk of hemolytic anemia)
- If radical cure is necessary in mild G6PD deficiency: primaquine 45 mg once weekly x 8 weeks with expert consultation
VI. Chemoprophylaxis in Chloroquine-Resistant Areas
For travelers to chloroquine-resistant endemic areas, three options are equivalent:
| Drug | Dosing | Notes |
|---|---|---|
| Atovaquone-proguanil | 1 adult tab/day (start 1-2 days before, continue 7 days after) | Best for short-term travel |
| Doxycycline | 100 mg/day (start 1-2 days before, continue 4 weeks after) | Avoid in <8 yr, pregnancy |
| Mefloquine | 250 mg/week (start 2-3 weeks before, continue 4 weeks after) | Best documented for long-term travelers; avoid in SE Asia mefloquine-resistant areas |
Trimethoprim-sulfamethoxazole (daily prophylaxis in HIV-infected patients) provides partial preventive efficacy against malaria in Africa but is not a primary antimalarial prophylactic. - Katzung, p. 1443-1444
VII. Resistance Mechanisms and Emerging Threats
| Mechanism | Drug Affected |
|---|---|
| pfcrt mutation (K76T and others) | Chloroquine resistance |
| pfkelch13 mutations | Artemisinin partial resistance (Southeast Asia, now Africa) |
| pfpm2 copy number amplification | Dihydroartemisinin-piperaquine resistance (Cambodia) |
| pfdhfr/pfdhps mutations | Sulfadoxine-pyrimethamine resistance |
Artemisinin partial resistance (delayed parasite clearance) is now spreading from Southeast Asia into sub-Saharan Africa - a critical threat to malaria control globally.
Drugs in development:
- Ganaplacide (KAF156) - imidazolopiperazine; active on asexual forms and gametocytes of both P. falciparum and P. vivax (Phase II with solid dispersible lumefantrine)
- Cipargamin (KAE609) - spiroindolone; blood schizonticide (field trials)
- Ferroquine + artefenomel - retains activity against chloroquine-resistant AND piperaquine-resistant strains
- Monoclonal antibodies targeting PfCSP (Phase I) - Goodman & Gilman's, p. 1322
Quick Reference Summary Table
| Scenario | Preferred Regimen |
|---|---|
| Uncomplicated CR P. falciparum | Artemether-lumefantrine OR Atovaquone-proguanil |
| Alternative oral regimens | Quinine + doxycycline; Quinine + clindamycin (children/pregnancy); Mefloquine (not SE Asia) |
| CRPV (P. vivax) | Atovaquone-proguanil OR Artemether-lumefantrine + primaquine |
| Severe malaria (parenteral) | IV Artesunate 2.4 mg/kg at 0, 12, 24 h → oral follow-on ACT |
| Pregnancy (1st tri) | Quinine + clindamycin; IV artesunate if severe |
| Pregnancy (2nd-3rd tri) | Artemether-lumefantrine; IV artesunate if severe |
| Children <8 yr | Atovaquone-proguanil or Artemether-lumefantrine; avoid doxycycline |
| Chemoprophylaxis (CR area) | Atovaquone-proguanil, Doxycycline, or Mefloquine |
Sources:
- Goodman & Gilman's The Pharmacological Basis of Therapeutics (Tables 66-2 and 66-3), pp. 1321-1324
- Katzung's Basic and Clinical Pharmacology, 16th Ed., pp. 1438-1444
- Lippincott Illustrated Reviews: Pharmacology, pp. 1176-1178
- Red Book 2021 (AAP), pp. 1399-1400
- CDC Malaria Hotline for IV artesunate access: 770-488-7100
Lower UTI dt psudomonas sps - enlist drugs used , MOA of drugs , A/E of these drugs , instructions to pt to prevent future inf
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
I now have comprehensive data from multiple authoritative textbooks. Let me compose the full answer.
Lower UTI due to Pseudomonas aeruginosa - Complete Pharmacotherapy Guide
Why Pseudomonas UTI is Clinically Significant
Pseudomonas aeruginosa is an inherently resistant, opportunistic gram-negative bacillus. It rarely infects healthy individuals; UTI typically occurs in patients with urinary catheters, structural urinary tract abnormalities, immunocompromise, recent antibiotic exposure, or prolonged hospitalization. Its intrinsic multi-drug resistance mechanisms (efflux pumps, AmpC β-lactamases, reduced outer membrane permeability) make it one of the most challenging urinary pathogens. Treatment must always be guided by urine culture and sensitivity (C&S).
I. Drugs Used for Pseudomonas Lower UTI
A. Fluoroquinolones (Oral - First-line for uncomplicated lower UTI)
| Drug | Route | Dosing |
|---|---|---|
| Ciprofloxacin | Oral/IV | 250-500 mg BID x 7 days (oral); 400 mg IV BID |
| Levofloxacin | Oral/IV | 250-750 mg OD x 5-7 days |
Ciprofloxacin is the most active fluoroquinolone against Pseudomonas and is the oral drug of choice for uncomplicated lower Pseudomonas UTI when the isolate is susceptible.
B. Antipseudomonal β-Lactams (IV - For complicated/hospitalized cases)
| Drug | Class | Route |
|---|---|---|
| Piperacillin-tazobactam | Extended-spectrum penicillin + β-lactamase inhibitor | IV |
| Ceftazidime | 3rd-gen antipseudomonal cephalosporin | IV |
| Cefepime | 4th-gen cephalosporin | IV |
| Ceftolozane-tazobactam | Novel cephalosporin + BLI | IV |
| Ceftazidime-avibactam | Cephalosporin + novel BLI | IV |
| Aztreonam | Monobactam | IV |
| Imipenem-cilastatin | Carbapenem | IV |
| Meropenem | Carbapenem | IV |
C. Aminoglycosides
| Drug | Route | Use |
|---|---|---|
| Tobramycin | IV / IM | UTI monotherapy or combination |
| Gentamicin | IV / IM | Combination with β-lactams |
| Amikacin | IV / IM | MDR strains (less vulnerable to modifying enzymes) |
Aminoglycosides are particularly useful for Pseudomonas UTI because >90% is excreted unchanged in urine, achieving high urinary concentrations. Tobramycin alone is appropriate for uncomplicated Pseudomonas UTI. - Lippincott Illustrated Reviews: Pharmacology, p. 993
D. Polymyxins (Reserve agents - MDR/XDR strains)
| Drug | Route | Use |
|---|---|---|
| Colistin (Polymyxin E) | IV / nebulized | Extensively drug-resistant (XDR) Pseudomonas |
| Polymyxin B | IV | Same as above |
Used only when all other options have failed or the isolate is pan-drug-resistant.
E. Novel β-Lactam/β-Lactamase Inhibitor Combinations (MDR strains)
| Drug | Use |
|---|---|
| Ceftolozane-tazobactam (Zerbaxa) | MDR Pseudomonas; active against ceftazidime-resistant strains via β-lactamase overexpression |
| Ceftazidime-avibactam | KPC-producing and ESBL-producing strains |
| Imipenem-cilastatin-relebactam | Approved for hospital-acquired infections including UTI |
| Meropenem-vaborbactam (Vabomere) | Approved for complicated UTI including pyelonephritis |
| Cefiderocol | Pan-drug-resistant strains (acts as siderophore, stable against metallo-β-lactamases) |
II. Mechanism of Action of Each Drug Class
1. Fluoroquinolones (Ciprofloxacin, Levofloxacin)
- Target: Bacterial topoisomerase II (DNA gyrase, encoded by gyrA/gyrB) and topoisomerase IV (encoded by parC/parE)
- Action: Bind to and stabilize the DNA-enzyme complex, preventing re-ligation of DNA strands after the enzyme cuts them for replication and transcription - this leads to double-strand DNA breaks
- Net effect: Bactericidal - prevents DNA replication, transcription, repair and recombination
- Pseudomonas is susceptible primarily via DNA gyrase inhibition (GyrA subunit is the primary target)
2. β-Lactams (Penicillins, Cephalosporins, Carbapenems, Monobactams)
- Target: Penicillin-binding proteins (PBPs) - specifically transpeptidase enzymes in the bacterial cell membrane
- Action: Structurally mimic the terminal D-Ala-D-Ala portion of peptidoglycan precursors; covalently bind and irreversibly inhibit PBPs, blocking transpeptidation - the final cross-linking step of peptidoglycan cell wall synthesis
- Loss of structural integrity → osmotic lysis → bactericidal
- β-lactamase inhibitors (tazobactam, avibactam, vaborbactam, relebactam) bind and irreversibly inactivate β-lactamase enzymes, protecting the β-lactam partner from hydrolysis
- Cefiderocol additionally acts as a siderophore - chelates free iron and uses bacterial iron-uptake channels to achieve high periplasmic concentrations, overcoming efflux-pump and porin-loss resistance
3. Aminoglycosides (Tobramycin, Gentamicin, Amikacin)
- Target: 30S ribosomal subunit (16S rRNA)
- Action (3-step process):
- Ionic binding to the negatively charged outer membrane, displacing Ca²+ and Mg²+ → increases membrane permeability
- Energy-dependent phase I (EDP-I): Small amounts enter and bind to the 30S subunit → misreading of mRNA codons → production of abnormal proteins → inserted into cell membrane → increased permeability
- Energy-dependent phase II (EDP-II): Massive drug influx → complete inhibition of protein synthesis
- Net effect: Concentration-dependent bactericidal killing
- Resistance via: (a) efflux pumps, (b) decreased uptake, (c) aminoglycoside-modifying enzymes (AMEs) encoded on plasmids - amikacin and plazomicin are least affected by AMEs
4. Polymyxins (Colistin/Polymyxin E, Polymyxin B)
- Target: Gram-negative outer membrane (lipopolysaccharide - LPS)
- Action: Cationic cyclic peptides that bind to the negatively charged phosphate groups of lipid A (LPS component); this electrostatic interaction displaces Ca²+ and Mg²+ that stabilize the outer membrane, disrupting and permeabilizing both the outer membrane and cytoplasmic membrane
- Result: Cell contents leak out → rapid bactericidal killing (detergent-like effect)
- Resistance can emerge via mcr-1 (plasmid-mediated phosphoethanolamine transferase) that reduces negative charge on the cell surface, reducing polymyxin binding - Harrison's Principles of Internal Medicine 22E, p. 1229
III. Adverse Effects
1. Fluoroquinolones
| System | Adverse Effect |
|---|---|
| GI | Nausea, vomiting, diarrhea, C. difficile colitis |
| CNS | Headache, dizziness, insomnia, seizures (lower threshold), confusion (especially elderly) |
| Musculoskeletal | Tendinopathy and tendon rupture (Achilles tendon most common - Black Box Warning); arthropathy in children |
| Cardiac | QT interval prolongation → risk of torsades de pointes |
| Metabolic | Hypo- or hyperglycemia (especially with concurrent hypoglycemics) |
| Eyes | Photosensitivity; retinal detachment (rare, controversial) |
| Other | Peripheral neuropathy (Black Box Warning); aortic aneurysm/dissection (FDA warning) |
| Special populations | Avoid in pregnancy, children <18 yr, myasthenia gravis |
2. Antipseudomonal β-Lactams (Piperacillin-tazobactam, Ceftazidime, Cefepime, Carbapenems)
| Adverse Effect | Notes |
|---|---|
| Hypersensitivity | Rash, urticaria, anaphylaxis (1-4%); cross-reactivity between penicillins and cephalosporins ~2% |
| GI | Nausea, diarrhea, C. difficile (especially with broad-spectrum agents) |
| Hematologic | Neutropenia, thrombocytopenia (piperacillin-tazobactam - especially with prolonged use) |
| CNS - Cefepime | Neurotoxicity (encephalopathy, myoclonus, non-convulsive status epilepticus) - particularly in renal failure (dose reduction required) |
| Carbapenems | Seizures (imipenem > meropenem, dose-dependent); nausea/vomiting; elevated LFTs |
| Electrolytes | Hypokalemia (piperacillin - high sodium load) |
3. Aminoglycosides
| Adverse Effect | Details |
|---|---|
| Nephrotoxicity ⚠️ | Aminoglycoside accumulation in proximal tubular cells disrupts Ca²+-mediated transport → acute tubular necrosis (mild reversible → irreversible). Risk ↑ with duration, concurrent NSAIDs, vancomycin, cisplatin, contrast agents |
| Ototoxicity ⚠️ | Accumulates in endolymph/perilymph of inner ear; vestibular (vertigo, ataxia - streptomycin > others) and cochlear (high-frequency hearing loss - may be irreversible); risk ↑ with loop diuretics, cisplatin |
| Neuromuscular blockade | Risk with rapid infusion or concurrent neuromuscular blockers; particularly dangerous in myasthenia gravis. Reverse with IV calcium gluconate |
| Allergic reactions | Rare; contact dermatitis common with topical neomycin |
| Monitoring required | Therapeutic drug monitoring (TDM) of peaks and troughs - Lippincott, p. 996 |
4. Polymyxins (Colistin, Polymyxin B)
| Adverse Effect | Details |
|---|---|
| Nephrotoxicity ⚠️ | Dose-dependent; occurs in 20-50% of patients (acute tubular injury); requires dose reduction for CrCl <50 mL/min |
| Neurotoxicity | Paresthesias, dizziness, ataxia, facial numbness; neuromuscular blockade |
| Respiratory | Bronchospasm with inhaled colistin |
| Infusion-related | Hypotension, flushing with rapid IV infusion |
IV. Patient Instructions to Prevent Future Pseudomonas UTI
Hygiene and Behavioral Measures
- Wipe front to back after bowel movements (in women) - prevents fecal organisms, including Pseudomonas, from reaching the urethra
- Void before and after sexual intercourse - flushes out any organisms introduced during activity
- Do not delay urination - avoid "holding" urine for prolonged periods; urinate every 3-4 hours
- Adequate hydration - drink 6-8 glasses (1.5-2 L) of water daily to dilute urine and flush the urinary tract
- Avoid harsh soaps, douches, or bubble baths in the genital area - these disrupt natural flora and can introduce pathogens
- Wear breathable, cotton underwear and avoid tight-fitting clothing that traps moisture
Catheter-Specific Instructions (if applicable)
- Limit catheter use - use urinary catheters only when medically necessary; remove as early as possible
- Maintain closed drainage system - never disconnect the catheter from the drainage bag unnecessarily
- Keep drainage bag below bladder level at all times to prevent backflow
- Daily catheter hygiene - clean the urethral meatus and catheter junction with soap and water daily
- Change catheters regularly per medical advice - do not reuse disposable catheters
Medication and Compliance
- Complete the full antibiotic course - never stop antibiotics early even if symptoms resolve; incomplete treatment promotes resistance
- Do not self-medicate - never use leftover antibiotics for UTI symptoms; Pseudomonas requires sensitivity-guided therapy
- Disclose all medications - inform your doctor of any immunosuppressants or corticosteroids, as these increase susceptibility
Risk Factor Modification
- Manage underlying conditions - control diabetes optimally (high blood glucose promotes bacterial growth in urine)
- Treat urinary obstruction - bladder stones, enlarged prostate (BPH), or strictures must be addressed, as these predispose to recurrent infections
- Probiotic consideration - Lactobacillus-based probiotics may help restore normal urinary/vaginal flora (discuss with physician)
- Avoid antibiotic overuse - prior antibiotic exposure is a key risk factor for Pseudomonas UTI; use antibiotics only when prescribed
When to Seek Immediate Care
- Fever >38°C, rigors, flank pain, or back pain (suggests upper tract spread/pyelonephritis)
- Gross hematuria (blood in urine)
- Worsening symptoms despite antibiotics
- Persistent symptoms >48 hours after starting treatment
Quick Summary Table
| Drug Class | Key Agents | MOA | Key Adverse Effects |
|---|---|---|---|
| Fluoroquinolones | Ciprofloxacin, Levofloxacin | DNA gyrase/topo IV inhibition → DNA breaks | Tendon rupture, QT prolongation, peripheral neuropathy, CNS effects |
| Antipseudomonal β-lactams | Pip-tazo, Ceftazidime, Cefepime, Meropenem | PBP inhibition → block peptidoglycan cross-linking | Hypersensitivity, C. diff, neurotoxicity (cefepime), seizures (imipenem) |
| Aminoglycosides | Tobramycin, Gentamicin, Amikacin | 30S ribosomal binding → protein synthesis inhibition + membrane disruption | Nephrotoxicity, ototoxicity, NMJ blockade |
| Polymyxins | Colistin, Polymyxin B | LPS binding → outer + inner membrane disruption | Nephrotoxicity, neurotoxicity, NMJ blockade |
Sources:
- Lippincott Illustrated Reviews: Pharmacology, pp. 993-997
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, pp. 1177-1178
- Harrison's Principles of Internal Medicine 22E, pp. 1228-1229
- Bailey and Love's Short Practice of Surgery 28th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.