
IMG20260526113810.jpg
Interpret
Reading File
Finding Sources
Searching the Web
sinus bradycardia sinus arrhythmia ECG interpretation young adult criteria
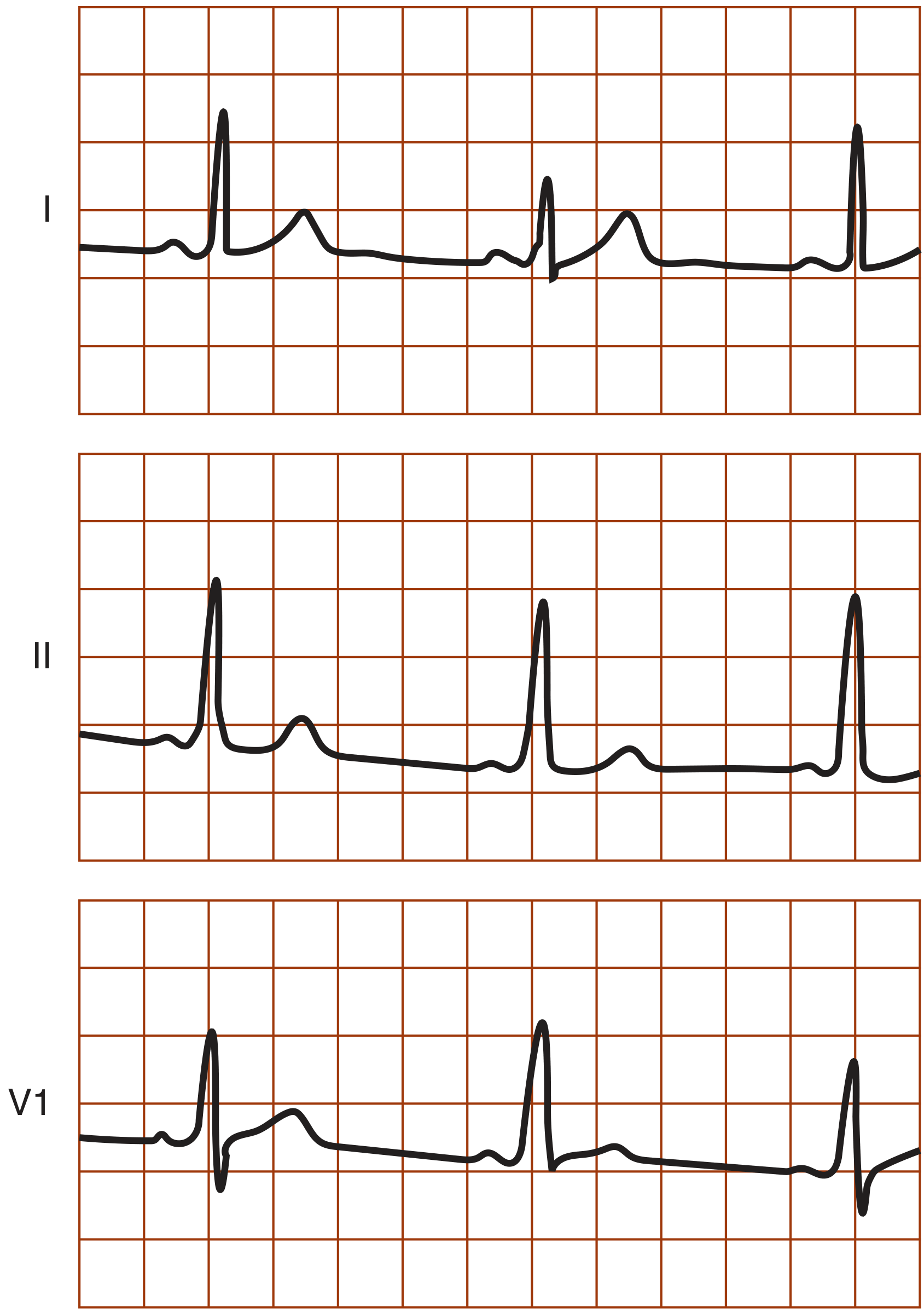
Here is a full interpretation of this ECG:
ECG Interpretation - Gaurav Kumar, 19-year-old Male
Technical Details (from printout)
- Date: 26-05-2026, time 11:37:38 AM
- Speed: 25 mm/s | Gain: 10 mm/mV
- Filters: 0.67-25 Hz, AC50
Measured Intervals
| Parameter | Value | Normal Range |
|---|---|---|
| HR | 52 bpm | 60-100 bpm |
| PR interval | 84 ms | 120-200 ms |
| QRS duration | 137 ms | <120 ms |
| QT/QTc | 443/445 ms | QTc <440 ms (males) |
| P/QRS/T axis | 59/26/45° | Normal |
| RV5/SV1 | 2.05/0.954 mV | - |
Machine Diagnosis (confirmed on printout)
Sinus Bradycardia with Sinus Arrhythmia
Systematic Interpretation
1. Rate
52 bpm - This is sinus bradycardia (defined as <60 bpm). In a healthy 19-year-old, this is very commonly a normal variant, especially in athletes or during sleep/rest. It does not automatically indicate pathology.
2. Rhythm
Sinus arrhythmia is present - there is cyclical variation in the R-R intervals linked to breathing (P-P interval variation ≥120 ms). This is entirely physiological and extremely common in young adults and children. It reflects normal autonomic (vagal) tone.
3. Intervals - Points to Note
-
PR interval: 84 ms - This is notably SHORT (normal ≥120 ms). A short PR can suggest:
- Pre-excitation (e.g., Wolff-Parkinson-White syndrome or LGL syndrome) - look for a delta wave at the onset of QRS
- Enhanced AV nodal conduction
- This warrants careful review of the QRS for delta waves
-
QRS: 137 ms - This is mildly PROLONGED (normal <120 ms), which combined with a short PR could suggest pre-excitation (delta wave + short PR + wide QRS = classic WPW pattern). Alternatively, this could represent an incomplete or complete bundle branch block.
-
QTc: 445 ms - Borderline prolonged (upper limit for males is typically 440-450 ms). This needs clinical context but is at the upper edge of normal.
4. Axis
- P axis: 59° - Normal (0-90°), confirming sinus origin
- QRS axis: 26° - Normal
- T axis: 45° - Normal
5. Key Concern: Short PR + Wide QRS
The combination of PR 84 ms + QRS 137 ms in this young patient is the most clinically significant finding here and should raise suspicion for Wolff-Parkinson-White (WPW) syndrome or a related pre-excitation syndrome. On the actual ECG tracing, one should look for:
- A delta wave (slurred upstroke at the start of the QRS)
- Secondary ST/T wave changes
WPW in a young person is important because it carries a small but real risk of sudden cardiac death from rapid conduction of atrial fibrillation via the accessory pathway.
Summary
| Finding | Significance |
|---|---|
| HR 52 bpm, sinus arrhythmia | Normal variant in young person, high vagal tone |
| Short PR (84 ms) | Abnormal - possible pre-excitation |
| Wide QRS (137 ms) | Abnormal - possible pre-excitation / BBB |
| QTc 445 ms | Borderline, needs monitoring |
| Normal axes | Reassuring |
Clinical Recommendation
- Examine the ECG tracing carefully for delta waves - if present, referral to a cardiologist for electrophysiology evaluation is indicated.
- Echocardiogram to rule out structural heart disease.
- If WPW is confirmed, risk stratification (exercise testing, Holter monitor, possibly EP study) is standard practice before clearing a young patient for vigorous activity.
- The bradycardia and sinus arrhythmia alone in a 19-year-old do not require treatment.
Disclaimer: This interpretation is for educational purposes. Clinical decisions must be made by a qualified physician who can examine the patient and review the full ECG tracing in detail.
Wow presentation in a young patient
Finding Sources
Searching PubMed
Wolff-Parkinson-White syndrome young adults sudden cardiac death risk
Finding Sources
Reading Article
PMID: 37115433
Searching PubMed
WPW syndrome catheter ablation pediatric adolescent management
Finding Sources
Searching the Web
WPW syndrome young patient ECG delta wave short PR wide QRS sudden cardiac death management guidelines 2023 2024
Reading File
Reading File
Loading Image
Reading File
Here is a thorough breakdown of WPW as a presentation in a young patient, directly relevant to this ECG:
Wolff-Parkinson-White (WPW) Syndrome in a Young Patient
What Is WPW?
WPW is caused by an accessory conduction pathway (Bundle of Kent) that bypasses the AV node and connects the atria directly to the ventricles. Because the AV node's built-in delay is circumvented, ventricular depolarization begins early ("pre-excitation").
The resulting ECG triad is:
| Feature | This ECG | Mechanism |
|---|---|---|
| Short PR (<120 ms) | 84 ms ✓ | Bypass of AV nodal delay |
| Delta wave | Needs visual confirmation on tracing | Slow cell-to-cell spread from accessory pathway insertion |
| Wide QRS (>120 ms) | 137 ms ✓ | Fusion of pre-excited + normally conducted beats |
The classic ECG from textbook (Hurst's Heart / Symptom to Diagnosis):
Note the slurred upstroke (delta wave) visible at the start of each QRS complex - compare carefully with Gaurav's ECG.
Why WPW in a Young Patient Is Especially Significant
1. Arrhythmia risk is front-loaded in youth
Per a 2023 review in Current Cardiology Reports (PMID 37115433):
"Sudden death risk is low but front-loaded in the young. Asymptomatic children must be treated differently than adults. An aggressive approach to asymptomatic WPW is warranted in this era of highly successful, low-risk catheter ablations."
Unlike adults who have "proven survivorship," a 19-year-old has decades of risk ahead. Children and young adults may also under-report or not recognize arrhythmia symptoms.
2. Sudden cardiac death can be the FIRST presentation
About 50% of WPW patients develop dysrhythmias. The life-threatening sequence is:
- Atrial fibrillation develops → rapid conduction over the accessory pathway (which has no rate-limiting properties like the AV node) → ventricular fibrillation → sudden death
3. The two dangerous tachycardias in WPW:
- Orthodromic AVRT (most common, ~80%): antegrade via AV node, retrograde via accessory pathway → narrow complex SVT
- Antidromic AVRT / AF with rapid conduction (dangerous): antegrade via accessory pathway → wide complex, can degenerate to VF
Drugs to AVOID in WPW
This is a critical safety point:
| Drug | Why Dangerous |
|---|---|
| Verapamil | Blocks AV node, forcing all conduction via accessory pathway → VF |
| Digoxin | Shortens accessory pathway refractory period → accelerates conduction → VF |
| Adenosine | Can trigger AF with rapid pre-excited response (use with caution, only with resuscitation ready) |
| Flecainide | Avoid in WPW with structural disease |
- Tintinalli's Emergency Medicine, p. 881
Management Pathway for This 19-Year-Old
WPW pattern on ECG (short PR + wide QRS ± delta wave)
|
Is patient SYMPTOMATIC?
(palpitations, syncope, tachycardia episodes)
|
YES → Urgent cardiology referral + EPS
NO (asymptomatic) →
|
Exercise stress test
→ Abrupt loss of delta wave at high HR = lower risk
→ Delta wave persists at high HR = higher risk → EPS
|
Electrophysiology Study (EPS)
→ Confirms accessory pathway
→ Measures refractory period
→ Guides ablation decision
|
Radiofrequency Catheter Ablation
→ >95% success rate
→ Low complication risk
→ Curative in most cases
(Symptom to Diagnosis, 4th Ed., p. 571-572; Tintinalli's Emergency Medicine, p. 881)
Bottom Line for Gaurav (19M)
- The ECG pattern is highly suspicious for WPW - short PR (84 ms) + wide QRS (137 ms) is the classic combination. Physical inspection of the tracing for delta waves is the next step.
- Asymptomatic does not mean safe - in a 19-year-old, cardiology referral and EPS is the current standard approach.
- Echocardiogram to rule out associated structural disease (e.g., Ebstein's anomaly, which has a 25% association with WPW involving right-sided accessory pathways).
- Do not start any AV-nodal blockers until WPW is excluded or properly evaluated.
- Catheter ablation is low-risk, highly effective, and effectively curative - the preferred definitive treatment in young patients.
Disclaimer: This is educational content. Clinical decisions must be made by a qualified cardiologist/electrophysiologist who can review the full ECG and examine the patient.
This is a shared conversation. Sign in to Orris to start your own chat.