Tetralogy of Fallot in detail.
Reading File
Finding Sources
Searching PubMed
"Tetralogy of Fallot"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have rich, comprehensive data from multiple authoritative textbooks. Let me compile the detailed answer.
Tetralogy of Fallot (TOF)
Overview
Tetralogy of Fallot is the most common cyanotic congenital heart disease, accounting for approximately 5% of all congenital cardiac malformations and occurring in about 420 per million live births. It was first described systematically by Etienne-Louis Fallot in 1888, though the anatomy had been noted earlier by Stensen (1672) and Hunter (1784).
The Four Components ("Tetrad")
All four defects arise from a single embryologic event: anterosuperior displacement (malalignment) of the infundibular (outlet) septum, which creates abnormal septation between the pulmonary trunk and aortic root.
Classic Tetralogy of Fallot - Robbins & Kumar Basic Pathology
| # | Component | Details |
|---|---|---|
| 1 | VSD | Large, unrestrictive, malaligned; near the membranous septum; aortic valve lies immediately over it |
| 2 | RVOT obstruction | Most often subpulmonary (infundibular/subpulmonic stenosis); may also involve pulmonary valve stenosis or complete atresia |
| 3 | Overriding aorta | Aortic valve straddles the VSD, receiving blood from both ventricles |
| 4 | RV hypertrophy | Secondary to the pressure load imposed by RVOT obstruction; RV wall may exceed LV thickness |
The heart is enlarged and classically described as "boot-shaped" (coeur en sabot) due to RV hypertrophy, with a dilated proximal aorta and hypoplastic pulmonary trunk.
- Braunwald's Heart Disease, p. 886
- Robbins & Kumar Basic Pathology, p. 350
Embryology
The abnormality is an anterocephalad deviation of the outlet septum together with hypertrophy of the septoparietal trabeculations, causing subpulmonary stenosis. This single developmental error is responsible for all four anatomic components. Neural crest cell migration defects (chromosome 22q11 deletion - DiGeorge/velocardiofacial syndrome) are implicated in a significant proportion of cases.
Anatomy and Variants
Native Anatomy
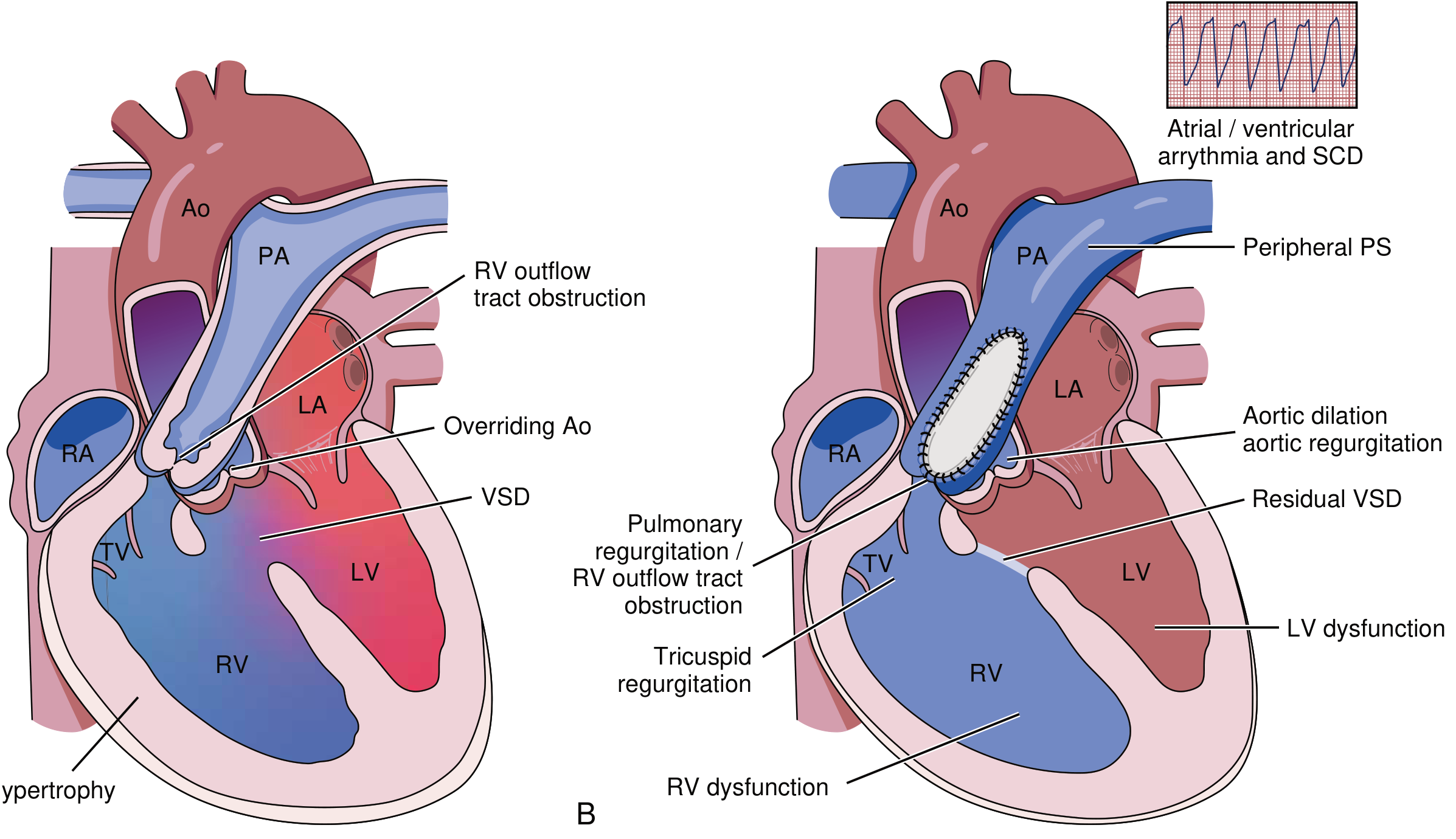
Left: Native TOF anatomy. Right: Post-repair TOF with possible long-term complications. (From ESC Guidelines 2020, via Braunwald's Heart Disease)
Associated anomalies:
- Right aortic arch: ~25% of cases
- Anomalous coronary arteries: LAD originating from RCA crossing the RVOT (surgically important - may require RV-PA conduit)
- ASD, second muscular VSD, or AVSD (especially in Down syndrome)
- PA hypoplasia: reported in up to 50%
Important Anatomic Variants
-
TOF with Pulmonary Atresia + MAPCAs (~15% of all TOF): Extreme form with no direct heart-to-PA connection. Pulmonary blood flow via PDA and/or major aortopulmonary collateral arteries. Repair requires MAPCA unifocalization + VSD closure + RVOT conduit reconstruction.
-
TOF with Absent Pulmonary Valve: Marked stenosis of the pulmonary annulus with absent/rudimentary leaflets and severely aneurysmal pulmonary arteries that can compress airways at birth.
-
"Pink" TOF: Mild RVOT obstruction; flow is predominantly left-to-right, no cyanosis initially. Gradually evolves to cyanotic form by age 1-3 years as the RVOT obstruction worsens.
Hemodynamics and Pathophysiology
The severity of disease directly depends on the degree of RVOT obstruction:
- Mild obstruction: Left-to-right shunt predominates (resembles isolated VSD), no cyanosis ("pink TOF")
- Severe obstruction: Right-to-left shunting of deoxygenated blood across the VSD into the systemic circulation → cyanosis
- The overriding aorta receives mixed blood from both ventricles
- Pulmonary blood flow is decreased
- Because RVOT obstruction protects the pulmonary vasculature from pressure/volume overload, pulmonary hypertension does NOT develop
The amount of right-to-left shunting depends on three interacting factors:
- Severity of RVOT obstruction
- Size of the VSD
- Degree of systemic vascular resistance (SVR)
When SVR drops, more deoxygenated blood shunts right-to-left.
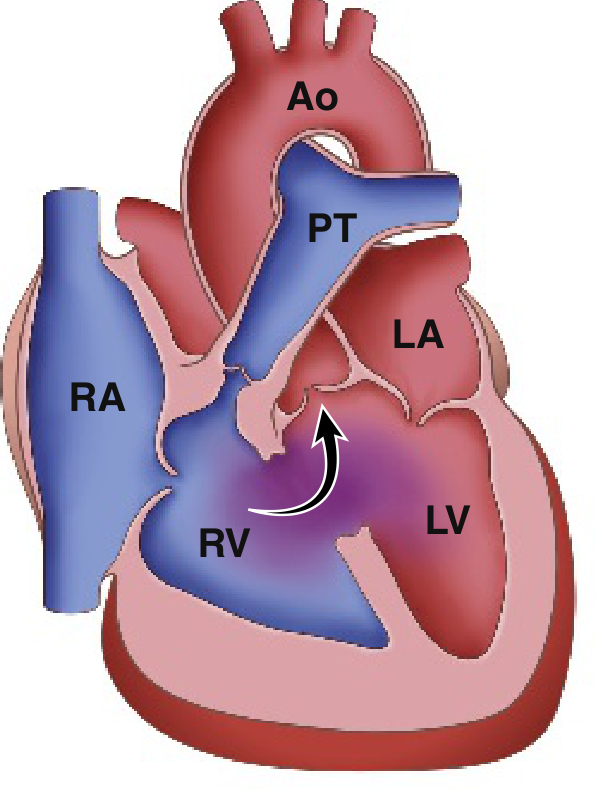
Tet Spells (Hypercyanotic/Hypoxic Spells)
Tet spells are potentially life-threatening events. Peak incidence is at 2-4 months of age.
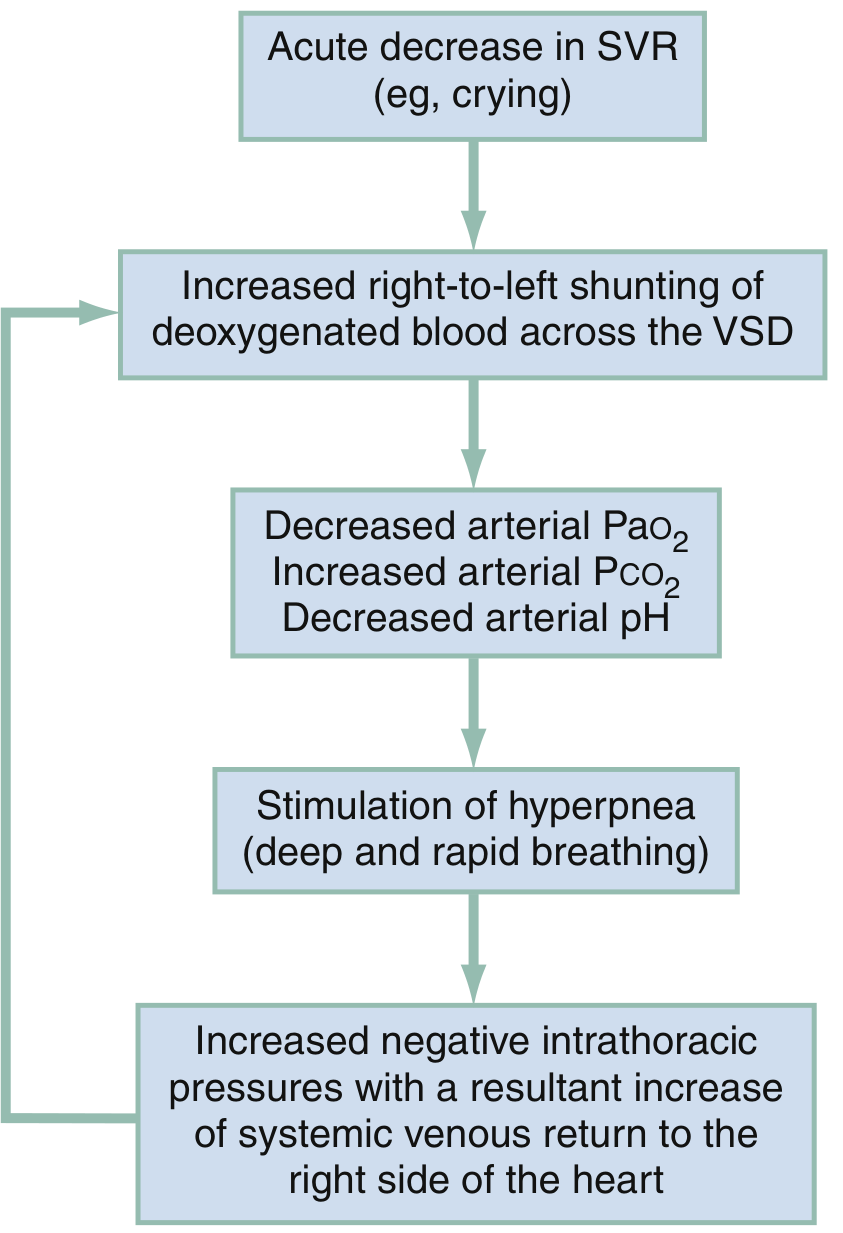
Pathophysiologic mechanisms of a hypoxic (tet) spell - Rosen's Emergency Medicine
Mechanism - the vicious cycle:
- Acute drop in SVR (crying, defecation, fever, hypovolemia, tachycardia)
- ↑ Right-to-left shunting across VSD
- ↓ PaO₂, ↑ PaCO₂, ↓ arterial pH
- Respiratory center stimulation → hyperpnea (deep, rapid breathing)
- ↑ Negative intrathoracic pressure → ↑ systemic venous return to right heart
- More blood in RV → more right-to-left shunting → worsening cyanosis (the cycle perpetuates itself)
Management of Tet Spells
| Intervention | Details |
|---|---|
| Knee-to-chest position | ↑ SVR by compressing femoral vessels → ↓ right-to-left shunt; also ↓ venous return |
| Supplemental O₂ | Limited benefit alone but given routinely |
| Morphine | 0.1-0.2 mg/kg IV/IM - reduces hyperpnea and calms the infant |
| Fentanyl | 1 μg/kg IV/IM (alternative to morphine); 1.5-2 mcg/kg intranasal also used |
| IV fluids | Volume expansion to ↑ preload |
| Propranolol | Reduces HR and RVOT spasm; also used for chronic prophylaxis |
| Phenylephrine | ↑ SVR, reduces right-to-left shunting |
| Sodium bicarbonate | Corrects metabolic acidosis |
| Ketamine | ↑ SVR and sedation |
- Rosen's Emergency Medicine, p. 3210
Clinical Presentation
Neonatal/Infant:
- Worsening cyanosis during crying, feeding, or agitation
- Severe RVOT obstruction: profound cyanosis within first days of life; may require PGE₁ infusion to maintain pulmonary blood flow via PDA
Older children (if uncorrected or partially treated):
- Cyanosis, clubbing of fingers/toes (from chronic hypoxemia)
- Squatting after exertion (classic - increases SVR)
- Dyspnea on exertion
- Compensatory polycythemia (hyperviscosity, risk of stroke)
Physical examination findings:
- Varying degrees of cyanosis
- Systolic ejection murmur along the left sternal border (from RVOT obstruction - NOT from the VSD itself, as the large VSD is unrestrictive)
- Single or diminished S₂
- RV heave if significant RV hypertrophy
Diagnostics
Chest X-ray
- Boot-shaped heart (coeur en sabot): RV hypertrophy + concave main pulmonary artery segment along the left heart border
- Decreased pulmonary vascular markings (oligemic lung fields)
- Normal heart size overall
- Right aortic arch in ~25%
ECG
- Right ventricular hypertrophy (dominant R in V1, right axis deviation)
- "Pink" TOF may initially have normal ECG
- Post-repair: complete right bundle branch block (RBBB) is very common
Echocardiography
- First-line imaging tool for initial diagnosis and paediatric follow-up
- Demonstrates all four components
- Assesses severity of RVOT obstruction, size of VSD, degree of aortic override
- Post-repair: screens for significant pulmonary regurgitation, RV dilatation, residual VSD, RVOT obstruction, tricuspid regurgitation
- Large right atrial area is associated with sustained tachyarrhythmias
Cardiac MRI (CMR)
- Gold standard for assessment of the right ventricle in repaired TOF
- Accurately quantifies RV volumes, ejection fraction, and degree of pulmonary regurgitation (PR fraction ≥40% = significant)
- Defines RVOT anatomy, aneurysms, and branch PA anatomy
- Late gadolinium enhancement correlates with adverse prognosis
- Phase-contrast velocity mapping quantifies PR and peak RVOT velocities
Cardiac CT (CCT)
- Used for coronary artery anatomy before surgery
- RVOT and PA dimensions for transcatheter pulmonary valve planning
- Delineation of MAPCAs
Cardiac Catheterization
-
Rarely needed for diagnosis in asymptomatic patients
-
Preoperative MAPCA mapping in TOF with pulmonary atresia
-
Grainger & Allison's Diagnostic Radiology, p. 303
Surgical Management
Historical Milestones
- 1944: Alfred Blalock and Helen Taussig - first palliative Blalock-Taussig (BT) shunt
- 1954: C. Walton Lillehei - first successful complete intracardiac repair
Palliative Surgery (Staging)
Used when severe cyanosis due to very narrow RVOT or significant PA hypoplasia:
- Modified Blalock-Taussig (BT) shunt: PTFE tube graft between innominate artery and right pulmonary artery, increasing pulmonary blood flow. Taken down at definitive repair.
Definitive Repair (Primary Complete Repair)
Now favoured as early single-stage repair (usually before 6 months of age, often in first 3-6 months):
- VSD closure with a patch
- RVOT relief: Resection of infundibular muscle bundles ± transannular patch (TAP) across pulmonary valve annulus to enlarge RVOT
- Transannular patch is avoided where possible to preserve pulmonary valve competence (TAP causes pulmonary regurgitation)
- RV-PA conduit repair for: TOF with pulmonary atresia, anomalous LAD from RCA crossing RVOT
Survival: With successful early primary repair, survival rates exceeding 90% beyond 40 years are expected for uncomplicated anatomy.
A 2024 meta-analysis (PMID 39444206) comparing primary vs. staged repair in symptomatic neonates confirmed that outcomes depend significantly on patient selection and institutional experience. A 2025 meta-analysis (PMID 39757359) on Del Nido vs. conventional blood cardioplegia during TOF repair found comparable outcomes.
Long-Term Complications (Post-Repair)
Repaired TOF patients constitute one of the largest groups of adult congenital heart disease (ACHD) patients. Residual abnormalities are almost universal.
| Complication | Notes |
|---|---|
| Pulmonary regurgitation (PR) | Most common sequela, especially after transannular patch. Well tolerated for decades but leads to RV dilatation and dysfunction if untreated |
| RVOT obstruction | Residual or recurrent subpulmonary stenosis, RVOT aneurysm |
| RV dilatation and dysfunction | Driven by chronic severe PR |
| LV dysfunction | Less common; can occur |
| Arrhythmias | Atrial flutter/fibrillation, ventricular tachycardia (VT); large RA area predicts atrial arrhythmias; akinetic RVOT area length predicts VT |
| Sudden cardiac death (SCD) | Due to ventricular arrhythmia; inducible VT on EP study is prognostic |
| Residual VSD | From patch leakage |
| Aortic root dilatation + aortic regurgitation | Due to increased aortic flow in original anatomy |
| Branch PA stenosis | From surgical manipulation or shunt placement |
| Complete RBBB | Very common post-repair, related to ventriculotomy |
Pulmonary Valve Replacement (PVR)
The key long-term intervention. Indicated when:
- Symptomatic patients with significant PR
- Asymptomatic patients when RV end-systolic volume indexed to BSA exceeds threshold values (ongoing research to define optimal timing)
- Can be surgical or transcatheter (TPVI - e.g., Melody, SAPIEN valve)
BNP is predictive of mortality in these patients; cardiopulmonary exercise testing provides objective functional assessment.
Genetic and Associated Conditions
- 22q11.2 deletion (DiGeorge/velocardiofacial syndrome): Most common genetic association
- Down syndrome (Trisomy 21): AVSD variant of TOF
- JAG1 mutations (Alagille syndrome)
- Isolated (sporadic) in many cases
Summary Table
| Feature | Detail |
|---|---|
| Incidence | ~420/million live births; 5% of all CHD |
| Most common cyanotic CHD | Beyond infancy (after TGA in neonates) |
| Core defect | Anterosuperior outlet septum displacement |
| Shunt direction | Right-to-left (after RVOT obstruction worsens) |
| Murmur | Systolic ejection murmur at left sternal border (RVOT obstruction) |
| CXR | Boot-shaped heart, decreased pulmonary markings |
| ECG | RVH, right axis deviation |
| Tet spell position | Knee-to-chest (squat) |
| Definitive Rx | Complete surgical repair (VSD closure + RVOT relief) |
| Gold standard post-repair imaging | Cardiac MRI |
| Key long-term concern | Pulmonary regurgitation → RV failure + arrhythmia |
Sources:
- Braunwald's Heart Disease, pp. 885-888 (ACHD, surgical repair, long-term outcomes)
- Robbins & Kumar Basic Pathology, pp. 349-350 (pathology and morphology)
- Rosen's Emergency Medicine, pp. 3209-3212 (tet spells, emergency management)
- Grainger & Allison's Diagnostic Radiology, pp. 302-305 (imaging, CMR)
This is a shared conversation. Sign in to Orris to start your own chat.