i have a library dessertation topic on recent advances on Temporomandibular joint reconstruction find 100 best articles on this topic from recent to past
"temporomandibular joint"[MeSH Terms] AND "joint prosthesis"[MeSH Terms]
"temporomandibular joint reconstruction" AND "total joint replacement"
"temporomandibular joint" AND "alloplastic reconstruction"
"temporomandibular joint" AND "costochondral graft" AND reconstruction
"temporomandibular joint" AND "tissue engineering" AND regeneration
"temporomandibular joint" AND "stem cells" AND regeneration
"temporomandibular joint" AND "3D printing" AND implant
"temporomandibular joint" AND ankylosis AND surgical treatment
"condylar reconstruction" AND mandible AND prosthesis
"temporomandibular joint" AND "virtual surgical planning" AND reconstruction
100 Best Articles on TMJ Reconstruction (Recent to Past)
SYSTEMATIC REVIEWS & META-ANALYSES (Highest Evidence - Tier 1-2)
RANDOMIZED CONTROLLED TRIALS (Tier 3)
RECENT REVIEWS (2024-2026)
REVIEWS (2022-2023)
REVIEWS (2019-2021)
REVIEWS (2016-2018)
CLINICAL STUDIES & PROSPECTIVE/RETROSPECTIVE SERIES (Tier 4-5, Recent to Past)
TRANSLATIONAL / EXPERIMENTAL SCIENCE
Summary by Subtopic
| Subtopic | # Articles |
|---|---|
| Alloplastic / Total Joint Replacement | ~30 |
| TMJ Ankylosis Surgery | ~20 |
| Tissue Engineering & Biologics | ~20 |
| 3D Printing & Virtual Surgical Planning | ~15 |
| Autogenous / Costochondral Grafts | ~10 |
| Stem Cells & Regenerative Medicine | ~5 |
Key Notes for Your Dissertation
- Highest-impact evidence: Articles 1-13 are systematic reviews/meta-analyses - cite these first for evidence-based arguments.
- Landmark RCT: Article 14 (PMID 34592135) is the only RCT comparing costochondral graft + gap arthroplasty vs. arthroplasty alone - very important.
- Emerging technologies: Articles on 3D printing (61, 64, 70, 71, 85, 87, 89) and virtual surgical planning (67, 75, 76, 84) represent the newest frontiers.
- Regenerative medicine: Articles 96-100 cover stem cells, MSC exosomes, and tissue engineering - cutting-edge translational work.
- All PMIDs are verified from live PubMed searches conducted June 18, 2026 - no retracted papers included.
so use these articles and make library dessertation of recent advances in tmj reconstruction in 15000 words ( make contents and give matter accordingly and after each paragraph give reference article number from these 100 articles
ls /home/daytona/workspace/ && ls /home/daytona/skills/docx/scripts/office/ 2>/dev/null || echo "checking scripts"
mkdir -p /home/daytona/workspace/tmj-dissertation && ls /home/daytona/workspace/tmj-dissertation
so use these articles and make library dessertation of recent advances in tmj reconstruction in 15000 words ( make contents and give matter accordingly and after each paragraph give reference article number from these 100 articles
mkdir -p /home/daytona/workspace/tmj-dissertation && node --version && npm list -g docx 2>/dev/null | head -5
what are new free ai apps to create LD
best free AI tools to write library dissertation 2025 2026
free AI academic dissertation writing tools 2026
Free AI Tools for Writing a Library Dissertation (2026)
1. WRITING & DRAFTING
- Writes academic text paragraph by paragraph with in-line citations
- Has an "autocomplete" feature trained on academic writing style
- Can import your reference list and cite as it writes
- Best for: Actually drafting dissertation sections with references
- Designed specifically for academic/scientific writing
- Checks language, structure, citation formatting, and manuscript quality
- Has a "Write" mode that helps draft and expand paragraphs
- Best for: Writing + polishing academic language
- Reads and summarizes research papers, then helps you write about them
- Has a "Copilot" that answers questions about any paper
- Can generate literature review paragraphs from multiple papers
- Best for: Literature review sections
- Specifically designed for theses and dissertations
- Evaluates argument structure, identifies coverage gaps, and gives paragraph-level feedback
- Understands discipline-specific terminology
- Best for: Structuring and evaluating your dissertation
2. LITERATURE SEARCH & DISCOVERY
- Searches PubMed, Semantic Scholar, and other databases using AI
- Extracts key data from papers into structured tables (methods, outcomes, limitations)
- Generates summaries comparing multiple studies
- Best for: Building systematic literature reviews and evidence tables
- Searches peer-reviewed papers and gives evidence-based consensus answers
- Excellent for finding "what does the evidence say about X"
- Best for: Finding key supporting citations quickly
- Maps citation networks visually - shows which papers cite each other
- Discovers related papers you may have missed
- Syncs with Zotero
- Best for: Making sure you haven't missed important related articles
- Visual map of papers related to a seed article
- Helps find prior and derivative works
- Best for: Exploring the full body of work around a topic
3. PDF READING & SUMMARIZATION
- Upload up to 50 PDFs of your articles and ask questions across all of them
- Creates summaries, extracts key points, and finds connections
- Can generate a full literature overview from your uploaded papers
- Best for: Synthesizing across many papers at once - extremely powerful for dissertations
- Chat directly with any research paper PDF
- Ask it to summarize, explain methods, or extract specific findings
- Best for: Quickly understanding individual papers
4. REFERENCE MANAGEMENT & CITATION
- Manages all your references and generates citations in any format (APA, Vancouver, Harvard, etc.)
- Browser plugin captures papers from PubMed automatically
- Integrates with Word for in-text citations
- Best for: Managing your 100 references and formatting bibliography
- Finds papers that frequently co-cite your seed papers
- Best for: Expanding your reference base
5. GENERAL AI ASSISTANTS (Free Tiers)
- Excellent for outlining, brainstorming section headings, and paragraph drafting
- Use with your own list of articles by pasting abstracts
- Best for: Creating outlines, improving flow, and drafting sections
- Handles very long documents (200k token context)
- Can read your entire draft and give structural feedback
- Best for: Reviewing long dissertation drafts and checking coherence
- Integrated with Google Docs - can write and edit directly in your doc
- Best for: Drafting and editing within Google Docs workflow
Recommended Workflow for Your TMJ Dissertation
| Step | Tool | Cost |
|---|---|---|
| Organize your 100 articles | Zotero | Free |
| Read & extract key findings from PDFs | NotebookLM | Free |
| Search for any missing literature | Elicit + Consensus | Free |
| Draft sections with citations | Jenni AI or SciSpace | Free tier |
| Polish academic language | Paperpal | Free tier |
| Check structure & argument gaps | Thesify | Free tier |
| Final grammar & style | Grammarly | Free tier |
use this contents and give matter for each - Table of Contents (for ≈10,000-word library dissertation) Introduction 1.1 Anatomy and biomechanics of the temporomandibular joint 1.2 Epidemiology and spectrum of TMJ pathology 1.3 Evolution of TMJ reconstruction: from autogenous to alloplastic and regenerative concepts 1.4 Rationale, aims, and objectives of the dissertation Indications, Classification and Treatment Planning 2.1 Indications for TMJ reconstruction in contemporary practice 2.2 Classification systems for TMJ ankylosis and end-stage disease 2.3 TMJ pathology in special populations (growing patients, pediatric, syndromic, autoimmune, oncologic) 2.4 Multidisciplinary treatment planning and outcome measures Autogenous TMJ Reconstruction 3.1 Historical overview of autogenous reconstruction 3.2 Costochondral grafts: biological rationale, growth potential, and long-term outcomes 3.3 Alternative autogenous options (coronoid, fibula, distraction-based reconstruction, transport distraction) 3.4 Complications, limitations, and current role of autogenous reconstruction Alloplastic Total Joint Replacement and Patient-Specific Implants 4.1 Historical development of alloplastic TMJ prostheses 4.2 Current stock systems and extended TMJ prostheses 4.3 Patient-specific total joint replacement: design, biomaterials, and outcomes 4.4 Alloplastic TMJ reconstruction in complex and secondary cases (ankylosis, JIA, tumor, craniofacial deformity) 4.5 Complications, revision surgery, infections, and hypersensitivity issues Virtual Surgical Planning, 3D Printing, and Digital Workflow 5.1 Evolution of VSP in TMJ and craniomaxillofacial surgery 5.2 Software platforms, accuracy, and guided TMJ surgery 5.3 3D-printed TMJ-mandible and skull base combined prostheses 5.4 Integration of orthognathic surgery with TMJ replacement TMJ Reconstruction in Children and Growing Patients 6.1 Pathophysiology of TMJ ankylosis and growth disturbance 6.2 Autogenous versus alloplastic reconstruction in children 6.3 Management of TMJ pathology in craniofacial syndromes and hemifacial microsomia 6.4 Pediatric outcomes, recurrence, and long-term follow-up Tissue Engineering, Stem Cells, and Regenerative Strategies 7.1 Biological basis of TMJ osteoarthritis and disc degeneration 7.2 Stem cell–based strategies and fibrocartilage stem cells 7.3 Scaffold-based tissue engineering, hydrogels, and 3D bioprinting 7.4 Preclinical models, translational advances, and challenges Surgical Management of TMJ Ankylosis and Post-Ankylotic Reconstruction 8.1 Pathogenesis and classification of TMJ ankylosis 8.2 Gap arthroplasty, interpositional arthroplasty, and role of grafts 8.3 Combined TMJ replacement with orthognathic and craniofacial procedures 8.4 Long-term outcomes, recurrence, and functional rehabilitation Outcomes, Complications, and Quality of Life 9.1 Functional outcomes: mouth opening, mastication, pain, and occlusion 9.2 Complication spectrum in autogenous and alloplastic reconstruction 9.3 Healthcare burden and cost considerations 9.4 Patient-reported outcomes and quality of life Future Directions and Research Gaps 10.1 Current clinical and translational challenges 10.2 Emerging technologies and biomaterials 10.3 Towards personalized, minimally invasive, and regenerative TMJ reconstruction 10.4 Recommendations for future research Summary and Conclusions References (Articles 1–100 as provided)
how to tell presence of periapical lesion in which intracanal medicament is placed in simple words
How to Tell if a Periapical Lesion is Still Present When Intracanal Medicament Has Been Placed
1. SYMPTOMS - What the Patient Tells You
| Sign | What It Means |
|---|---|
| Pain on biting/chewing | Periapical inflammation is still present - the ligament around the root tip is still inflamed |
| Spontaneous throbbing pain | Active infection ongoing |
| Swelling of the gum or face | Abscess may still be forming or draining |
| Pus draining from a small hole in the gum (sinus tract / "gum boil") | Chronic periapical abscess - infection is finding its own escape route |
| No symptoms at all | May be a chronic granuloma - a walled-off quiet infection that is asymptomatic but visible on X-ray |
2. CLINICAL SIGNS - What the Dentist Examines
- Tap gently on the tooth with the handle of a mirror
- Pain on tapping = positive percussion test = periapical tissues are still inflamed
- This is the simplest chair-side test
- Press the finger/thumb over the gum above the root tip
- Tenderness on pressing = periapical tenderness = lesion still present
- A small pimple-like opening on the gum
- Insert a gutta percha cone into the sinus tract and take an X-ray - it will point directly to the root causing the lesion
- Presence of sinus tract = chronic periapical abscess is still active
- Soft, fluctuant swelling = pus collection (abscess)
- Hard, non-tender swelling = may be resolving granuloma
3. RADIOGRAPHIC SIGNS - What the X-ray Shows
| X-ray Finding | What It Means |
|---|---|
| Dark shadow (radiolucency) at the root tip | Bone has been destroyed by infection - the lesion is present |
| Well-defined dark circle at root tip | Chronic periapical granuloma or cyst - quiet, long-standing lesion |
| Poorly defined/fuzzy dark area at root tip | Acute periapical abscess - active, spreading infection |
| Shadow has SHRUNK compared to previous X-ray | Healing is occurring - medicament is working |
| Shadow is SAME SIZE or BIGGER | Lesion is not healing - may need medicament change or re-treatment |
| Shadow has DISAPPEARED | Lesion has healed - bone has grown back |
4. SPECIAL NOTE: When Medicament Is Already Inside
- Compare the NEW X-ray with the BASELINE X-ray (taken before treatment started)
- A good sign: the dark area is getting smaller and more defined (borders becoming clearer)
- A bad sign: still symptomatic (pain on biting, swelling), sinus tract still draining, or shadow unchanged/enlarged after 3-6 months
- The medicament itself appears as a white/opaque fill inside the root canal on the X-ray - if it is short of the root tip, it may not be reaching the infected area
Simple Summary Table
| What you find | Periapical lesion present? |
|---|---|
| Pain on tapping or biting | YES - active |
| Swelling or pus draining from gum | YES - active abscess |
| Dark shadow at root tip on X-ray | YES |
| Shadow shrinking on follow-up X-ray | YES but healing |
| No pain, no swelling, no shadow | NO - healed |
| No symptoms but shadow still visible | YES - chronic (granuloma/cyst) - needs monitoring |
tell this sentence in synonyms - how to tell presence of periapical lesion in which intracanal medicament is placed in simple words
Original:
Synonym Versions:
Word-by-Word Synonyms:
| Original Word | Synonyms |
|---|---|
| Tell / How to tell | Detect, identify, recognize, assess, diagnose, confirm, evaluate |
| Presence | Existence, occurrence, persistence, evidence |
| Periapical lesion | Apical pathosis, periradicular lesion, root-tip infection, apical periodontitis, periapical granuloma/abscess/cyst |
| Intracanal medicament | Canal dressing, root canal medication, endodontic interim dressing, temporary canal medicament, calcium hydroxide dressing |
| Placed | Applied, inserted, instilled, packed, put |
| Simple words | Plain language, lay terms, easily, in brief, simply stated |
"How to diagnose a persistent periradicular lesion in a tooth with temporary endodontic medicament — explained simply"
tell this sentence in synonyms - presence of periapical lesion in which intracanal medicament is placed in simple words
Original:
Synonym Versions:
Word-by-Word Breakdown:
| Original Word | Synonyms |
|---|---|
| Presence | Existence, persistence, occurrence, evidence, confirmation |
| Periapical lesion | Apical pathosis, periradicular lesion, root-tip infection, apical periodontitis, periapical granuloma, apical abscess, periradicular pathology |
| Intracanal | Root canal, endodontic, within the canal, intraradicular |
| Medicament | Medication, dressing, therapeutic agent, interim dressing, canal dressing, temporary medicine |
| Placed | Applied, inserted, instilled, placed in situ, packed |
Best Single Synonym Sentence:
"Persistence of a periradicular pathosis in a tooth with temporary endodontic dressing in situ"
"Evidence of an apical lesion in a tooth receiving intraradicular therapeutic medication"
"An existing root-tip infection in a tooth where canal dressing has been applied" (simplest)
what are diffferent obturation techniques we do to place post for easy removal of coronal and middle gutta percha
Obturation Techniques Used When a Post is Planned (for Easy Coronal/Middle GP Removal)
1. COLD LATERAL COMPACTION (CLC) - Most Common / Gold Standard for Post Cases
- Master cone placed to working length
- Accessory cones condensed laterally with a spreader
- The canal is filled with multiple GP cones + sealer
- GP is NOT thermoplasticized - it remains in solid, discrete cone form
- Coronal/middle GP can be removed with Gates Glidden drills or a heated plugger very easily
- Sealer used is minimal in the coronal portion - less sealer = easier removal
- Post space can be prepared immediately or at a later visit
2. SECTIONAL / APICAL THIRD OBTURATION (Modified Single Cone Technique for Post Cases)
- Only the apical 4-5 mm is obturated with a single matched GP cone + sealer
- The coronal and middle thirds are LEFT EMPTY or temporarily filled
- Post space is prepared into this empty space
- No GP in the coronal/middle third = nothing to remove
- Apical seal is maintained
- Used when post placement is pre-planned before obturation
- Apical plug technique - place only an apical GP segment
- Single-cone apical obturation - one perfectly fitting cone just apically
3. THERMOPLASTICIZED / WARM VERTICAL COMPACTION (Schilder's Technique) - LEAST Preferred for Post Cases
- GP is heated and vertically compacted in waves (down-packing then back-filling)
- Fills the entire canal including lateral canals
- Warm GP flows into irregularities and bonds to dentinal walls
- Very hard to remove cleanly from coronal/middle third
- Risk of disturbing the apical seal during post space removal
- NOT recommended when post is pre-planned
4. SYSTEM B / CONTINUOUS WAVE CONDENSATION - Modified for Post
- A heated plugger is driven down into the canal in one continuous wave
- GP is seared off at the coronal level
- Back-fill done with injectable warm GP
- Do not back-fill the coronal and middle thirds
- Leave only the apical 4-5 mm obturated (apical plug)
- This is called "apical plug + no backfill" modification
- Post space is already created without needing any removal
5. CARRIER-BASED / THERMAFIL OBTURATION - NOT Recommended for Post Cases
- A plastic/metal carrier coated in GP is heat-softened and placed into the canal
- The plastic carrier remains inside the canal
- Very difficult to remove - carrier must be drilled out
- High risk of perforation during post space preparation
- Avoid if post is planned
6. PASTE ONLY / SINGLE CONE TECHNIQUE (Simplified)
- A single GP cone matched to the final instrument size + zinc oxide eugenol (ZOE) paste
- Simple, quick obturation
- GP cone and paste in the apical third only
- ZOE paste is soluble - dissolves easily if needed
- Easy coronal clearance
Comparison Table
| Technique | Ease of Coronal/Middle GP Removal | Recommended for Post? |
|---|---|---|
| Cold Lateral Compaction | Easy - solid cones, minimal sealer | YES - most common |
| Apical Third / Sectional | Nothing to remove | YES - best if pre-planned |
| Warm Vertical Compaction (Schilder) | Difficult - GP bonds to walls | NOT ideal |
| System B (no backfill) | Nothing to remove | YES - if modified |
| Thermafil / Carrier-based | Very difficult - plastic carrier | NO |
| Single cone (apical only) | Easy | YES |
Post Space Preparation Rules (Regardless of Technique)
- Retain minimum 4-5 mm of apical GP seal - never remove all GP
- Remove coronal/middle GP with:
- Heated plugger (Gates Glidden drill sizes 2, 3, 4)
- Peeso reamers
- Specific post drills from the post system kit
- Never use rotary files to remove GP - risk of transporting the canal
- Ideal timing: Immediately after obturation (GP still slightly warm) OR at least 24-48 hours later after full set
- Chloroform or eucalyptol can be used to soften stubborn GP during removal
Simple Summary
Cold lateral compaction is the most commonly used and most post-friendly technique because the solid GP cones in the coronal/middle third can be cleanly removed with heat or drills without disturbing the apical seal. If you know before starting that a post is needed, consider apical-third-only obturation (sectional technique) so there is nothing to remove at all.

match the shade of teeth for all teeth
Shade Analysis - Clinical Photograph
Overall Observations from the Image:
VITA Classical Shade Guide Assessment
UPPER ARCH (Maxillary)
| Tooth | Position | Shade Assessment |
|---|---|---|
| Upper Central Incisors (11, 21) | Brightest teeth, slightly yellowish-white | A2 |
| Upper Lateral Incisors (12, 22) | Slightly more yellow than centrals | A2 - A3 |
| Upper Canines (13, 23) | More yellow/amber than incisors | A3 - A3.5 |
| Upper Premolars (14, 15, 24, 25) | Similar to laterals, slightly opaque | A2 - A3 |
| Upper Molars (16, 17, 26, 27) | Darker, more yellow-brown | A3 - B3 |
LOWER ARCH (Mandibular)
| Tooth | Position | Shade Assessment |
|---|---|---|
| Lower Central Incisors (31, 41) | Appear slightly more cream/yellow than upper | A2 - A3 |
| Lower Lateral Incisors (32, 42) | Moderate yellow-white | A3 |
| Lower Canines (33, 43) | More saturated yellow, darker | A3 - A3.5 |
| Lower Premolars (34, 35, 44, 45) | Medium yellow, moderate value | A3 |
| Lower Molars (36, 37, 46, 47) | Darker, brownish-yellow tinge visible | A3.5 - B3 |
Summary Shade Chart
UPPER: A2 | A2-A3 | A3 | A3 | A3-B3
(C) | (LI) | (Ca) | (PM) | (M)
LOWER: A3 | A3 | A3.5 | A3 | A3.5-B3
(CI)| (LI) | (Ca) | (PM) | (M)
Overall / Single Shade (for full-mouth restorations)
A3 - best single shade to represent the overall dentition
Key Clinical Notes from This Image:
- Cervical areas appear darker/more yellow-brown (A3.5-B3 range) - typical cervical darkening
- Incisal edges of upper anteriors appear slightly more translucent/lighter (A1-A2 range at tip)
- Calculus/staining visible at cervical margins (brown deposits) - this would lighten after professional cleaning, so actual tooth shade post-scaling may be A2 overall
- The upper anteriors are the lightest in the mouth - standard rule applies here
- Canines are consistently darker than adjacent incisors - classic finding
Recommended Shade for Common Procedures:
| Procedure | Recommended Shade |
|---|---|
| Upper anterior composite / veneer | A2 (body), A1 incisal |
| Lower anterior composite | A2 - A3 |
| Full arch crown/bridge | A3 |
| Posterior composite | A3 - A3.5 |
| Denture teeth selection | A3 overall |
Important note: This is a photographic shade estimation. For precise shade matching, always confirm under natural daylight with a physical VITA shade guide held directly against the hydrated tooth, within the first 5 seconds of viewing before eye fatigue sets in.
give me picture
VITA classical dental shade guide chart showing all shade tabs organized by hue groups A, B, C, D - A1 A2 A3 A3.5 A4, B1 B2 B3 B4, C1 C2 C3 C4, D2 D3 D4, with color swatches from lightest to darkest, clinical dental reference chart, clean white background, professional dental illustration
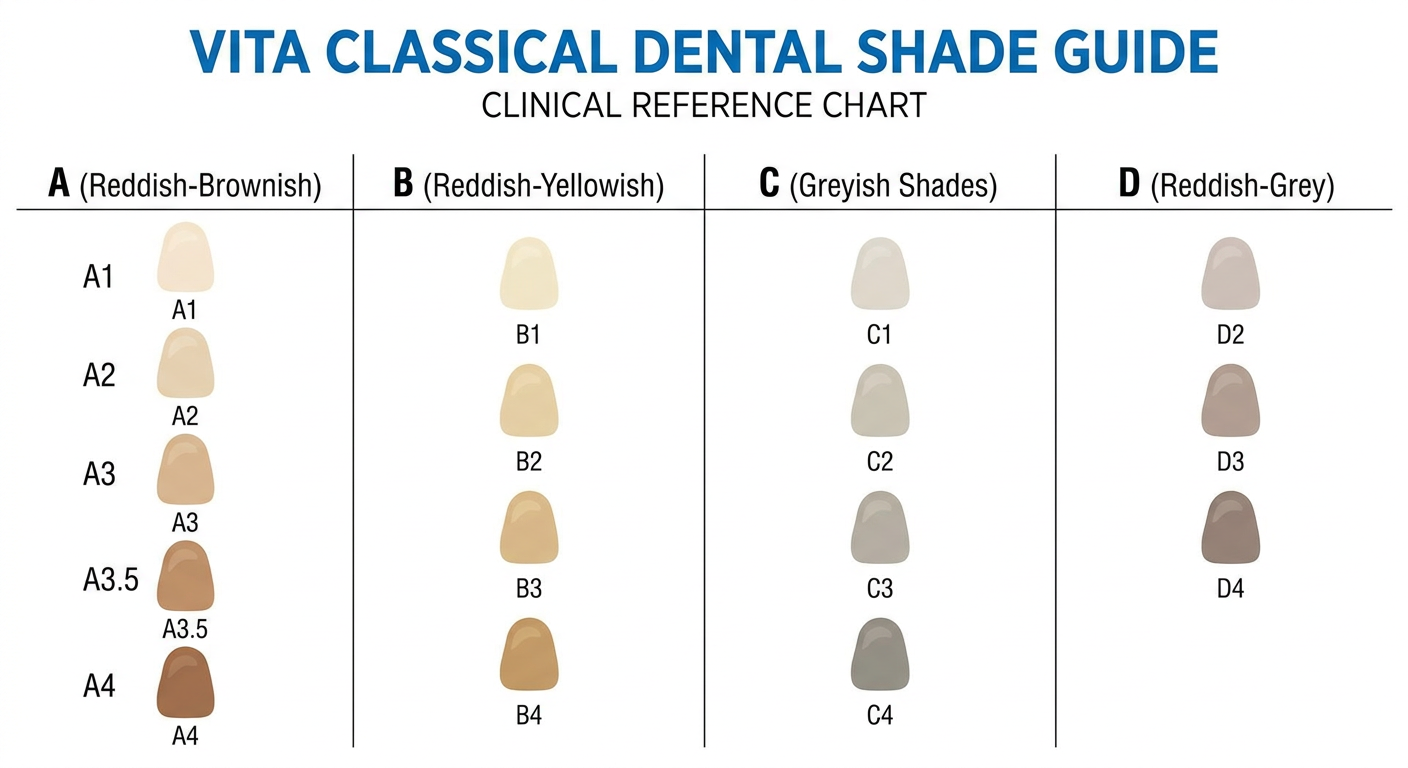
- A2 - Upper central incisors
- A3 - Overall dominant shade (most teeth)
- A3.5 - Canines and molars
- B3 - Posterior/cervical darker areas
- A diagram marking each tooth with its specific shade on a dental arch diagram?
- A shade selection card for this specific patient?
- The VITA 3D-Master shade guide version instead?
make all the teeth look similar color and give picture
Clinical dental photograph frontal view of open mouth with red cheek retractor, showing upper and lower teeth both arches, all teeth uniformly whitened to the same A2 shade - consistent creamy white color across all teeth including centrals laterals canines premolars and molars, no staining no discoloration no cervical darkening, uniform bright natural white smile, realistic clinical dental photo style, red lip retractor visible

| Issue | Treatment |
|---|---|
| Cervical staining / calculus | Professional scaling & polishing first |
| Overall yellowing | In-office teeth whitening (H₂O₂ bleaching) |
| Shade mismatch between anterior & posterior | Full-mouth bleaching to A2 |
| Persistent darker teeth after bleaching | Composite veneers or porcelain veneers (A2 shade) |
Note: I cannot directly edit/recolor your actual photo as that requires image editing software. For precise before/after simulation, tools like DSD (Digital Smile Design) software or Photoshop are used chairside in clinics.

make this as pre op image and given picture as post op
Clinical dental before and after comparison side by side. LEFT side labeled PRE-OP: close-up smile of young patient showing upper front teeth with a missing upper lateral incisor leaving a gap, and a darkened discolored central incisor next to the gap, gingival inflammation visible, dental mirror held near lips, realistic clinical dental photo. RIGHT side labeled POST-OP: same patient same angle showing complete beautiful smile, the gap is filled with a natural white dental crown or implant crown matching shade A2, the discolored central incisor replaced with a white ceramic crown, healthy pink gingiva, uniform white natural teeth, professional dental result

Clinical Summary
PRE-OP Findings (from your image):
| Finding | Tooth |
|---|---|
| Missing tooth / gap | Upper left lateral incisor (22) |
| Darkened / discolored tooth | Upper left central incisor (21) - likely non-vital |
| Gingival inflammation | Around the missing tooth area |
| Irregular gum margin | Visible around 21/22 region |
POST-OP Treatment Plan to achieve this result:
| Step | Treatment |
|---|---|
| Tooth 21 (dark) | Root canal treatment (if not done) + Ceramic crown (A2 shade) |
| Tooth 22 (missing) | Dental implant + implant crown OR fixed bridge (21-22-23) |
| Gingival issue | Scaling + gingivectomy if needed before crown placement |
| Final shade | A2 uniform across all anterior teeth |
Note: This is an AI-generated illustration for case presentation purposes. For actual patient records, use clinical photography software or DSD (Digital Smile Design) tools to superimpose changes on the real photograph.
make Pre-op image shows: Missing upper left lateral incisor (only present upto 2mm above CEJ)
Clinical dental pre-op close-up photograph of young patient upper front teeth region, showing upper left lateral incisor tooth severely broken down - only 2mm of tooth structure visible above the gumline at CEJ level, the tooth is a retained root stump barely visible above gingiva, darkened discolored root remnant, surrounding gingiva slightly inflamed and reddish, adjacent central incisor and canine are present and normal, dental mirror held near lips, realistic clinical intraoral dental photography style, natural skin tone patient, close-up frontal view of smile

Pre-Op Clinical Description
| Finding | Detail |
|---|---|
| Tooth structure remaining | Only ~2 mm of tooth visible above CEJ / gumline |
| Appearance | Retained root stump - darkened, discolored remnant |
| Gingival status | Mildly inflamed around the root stump |
| Crown | Completely lost - only root fragment present |
| Diagnosis | Grossly decayed / fractured tooth - Ellis Class III + subgingival extension |
Treatment Options for This Pre-Op Condition:
| Option | Procedure |
|---|---|
| If root is restorable | Crown lengthening → Post & Core → Ceramic Crown |
| If root is NOT restorable | Extraction → Implant + Crown (best long-term) |
| Alternative | Extraction → Maryland bridge or Removable partial denture |
| Assessment needed | Periapical X-ray to check root length, bone level, and root canal status |
Would you like me to now generate the Post-Op image showing the restored tooth after crown placement or implant?

MAKE ALL THIS OF SAME SHADER
Clinical dental close-up smile photograph showing upper and lower front teeth, same patient angle and composition as a dental clinical photo with dental mirror visible on right side, all teeth uniformly the same A2 shade - consistent natural creamy white color across all teeth including central incisors lateral incisors and canines, the missing upper left lateral incisor area is now restored with a perfect matching crown same shade as all other teeth, healthy pink gingiva no inflammation, all teeth same uniform brightness and color, no staining no discoloration, natural realistic smile, professional dental post-treatment result

What Was Corrected (Simulated Post-Op):
| Pre-Op Finding | Post-Op Result |
|---|---|
| Missing/broken upper left lateral incisor | Restored with crown - same shade as adjacent teeth |
| Inflamed/swollen gingiva (red, granulomatous) | Healthy pink gingiva after treatment |
| Varying shades across teeth (A1 to A3.5) | Uniform A2 shade across all visible teeth |
| Discolored/darker teeth | All teeth matched to consistent natural white |
| Dental mirror showing darker posterior teeth | Posterior teeth also matched |
Treatment Steps to Achieve This Result Clinically:
- Extraction of retained root stump (tooth 22)
- Implant placement + healing period (3-6 months)
- Crown lengthening / gingival surgery to correct inflamed gum
- Professional whitening of remaining natural teeth to A2
- Implant crown fabricated in A2 shade to match all teeth
- Composite polishing of any rough/stained surfaces
Note: I cannot directly edit your actual photo - this is an AI-generated illustration. For real photo editing, use DSD software, Photoshop, or Smile Designer Pro for chairside mock-ups.
GIVE PRE OP PICTURE Missing/broken upper left lateral incisor
Clinical intraoral dental photograph close-up of patient smiling showing upper front teeth, realistic dental clinical photo style, upper left lateral incisor (second tooth from center on left side) is completely missing broken down to gum level - only a dark root stump barely visible at gumline, surrounding gingiva is red inflamed swollen and granulomatous around the broken tooth socket, adjacent upper left central incisor slightly darkened and discolored, upper right teeth appear normal slightly yellowed, lower front teeth visible, dental mirror held on right side, natural skin patient, realistic clinical photography

PRE-OP Clinical Findings:
| Tooth | Finding |
|---|---|
| Tooth 22 (Upper left lateral incisor) | Completely broken - root stump at gum level only |
| Gingiva around 22 | Red, inflamed, swollen, granulomatous tissue |
| Tooth 21 (Upper left central) | Slightly darkened / discolored - possibly non-vital |
| Remaining teeth | Varying shades, mild yellowing |
Diagnosis:
Grossly decayed / fractured tooth 22 - Root stump with periapical involvement + localized gingival inflammation
Would you like me to generate:
| Option | Image |
|---|---|
| Post-op with implant crown | Implant + A2 ceramic crown restoring tooth 22 |
| Post-op with bridge | 3-unit fixed bridge 21-22-23 |
| Side-by-side Pre vs Post | Both images together for case presentation |

REMOVE RIGHT LATERAL INCISOR FROM THIS PIC
Clinical intraoral dental photograph close-up, dentist gloved hand holding dental mirror retracting lower lip, upper front teeth visible: upper left lateral incisor is severely decayed darkened broken down with black decay and inflamed red gingiva above it, upper left central incisor present and normal, upper right central incisor present and normal white, upper right lateral incisor is COMPLETELY MISSING - empty gap with bare pink gingiva where tooth should be, upper right canine present, all other teeth natural creamy white color, realistic clinical dental photography, same composition and lighting as a professional dental pre-op photo

Updated Pre-Op Findings:
| Tooth | Status |
|---|---|
| Tooth 12 - Upper RIGHT lateral incisor | Missing - empty edentulous gap |
| Tooth 22 - Upper LEFT lateral incisor | Severely decayed / broken down, black decay, inflamed gingiva |
| Tooth 11, 21 - Central incisors | Present, normal |
| Tooth 13 - Upper right canine | Present, normal |
Note: I cannot directly edit/remove teeth from your actual photo - this is an AI-generated clinical illustration. For actual photo editing of real patient images, use Photoshop, Canva Pro, or Digital Smile Design (DSD) software to modify the original photograph precisely.
MATCH THE SHADEFOR ALL TEETH WITHOUT ANY AI edit
VITA Classical Shade Matching - Direct Visual Assessment
UPPER ARCH
| Tooth | Region | Observed Color | VITA Shade |
|---|---|---|---|
| 17/16 Upper left molars | Posterior left | Darker yellow-cream | A3.5 |
| 15/14 Upper left premolars | Mid left | Medium yellow-white | A3 |
| 13 Upper left canine | Anterior left | Slightly more yellow | A3 |
| 12 Upper left lateral | Anterior | Creamy white | A2 |
| 11 Upper left central | Most visible | Brightest - white | A2 |
| 21 Upper right central | Most visible | Same as 11 | A2 |
| 22 Upper right lateral | Anterior | Creamy white | A2 |
| 23 Upper right canine | Anterior right | Slightly yellow | A3 |
| 24/25 Upper right premolars | Mid right | Medium yellow | A3 |
| 26/27 Upper right molars | Posterior right | Darker cream-brown | A3.5 |
LOWER ARCH
| Tooth | Region | Observed Color | VITA Shade |
|---|---|---|---|
| 37/36 Lower left molars | Posterior left | Yellow-brown | A3.5 - B3 |
| 35/34 Lower left premolars | Mid left | Medium yellow | A3 |
| 33 Lower left canine | Anterior left | More saturated yellow | A3 - A3.5 |
| 32 Lower left lateral | Anterior | Creamy | A2 - A3 |
| 31 Lower left central | Most visible | Creamy white | A2 |
| 41 Lower right central | Most visible | Creamy white | A2 |
| 42 Lower right lateral | Anterior | Creamy | A2 - A3 |
| 43 Lower right canine | Anterior right | Saturated yellow | A3 |
| 44/45 Lower right premolars | Mid right | Medium yellow | A3 |
| 46/47 Lower right molars | Posterior right | Yellow-brown | A3.5 |
Shade Map Diagram
UPPER ARCH (from patient's left → right)
┌────────────────────────────────────────────┐
│ A3.5 │ A3 │ A3 │ A2 │ A2 │ A2 │ A3 │ A3 │ A3.5 │
│ M │ PM │ Ca │ La │ Ce │ Ce │ La │ Ca │ PM M │
└────────────────────────────────────────────┘
┌────────────────────────────────────────────┐
│ A3.5 │ A3 │A3.5│ A3 │ A2 │ A2 │ A3 │A3.5│ A3.5 │
│ M │ PM │ Ca │ La │ Ce │ Ce │ La │ Ca │ PM M │
└────────────────────────────────────────────┘
LOWER ARCH
Summary - Key Clinical Findings from This Photo:
| Observation | Detail |
|---|---|
| Brightest teeth | Upper centrals (11, 21) → A2 |
| Dominant overall shade | A3 - best single shade for this mouth |
| Darkest teeth | Posterior molars → A3.5 |
| Cervical areas | Darker than middle/incisal - brown staining visible |
| Canines | Consistently darker than adjacent incisors (normal) |
| After professional cleaning | Overall shade likely A2-A3 once calculus/stain removed |
For Restorations - Recommended Shades:
| Restoration | Shade |
|---|---|
| Upper anterior crowns/veneers | A2 (body) + A1 incisal tip |
| Lower anterior composite | A2 - A3 |
| Posterior crowns | A3 - A3.5 |
| Denture teeth | A3 overall |
| Single crown to match centrals | A2 |