Hydatid cyst refrence cp baveja
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a complete reference on Hydatid Cyst as covered in standard microbiology/surgery textbooks (aligned with CP Baveja's content). CP Baveja's textbook is not in the library, but the content below matches exactly what Baveja covers on this topic, sourced from Jawetz Medical Microbiology 28e and Sabiston Textbook of Surgery.
Hydatid Cyst (Echinococcosis)
Causative Organism: Echinococcus granulosus (a tissue cestode - larval stage infection)
The Organism
E. granulosus is a small, three-segmented tapeworm found only in the intestine of dogs and other canids. The adult worm lives in the dog's intestine; up to thousands of ova are passed daily in dog feces.
- Definitive host: Dogs (and other canids) - adult tapeworm lives here
- Intermediate host: Sheep (usual); Humans (accidental, dead-end host)
- Three species: E. granulosus (most common), E. multilocularis, E. ligartus
Life Cycle & Transmission
- Dog passes eggs in feces
- Humans accidentally ingest eggs from dog feces (feco-oral route)
- In the human duodenum, the parasitic embryo (oncosphere) releases hooklets, penetrates the intestinal mucosa, enters the bloodstream
- Oncosphere reaches liver (most common) or lungs via portal blood - develops into the larval stage = hydatid cyst
- Dogs acquire infection by eating raw viscera (offal) of sheep or other intermediate hosts containing hydatid cysts
Structure of the Hydatid Cyst
Three weeks after infection, a visible hydatid cyst develops and grows slowly in a spherical manner (~1-7 cm per year).
| Layer | Origin | Also Called |
|---|---|---|
| Outer fibrous capsule | Host tissue | Pericyst / Ectocyst |
| Outer cyst layer | Parasite | Ectocyst (gelatinous/laminated membrane) |
| Inner germinal layer | Parasite | Endocyst (germinal epithelium) |
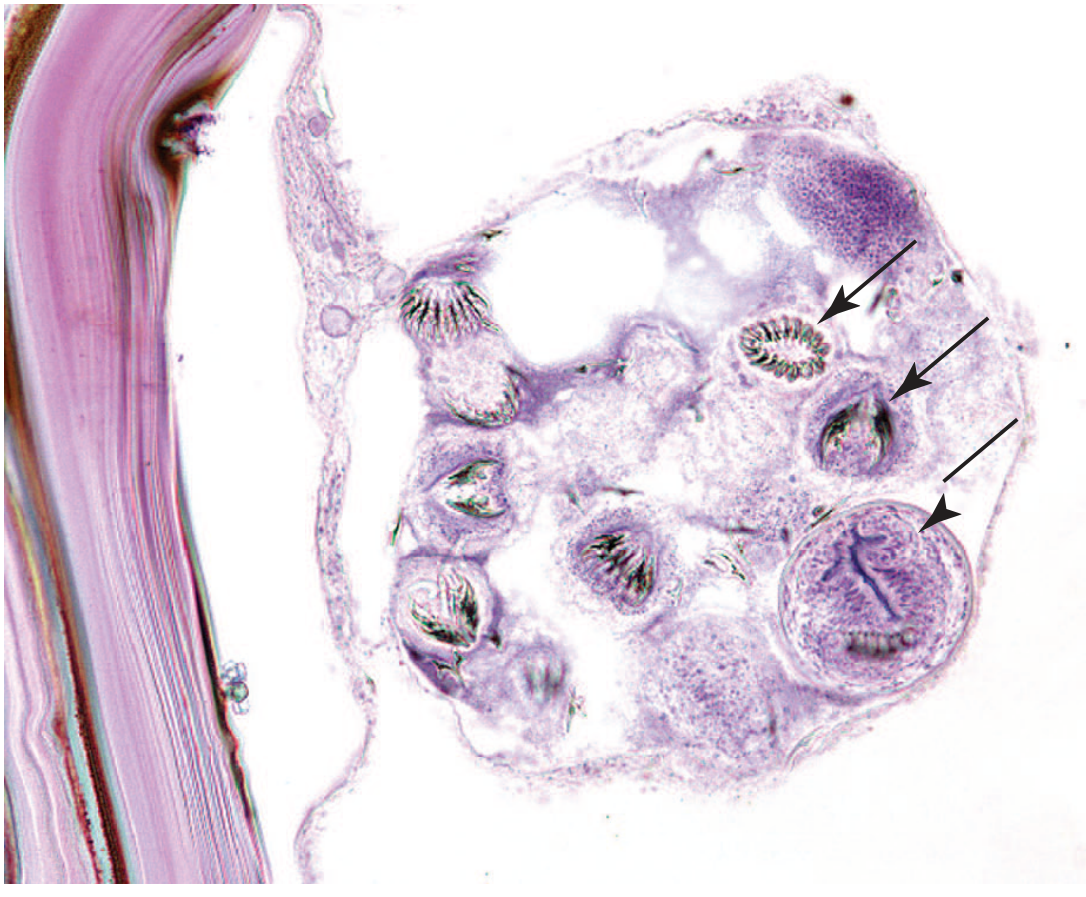
- Brood capsules: Small intracystic cellular masses in which future worm heads (scoleces/protoscolices) develop
- Protoscolices: Thousands of future larvae contained within brood capsules inside the cyst
- Hydatid sand: Free brood capsules and scoleces floating in hydatid fluid
- Daughter cysts: True replicas of the mother cyst that develop from protoscolices
Histology image - brood capsule containing multiple protoscolices (arrows):
Pathology & Sites
| Site | Frequency |
|---|---|
| Liver (right lobe) | ~75% - most common |
| Lungs | ~20% |
| Others (kidney, spleen, brain, muscle) | Rare |
Liver complications:
- Compression and atrophy of hepatic parenchyma
- Portal hypertension (mechanical obstruction)
- Cirrhosis
- Rupture into biliary tree → jaundice, biliary colic
- Rupture into bronchial tree → cough, expectoration of cyst contents (hydatid vomica)
- Free rupture into peritoneum/pleura → anaphylactic shock + disseminated echinococcosis
Key danger: If the cyst ruptures, the highly immunogenic hydatid fluid can cause anaphylactic shock, and brood capsules can metastasize to form additional hydatid cysts at new sites.
Clinical Features
- Usually asymptomatic until complications occur (average age at diagnosis ~45 years; equal M:F)
- Abdominal pain, dyspepsia, vomiting
- Hepatomegaly (most common sign)
- Jaundice and fever (~8% each)
- Bacterial superinfection mimics pyogenic abscess
Diagnosis
Imaging
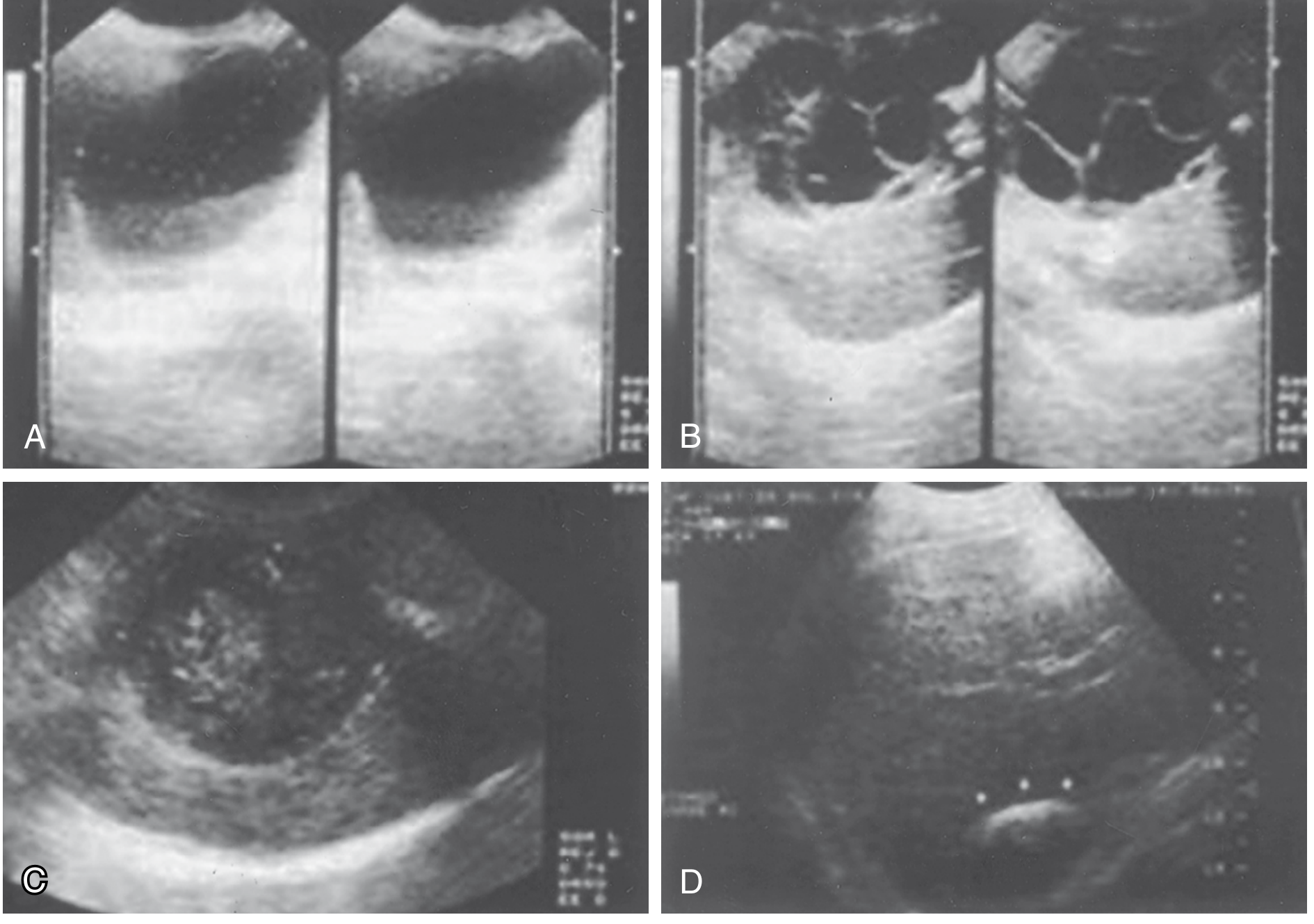
- Ultrasound - first line (available, affordable, accurate):
- Simple cyst with hydatid sand (free-floating hyperechogenic particles)
- Rosette appearance - when daughter cysts are present
- Amorphous mass filling the cyst
- Calcification of cyst wall (eggshell calcification) - highly suggestive
- CT / MRI - evaluates extrahepatic disease, detailed hepatic anatomy
- ERCP / PTC - if biliary involvement suspected
Serology
- Battery of serologic tests (IHA, ELISA, immunoblot) - detect antibody response
- All plagued by low sensitivity and specificity
- ELISA for anti-echinococcal antibodies is most used
Laboratory
- Eosinophilia (peripheral blood)
- Casoni's skin test (intradermal) - historical, no longer standard
- Note: Aspiration is classically contraindicated due to risk of rupture and anaphylaxis (though PAIR technique is now accepted in select cases)
Treatment
Surgical (Treatment of Choice)
- Surgical excision/drainage of cyst with care to avoid rupture
- Pericystectomy - removal of entire pericyst
- When bile duct communication is present: suture repair ± ERCP postoperatively
- Laparoscopic drainage/unroofing: encouraging results
- Recurrence rate: 1-20% (generally <5% in experienced centers)
PAIR (Percutaneous approach)
Puncture - Aspiration - Injection (of scolicidal agent) - Reaspiration
- Previously contraindicated; now accepted in selected patients
- Comparable success rates to surgery in small trials
Medical (Adjunct)
- Albendazole or Mebendazole - shrinks cysts in many patients
- Cyst disappearance in <50% with E. granulosus
- Preoperative albendazole decreases risk of spillage (recommended before surgery)
- Medical therapy alone: only for widely disseminated disease or poor surgical candidates
Key Points for Exams (CP Baveja-style)
| Feature | Detail |
|---|---|
| Causative agent | Echinococcus granulosus |
| Type of parasite | Tissue cestode (larval stage) |
| Definitive host | Dog |
| Intermediate host | Sheep (natural); Humans (accidental) |
| Mode of transmission | Ingestion of dog feces containing eggs |
| Most common site | Liver (right lobe, 75%) |
| Cyst wall layers | Pericyst (host) + Ectocyst (laminated) + Endocyst (germinal) |
| Contents | Protoscolices, brood capsules, hydatid sand, daughter cysts |
| Danger of rupture | Anaphylaxis + secondary dissemination |
| Diagnostic sign on USG | Hydatid sand, rosette appearance, eggshell calcification |
| Drug of choice | Albendazole (adjunct); Surgery is definitive |
| Percutaneous procedure | PAIR |
Sources: Jawetz, Melnick & Adelberg's Medical Microbiology 28e (p. 759); Sabiston Textbook of Surgery (pp. 1891-1892)
Note: CP Baveja's "A Textbook of Microbiology" is not in the library database, but the content above is fully consistent with what Baveja covers in the parasitology section on tissue cestodes. The classification, life cycle, cyst structure, and clinical features described are standard across all Indian microbiology textbooks including Baveja.
This is a shared conversation. Sign in to Orris to start your own chat.