Wrist drop , foot drop, and claw hand and peripheral nerve injuries for orthopaedic proff exam and clinical findings too
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive data from the textbooks. Let me compile the full answer.
Peripheral Nerve Injuries: Wrist Drop, Foot Drop, Claw Hand - Orthopaedic Prof Guide
Sources: S. Das Manual on Clinical Surgery 13th Ed | THIEME Atlas of General Anatomy & Musculoskeletal System | Miller's Review of Orthopaedics 9th Ed | Gray's Anatomy for Students
CLASSIFICATION OF NERVE INJURY (Seddon & Sunderland)
| Seddon | Sunderland | Injury | Prognosis |
|---|---|---|---|
| Neurapraxia | 1st degree | Demyelination only; focal conduction block | Resolves in 1-2 days (temporary) |
| Axonotmesis | 2nd degree | Axonal injury; endoneurium intact | Usually complete regeneration (weeks-months) |
| - | 3rd degree | Endoneurium injured | Regeneration incomplete |
| - | 4th degree | Perineurium injured | Neuroma-in-continuity; poor spontaneous recovery |
| Neurotmesis | 5th degree | Complete nerve transection | No spontaneous regeneration - surgery required |
Key point: Most important prognostic factor = patient age. Good prognosis: stretch injuries, clean wounds, direct surgical repair. Poor prognosis: crush/blast, infected/scarred wounds, delayed repair.
1. WRIST DROP (Drop Hand) - Radial Nerve Injury
Nerve: Radial Nerve (C5-C8)
Mechanism of Deformity
The radial nerve (via its posterior interosseous branch) supplies all extensors of the wrist. Injury = inability to extend the wrist at the wrist joint → Wrist drop (drop hand). Metacarpophalangeal extension is also lost. Note: Extension of the IP joints is done by the interossei through extensor expansions (supplied by ulnar nerve) - these are unaffected in radial nerve injury. This is a classic viva trap.
Causes by Level
Axilla (proximal) - "Crutch palsy":
- Improperly adjusted crutches
- Fracture-dislocation of upper end of humerus
- Features: Wrist drop + loss of triceps (cannot extend elbow) + full sensory loss
Radial Groove / Spiral Canal - "Saturday night palsy" / "Park bench palsy":
- Fracture of shaft of humerus (most classic for ortho exams)
- Sleeping with arm hanging over bench/chair
- Pressure at edge of operating table
- Inadvertent intramuscular injection
- Features: Wrist drop without triceps involvement (triceps branches exit before the groove) + sensory loss over first web space dorsum
Midlevel (lateral intermuscular septum / radial tunnel):
- Chronic compression
- Features: Wrist drop without triceps loss
Posterior Interosseous Nerve (PIN) injury:
- Fracture/dislocation of upper end of radius
- Features: Motor loss only (no wrist drop paradox - ECRB is spared), NO sensory loss
Clinical Findings (Motor)
- Unable to extend wrist
- Unable to extend MCPJs of fingers
- Brachioradialis test: Forearm in mid-prone position, flex elbow against resistance - muscle fails to stand out if radial nerve injured above its branching
Clinical Findings (Sensory)
- Sensory loss on the radial surface of the dorsum of the hand
- Extensor surface of thumb, index finger, and radial half of middle finger (up to PIP joint)
- Autonomous zone (exclusive territory): First dorsal web space (between thumb and index finger)
Brachioradialis Test (Level Determination)
Brachioradialis is supplied by the radial nerve before it divides into superficial and deep branches. Testing this muscle (forearm in mid-prone, flex elbow against resistance) determines the level of injury.
2. FOOT DROP - Common Peroneal (Lateral Popliteal) Nerve Injury
Nerve: Common Peroneal Nerve (L4, L5, S1)
Mechanism of Deformity
The common peroneal nerve supplies the extensor and peroneal (evertor) muscle groups of the leg. Injury = loss of dorsiflexion + eversion → Foot drop with talipes equinovarus deformity (foot plantarflexed and inverted).
Common Causes
- Fracture neck of fibula (most classic for ortho exams - nerve winds around the fibular neck)
- Prolonged squatting or crossed-leg sitting (pressure at fibular head)
- Plaster cast too tight at fibular head
- Knee dislocations (lateral aspect)
- Car bumper injury (classic trauma mechanism)
Deformity
- Equinovarus (foot drops and turns inward)
- Patient cannot dorsiflex or evert the foot
- High stepping (steppage) gait to clear the ground
Clinical Findings (Motor)
| Muscle | Test | Finding |
|---|---|---|
| Tibialis anterior | Dorsiflex foot against resistance | Absent |
| Extensor digitorum longus | Extend toes | Absent |
| Extensor hallucis longus | Extend big toe | Absent (often first affected) |
| Peroneus longus/brevis | Evert foot | Absent |
Clinical Findings (Sensory)
- Loss over anterior and lateral aspects of the leg
- Entire dorsum of the foot and toes (except the first web space between 1st and 2nd toes - supplied by deep peroneal nerve)
- Autonomous zone: First web space of dorsum of foot (deep peroneal branch)
Treatment (Ortho)
- Conservative: AFO (ankle-foot orthosis) - splint the foot in neutral
- Tendon transfer (if permanent): Transfer of PTT (posterior tibial tendon) through the interosseous membrane to the dorsal midfoot to restore dorsiflexion. Also requires TAL (tendoachilles lengthening).
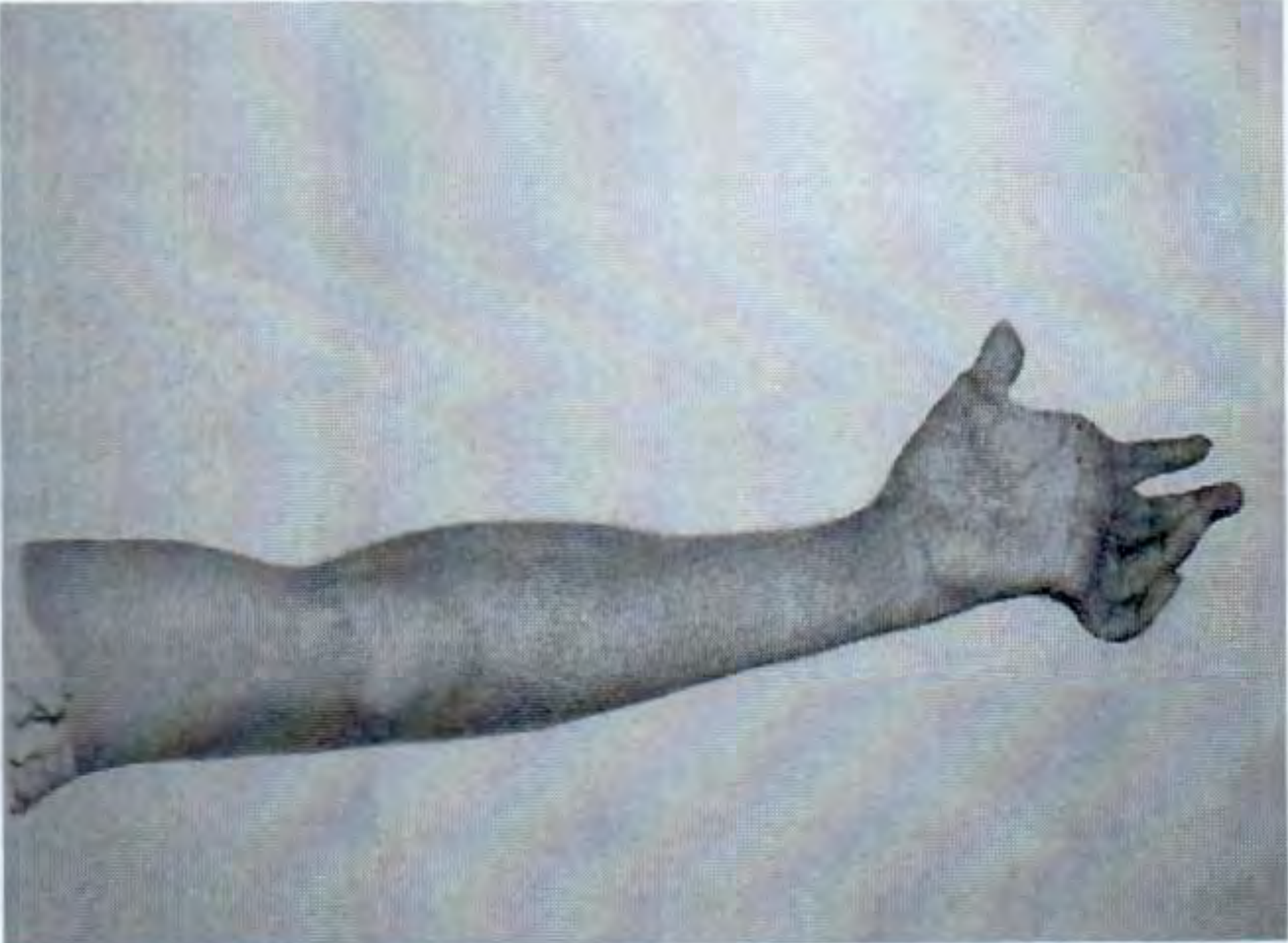
3. CLAW HAND (Main en Griffe) - Ulnar ± Median Nerve Injury
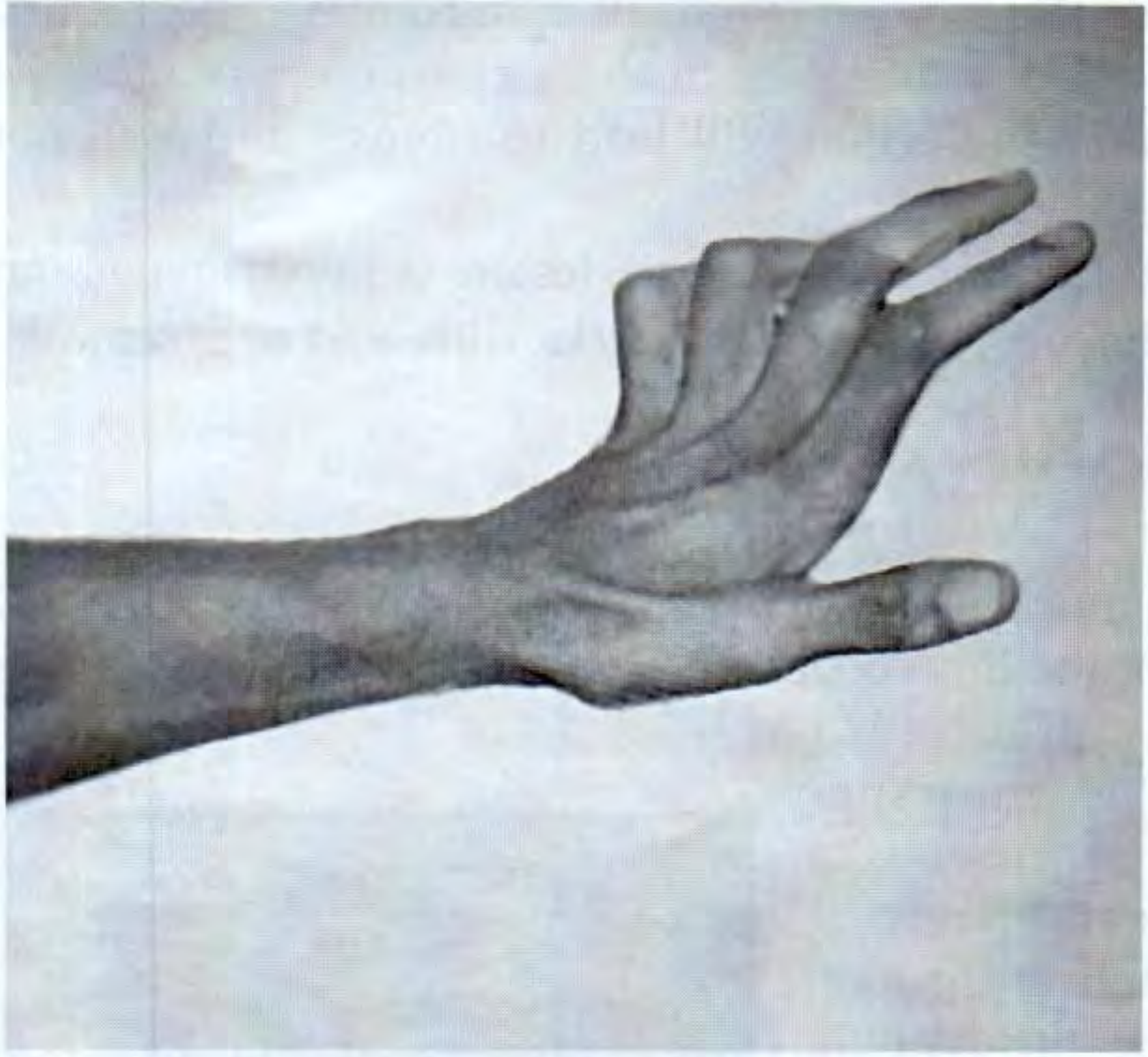
Claw hand deformity - ulnar nerve injury
Ulnar nerve sensory territory and clawing of ring/little fingers
Nerve: Ulnar Nerve (C8, T1) - primary; also Median Nerve (C6-T1)
Mechanism of Deformity
The interossei and lumbricals (supplied by ulnar nerve for 3rd and 4th lumbricals) perform:
- Flexion of MCPJs
- Extension of IPJs through extensor expansions
When they are paralyzed:
- Extensor digitorum (unopposed) hyperextends the MCPJs
- FDS and FDP (unopposed) flex the IPJs
- Result: Hyperextension at MCP + Flexion at PIP + DIP = Claw
Why is the claw worse for ring and little fingers?
- The 1st and 2nd lumbricals (for index and middle) are supplied by the median nerve and can partially compensate
- 3rd and 4th lumbricals (ring and little) are ulnar-supplied → these 2 fingers claw more = Ulnar Paradox: a more proximal lesion (at elbow) also paralyzes FDP to the ring and little fingers, which partially reduces the clawing. A distal wrist lesion produces a more severe claw.
Causes by Level
At the Elbow:
- Supracondylar fracture (recent injury or late tardy ulnar palsy from callus/cubitus valgus)
- Fracture medial epicondyle
- Cubital tunnel syndrome (compression between flexor carpi ulnaris heads)
- Sulcus ulnaris syndrome (chronic traction)
- Features: Claw + sensory loss + FCU paralysis (hand deviates radially on flexion) + medial half FDP paralysis (ring/little finger profundus lost)
At the Wrist:
- Lacerations, Guyon's canal (ulnar tunnel) compression
- Features: Claw + sensory loss (no FCU involvement)
Clinical Findings (Motor)
| Test | Muscle | Finding |
|---|---|---|
| Card test | Palmar interossei | Cannot hold card between fingers against pull |
| Finger abduction | Dorsal interossei | Cannot spread fingers against resistance |
| Froment's sign | Adductor pollicis | Thumb IP joint flexes when holding paper (FPL - median nerve - compensates for lost adductor pollicis) |
| FCU test | FCU (if elbow injury) | Hand deviates radially on wrist flexion |
| FDP test (ring/little) | Medial FDP (if elbow) | Cannot flex DIP of ring/little finger |
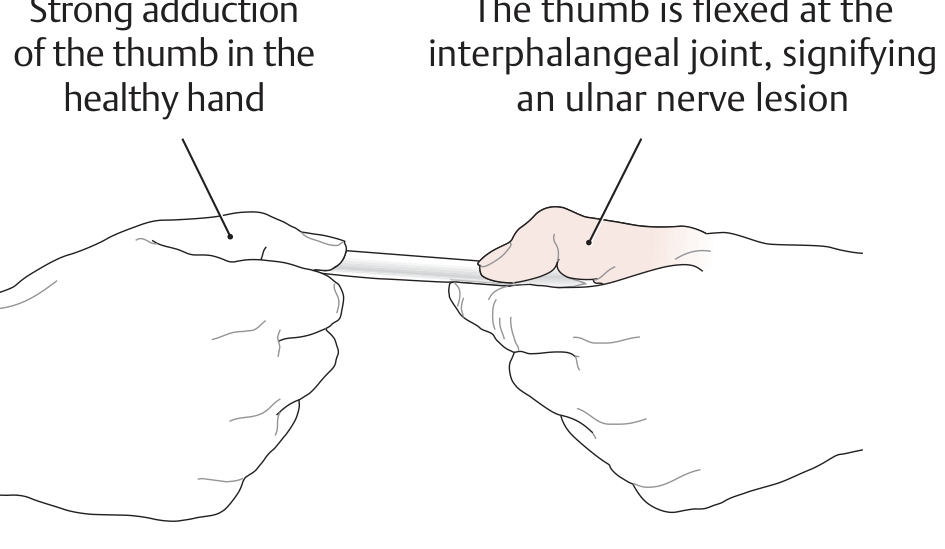
Froment's sign: thumb IP joint flexes on the affected side due to loss of adductor pollicis (compensated by FPL)
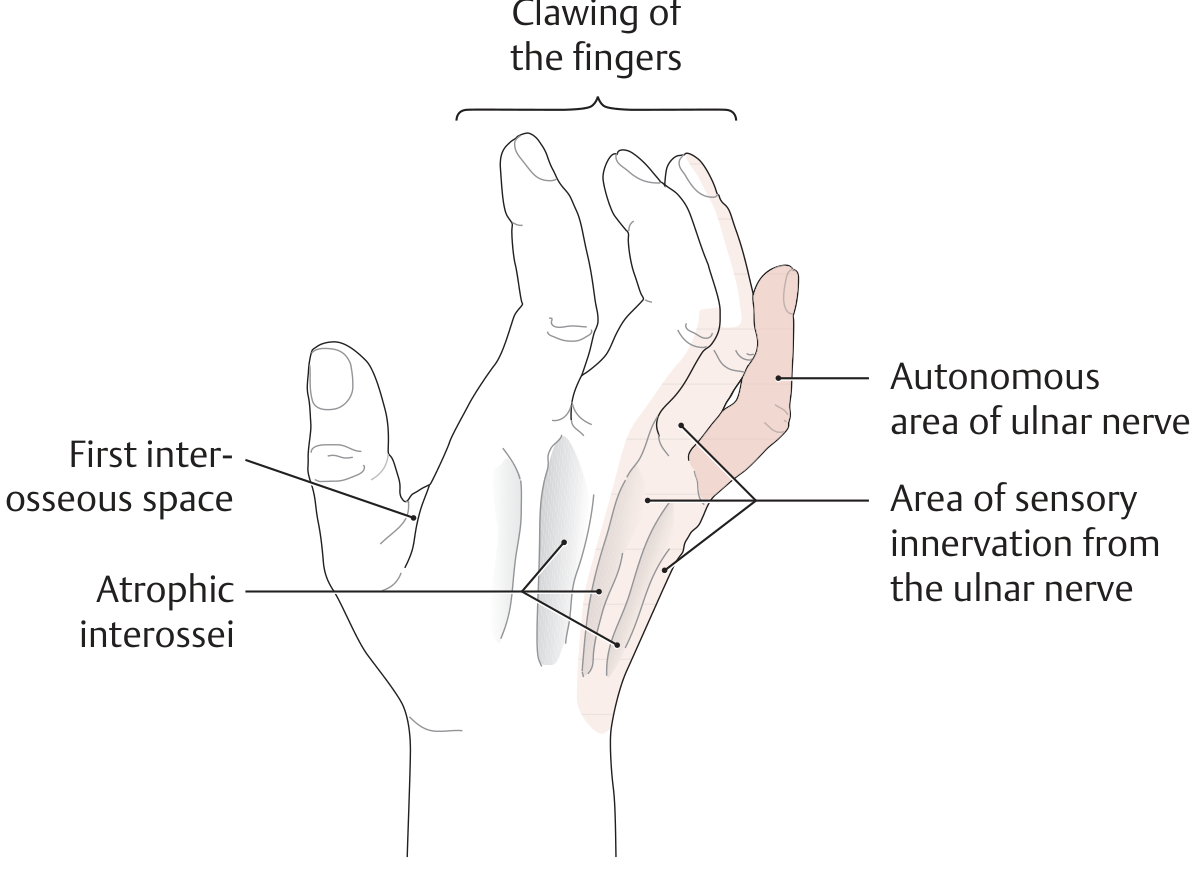
Clinical Findings (Sensory)
- Medial side of the hand
- Entire little finger (ring and little in some)
- Autonomous zone: Little finger (tip and medial border)
- Atrophy: Hypothenar eminence + interosseous spaces (first interosseous space most conspicuous)
4. OTHER IMPORTANT DEFORMITIES (for complete Prof exam)
Median Nerve Injury
Nerve root: C6, C7, C8, T1
At Elbow (above the elbow) - Supracondylar fracture:
- Ochsner's clasping test / Pointing index sign: When patient clasps hands, the index finger fails to flex (FDP lateral half paralyzed) - this is the "pointing index"
- FPL paralyzed: Cannot flex terminal phalanx of thumb
- FCR paralyzed: Hand deviates ulnar on wrist flexion
At Wrist (carpal tunnel level):
- Simian/Ape hand: Thenar muscles wasted; thumb comes to same plane as metacarpals; opposition lost
- Pen test (Abductor pollicis brevis): Lay hand flat, ask to touch pen held above palm - unable to do so
- Opponens pollicis: Cannot bring thumb tip to meet other fingertips
Sensory loss: Lateral 3.5 fingers + thenar eminence; autonomous zone = tip of index finger
Combined Ulnar + Median Nerve Injury
- Produces maximum claw hand (all interossei + all 4 lumbricals lost)
- Also seen in Klumpke's paralysis (lower brachial plexus C8-T1)
5. QUICK REVISION TABLE FOR VIVA
| Deformity | Nerve | Classic Cause | Autonomous Sensory Zone |
|---|---|---|---|
| Wrist drop | Radial | Humeral shaft # (radial groove) | 1st dorsal web space (hand) |
| Foot drop | Common peroneal | # neck of fibula | 1st web space (dorsum of foot) |
| Claw hand (ring+little) | Ulnar | Medial epicondyle # / Elbow fractures | Little finger |
| Ape hand + pointing index | Median | Supracondylar # / carpal tunnel | Index finger tip |
| Winging of scapula | Long thoracic of Bell | Mastectomy / stab | - |
| Policeman tip deformity | Brachial plexus (Erb-Duchenne, C5-C6) | Shoulder dystocia at birth | Lateral forearm |
| Claw foot | Medial popliteal (tibial) | Open wounds | Sole |
6. KEY CLINICAL EXAMINATION POINTS (Prof OSCE)
- Always look at the scar - the site of the wound tells you the likely nerve injured
- Attitude and deformity on inspection is the first clinical clue
- Test the "autonomous zone" for sensory loss - this is the most reliable area to confirm injury
- Extension of IP joints in wrist drop = NOT radial nerve recovery - it is the interossei (ulnar nerve) acting through the extensor expansion (common viva trap)
- Brachioradialis spared = injury is at/below lateral intermuscular septum (midlevel radial); if triceps lost = injury is above the radial groove (axilla)
- Ulnar paradox: Distal ulnar lesion (wrist) = worse claw than proximal (elbow), because FDP is still intact distally
- Froment's sign is the single best bedside test for adductor pollicis (ulnar nerve)
- Saturday night palsy = radial nerve compressed in the spiral groove - wrist drop without triceps loss, good prognosis
This is a shared conversation. Sign in to Orris to start your own chat.