
Screenshot_20260520-101345.jpg
Ans
Answer: 3. Parietal
The parietal lobe is responsible for hand-eye coordination. It integrates sensory information — particularly somatosensory (touch, proprioception) and visual inputs — to guide coordinated movements between the hands and eyes.
Key points:
- The posterior parietal cortex (areas 5 and 7) is critical for visuomotor integration — it processes where objects are in space and directs hand movements accordingly.
- It receives input from both the somatosensory cortex (body position/touch) and the visual cortex, combining them to produce coordinated motor actions.
- Lesions here cause optic ataxia (inability to reach accurately for visually presented objects) and ideomotor apraxia.
The other lobes' roles:
- Frontal — motor execution and planning
- Temporal — auditory processing, memory, object recognition
- Occipital — primary visual processing (but not coordination itself)
Explain the neural pathways involved in visuomotor integration
Reading File
Acc to me all lobes are somehow integrated with vision can you explain how and lesion of each produces which defect
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Excellent — great textbook material retrieved. Here is the complete explanation:
Vision and All Four Lobes — How They're Connected & Lesion Deficits
You're absolutely right — vision is not just "occipital lobe stuff." It's a whole-brain enterprise. Here's how it works systematically.
The Core Visual Pathway (Substrate for Everything Below)
Retina → Optic nerve → Optic chiasm → Optic tract → Lateral Geniculate Nucleus (LGN, thalamus) → Optic radiation → Primary Visual Cortex (V1, Area 17, occipital lobe)
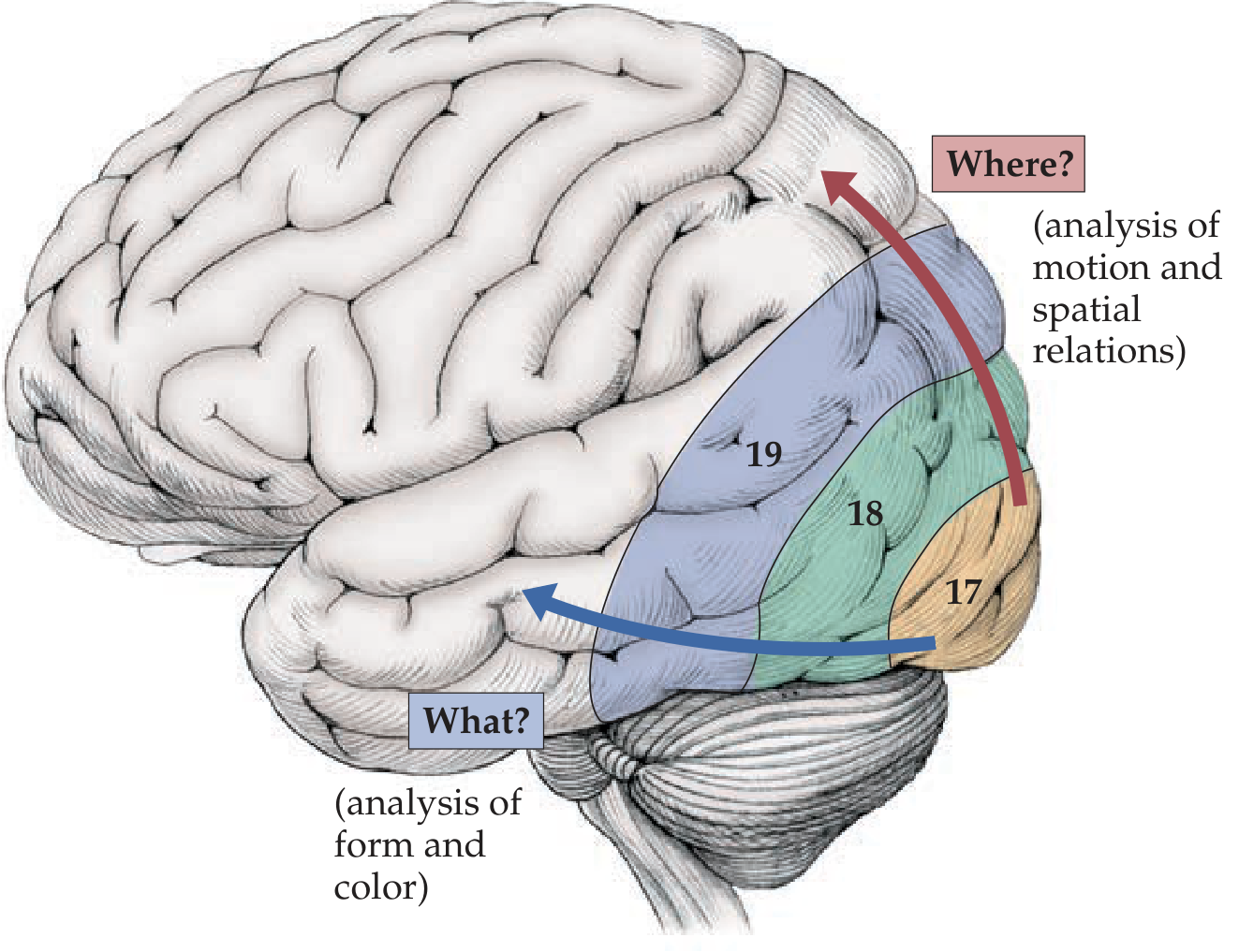
From V1, information splits into two major processing streams:
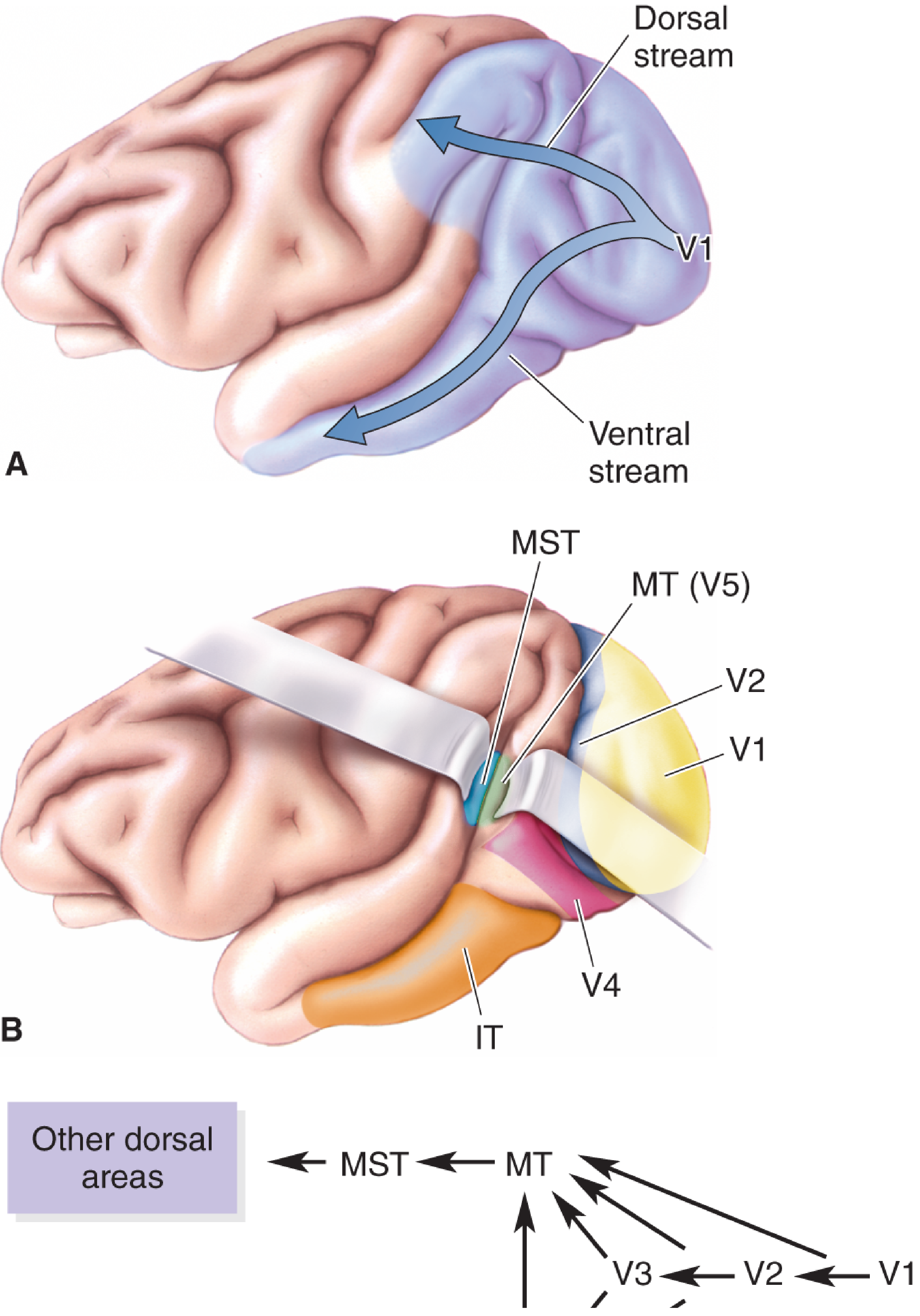
| Stream | Direction | Destination | Answers |
|---|---|---|---|
| Ventral stream | V1 → V2 → V4 → Inferotemporal cortex | Temporal lobe | "WHAT is it?" — form, color, face recognition |
| Dorsal stream | V1 → V2 → V3 → MT/V5 → MST → Posterior parietal cortex | Parietal lobe | "WHERE is it?" — motion, spatial relations, visuomotor guidance |
🟠 OCCIPITAL LOBE — The Primary Visual Processor
Role: Houses V1 (striate cortex, Area 17), V2 (Area 18), V3/V4/V5 (Area 19). Receives all visual input first. Processes basic features — orientation, contrast, color, motion.
Lesion Effects:
| Location | Defect |
|---|---|
| V1 (Area 17) unilateral | Contralateral homonymous hemianopia with macular sparing (dual blood supply to macular area) |
| Bilateral V1 | Cortical blindness (Anton's syndrome — patient is blind but denies it) |
| V4 (color area) | Cerebral achromatopsia — loss of color vision despite intact retina/optic nerves |
| V5/MT (motion area) | Akinetopsia — cannot perceive motion (objects appear to "freeze" or jump between positions; pouring water looks like a static statue) |
| Bilateral calcarine | Visual field defects + cortical blindness |
🔵 PARIETAL LOBE — The "WHERE" Stream Terminus
Role: Posterior parietal cortex (Areas 5 & 7) integrates visual + somatosensory + proprioceptive input → spatial awareness, visuomotor guidance, reaching/grasping.
The dorsal stream: V1 → MT → MST → Posterior parietal cortex → Frontal motor areas
Lesion Effects:
| Lesion | Defect |
|---|---|
| Contralateral parietal | Contralateral visual neglect / hemispatial neglect — ignores one side of visual space (not a field defect — they CAN see it, but don't attend to it) |
| Bilateral posterior parietal | Bálint's syndrome — triad of: (1) Simultanagnosia (can only see one object at a time, can't process a whole scene), (2) Optic ataxia (misreaching for visually presented objects), (3) Ocular apraxia/psychic paralysis of gaze (cannot voluntarily direct gaze) |
| Non-dominant (R) parietal | Constructional apraxia, dressing apraxia, topographical disorientation |
| Inferior parietal (angular gyrus) | Visual-verbal disconnection — alexia (can't read despite seeing words) |
"Patients with bilateral parietal injuries can have difficulty putting together the elements of a visual scene (simultanagnosia) and cannot find things in space although they apparently can see (optic ataxia and psychic paralysis of gaze)" — Plum & Posner
🟢 TEMPORAL LOBE — The "WHAT" Stream Terminus
Role: Inferotemporal cortex (IT cortex), fusiform gyrus — object recognition, face recognition, color categorization, and linking visual input to memory/meaning.
The ventral stream: V1 → V2 → V4 → Inferotemporal (IT) cortex → Hippocampus/Amygdala
Lesion Effects:
| Lesion | Defect |
|---|---|
| Fusiform gyrus (bilateral or right) | Prosopagnosia — cannot recognize familiar faces (even own face in mirror), but CAN detect a face as a face; can identify by voice |
| Inferior temporal | Visual object agnosia — cannot recognize objects visually despite intact vision and intact general intelligence; cannot name OR describe use of object |
| Left occipitotemporal | Pure alexia (alexia without agraphia) — cannot read, but CAN write; visual words fail to reach left language areas |
| Right temporal | Impaired face and object identity; visual memory deficits |
| Bilateral anterior temporal | Semantic dementia — loses meaning of words AND fails to recognize faces/objects |
"The deficit in prosopagnosia is modality-specific and reflects the inability of the visual percept to activate the multimodal associations necessary for concept formation. The responsible lesion is in the ventral temporal lobe." — Harrison's 22E
🔴 FRONTAL LOBE — The Action Controller
Role: The frontal lobe doesn't process visual content per se, but it drives where we look and what we do with what we see.
Key areas:
- Frontal Eye Fields (FEF, Area 8) — voluntary saccadic eye movements (looking toward a target)
- Prefrontal cortex — working memory for visual information (holding an image in mind), top-down attention control
- Premotor/SMA — receives dorsal stream input to execute visually-guided movements
Lesion Effects:
| Lesion | Defect |
|---|---|
| Frontal Eye Fields (unilateral) | Eyes deviate TOWARD the lesion (ipsilateral gaze deviation) in acute stroke — the intact FEF on the other side "pushes" eyes toward it; patient "looks at the lesion" |
| Prefrontal (DLPFC) | Impaired visual working memory — cannot hold or manipulate visual information in mind |
| Right prefrontal | Visual neglect (can contribute alongside parietal) |
| Frontal lobe broadly | Loss of top-down visual attention — cannot selectively attend to relevant visual stimuli; distractibility |
Summary Table — Lobe × Visual Role × Lesion Defect
| Lobe | Visual Role | Key Lesion Defect |
|---|---|---|
| Occipital | Primary reception + early processing (orientation, color, motion) | Hemianopia, cortical blindness, achromatopsia, akinetopsia |
| Parietal | Spatial location, visuomotor guidance ("WHERE") | Neglect, Bálint's syndrome, optic ataxia, simultanagnosia |
| Temporal | Object/face recognition, visual memory ("WHAT") | Prosopagnosia, visual agnosia, alexia |
| Frontal | Gaze control, visual attention, visually-guided action | Ipsilateral gaze deviation, loss of voluntary saccades, visual working memory loss |
So the elegance of the visual system is that the occipital lobe generates the raw image, temporal lobe identifies it, parietal lobe locates it in space, and frontal lobe acts on it. Lesion any node and a specific piece of the visual experience breaks down.
— Neuroscience: Exploring the Brain, 5th Ed. | Harrison's 22E | Adams & Victor's Neurology, 12th Ed. | Neuroanatomy Through Clinical Cases, 3rd Ed.
This is a shared conversation. Sign in to Orris to start your own chat.